


Rossana Cantanhede Farias de Vasconcelos1; Karla Azuaga2; Géssica Cantadori Funes Arenas3; João Guilherme Finizola de Vasconcelos4; Natalie Schnaider Borelli5
Keywords: ALOPECIA; PLATELET-RICH PLASMA; DERMATOLOGY
Androgenetic alopecia (AGA) affects men and women and is the most common alopecia in both genders. It is known that its onset is associated with age and gender, being slightly less frequent in individuals of Asian and African heritage. It can start at any age after puberty, and by age 70 affects up to 80% of men and 40% of women (of the Caucasian race), with a gradual increase in incidence occurring with age. 1,2
It is characterized by changes in the hair growth cycle leading to progressive follicular miniaturization, with the transformation of terminal hairs into vellus and the production of shorter, thinner, and less pigmented hair shafts.3
It is known that each follicle has an individual control mechanism dictated by various substances, such as hormones, cytokines, growth factors, and environmental influences.3
Its pathogenesis is multifactorial, with a genetic predisposition of polygenic inheritance. Testosterone is the most powerful circulating androgen, with higher concentrations in men. In the region of the follicular dermal papilla, the 5-alfaredutase type-II enzyme promotes the conversion of testosterone into its metabolite dihydrotestosterone (DHT), which in turn promotes the shortening of the anagen phase, an increase in the percentage of telogens, the miniaturization of follicles and the development of AGA. Its affinity for androgen receptors is five times greater than that of testosterone. 2,3
The 5α-reductase is present in higher levels and increased activity in the scalp follicles of affected individuals. In addition, its levels are higher in the frontal follicles as compared to occipital follicles of women and men with AGA. In female's AGA, there is greater complexity regarding its etiopathogeny, since not all cases present a clear response to anti-androgens. The clinical features of male and female AGA also differ. 2,3
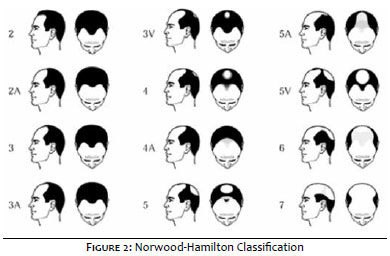
Clinically, there is a variable thinning of hairs of the frontoparietal, vertex, and bitemporal region, with the occipital region usually appearing normal. In order to characterize these different clinical patterns, two distinct classifications were implemented for each type of alopecia: the Ludwig classification for women and the Hamilton-Norwood classification for men. 4 (Figures 1 and 2)
Regarding diagnosis, there is no gold standard for AGA. In addition to a physical examination focusing on the pattern and degree of alopecia involvement, it is essential to carry out full anamnesis in order to rule out other causes. Dermoscopy is a quick and noninvasive examination, able to provide important data for diagnosis. The main alterations are: decrease in capillary density, yellow dots, variance in the diameter of hairs (which corresponds to the miniaturization of the hair follicles, and an increased number of vellus. 2,3
The treatment of AGA has at least four basic objectives: to prevent the progression of the alopecia, to stabilize the miniaturization process, to reverse the miniaturization process, and to increase hair density.4 Standardized photographic documentation from the beginning of treatment as well as during the follow-up period allows for appropriate therapeutic decision making by both the physician and the patient. 3
Although many medications have been launched for the treatment of AGA, only a few have endured the test of time. Among these, two stand out by presenting more evidence of results: the oral Finasteride and the topical Minoxidil, both requiring continuous use in order to obtain satisfactory results, with none of them restoring hair loss completely. 2-4
Encouraging the study of these aspects and the search for new knowledge is of paramount importance given the high prevalence of this disorder and the psychosocial impairment it entails.
The role of platelets in hemostasis is well known, nevertheless the use of platelets as a vehicle for storage and transport of cellular signals is a new concept. 5
The platelet-rich plasma (PRP) is a product derived from laboratory processing of autologous blood collected in the preoperative period, processed for concentration of platelets, and which is rich in growth factors that are released from alpha granules contained within the platelets after platelet activation. All protein load is released within 48 hours. Due to the fact it is autogenous, it is an organic, non-toxic, and non-immunoreactive product. 6-8
Assuming the influence of platelets in the hemostasis processes, the purpose of using PRP is to accelerate tissue regeneration starting from the endothelial lesion, inflammatory processes with the presence of macrophages and neutrophils, and regeneration and healing processes, where there is a presence of growth factors derived from the platelets that cause cell proliferation and differentiation up until the complete repair and regeneration of the damaged tissue. 5
The technique was first used in dentistry and later in orthopedics, with scientifically proven benefits. Currently there are other areas of application of PRP, for example, in the treatment of photoaging, 9 hair implant, 10-12 diabetic foot, 13,14 plastic surgery, 15-17 or simply to promote angiogenesis in tissues with poor vascularization or impaired circulation. 14, 18-24
In the present study the authors will evaluate the effect of PRP in patients with an androgenetic alopecia picture.
The objective of the present study is to assess hair growth through cell stimulation performed with subcutaneous applications of PRP in the affected regions. No additional treatment was associated in order to allow the assessment of the response of isolated PRP in patients with various degrees of AGA.
Eighteen volunteer individuals were selected, men and women between the ages of 18 to 60 years. The exclusion criteria were: patients with hormone disorders, nutritional deficiency, anemia, psoriasis, autoimmune disease, diabetics, pregnant women, nursing mothers, patients on anticoagulants, and use of oral isotretinoin.
The patients underwent an anamnesis conducted by the responsible physician, with the request of laboratory tests such as: complete blood count, serum iron, ferritin, zinc, TSH, free T4, ANA and fasting glucose, for evaluation and selection of individuals.
All project participants signed a free and informed term of consent in which all steps of the study, guidelines, and possible side effects were explained. An authorization form for the disclosure of results and photographs in the media was also signed. The project proposal was sent to an Ethics Committee and was approved under the protocol CAAE 25086613. 4. 0000 0081.
All procedures, such as assessments, PRP preparation, and injections were performed at the Instituto de Terapia Celular Aplicada - ITCA (Applied Cell Therapy Institute), a private practice involved in the research project, in conjunction with the study team, physicians, and a biologist.
The PRP was processed by the biologist responsible for the research, according to the protocol registered as Protocolo Cantadori (Reg. 508. 102 - Biblioteca Nacional do RJ - Rio de Janeiro National Library) and in compliance with all biosafety and asepsis standards.
Three applications have been programmed PRP with 21 days of interval. In all sessions, the volunteers underwent the process of having blood collected for the PRP preparation and injections in the affected areas immediately after. The procedure had an average duration of 90 minutes per patient, always with the supervision of the biologist and the physician in charge of the project.
The infiltrations were carried out by the physician in charge of the experiment, with sterile material and 26G x ½ needles. PRP was administered intradermally at a dose of 0.2 ml of on each point of the affected region, with spaces of approximately 2 cm between these points. The volume of processed PRP was individualized according to the size of the area to be treated in each patient.
The volunteers were evaluated through photographs and dermoscopy - both carried out before the treatment and before each session. Thirty days after the end of the third application, the patients returned for new photographic and dermoscopic records, having answered a questionnaire containing a satisfaction scale for the treatment, and for the final evaluation of the project.
Of the 18 patients treated, one dropped out after the first application, and another did not return for the final records.
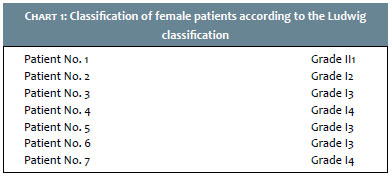
Among the seven women in the group, the AGA classification (according to the Ludwig scale) fell between GI2 and GII1. (Chart 1)
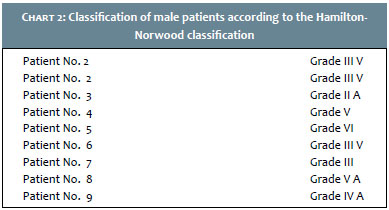
In the nine men, grades ranged from GIIA to GVI, according to Norwood-Hamilton classification. (Chart 2)
All patients were assessed after the end of the application by the patient himself or herself and by an external observer through photographic records, in addition to the pre- and posttreatment dermoscopic analysis.
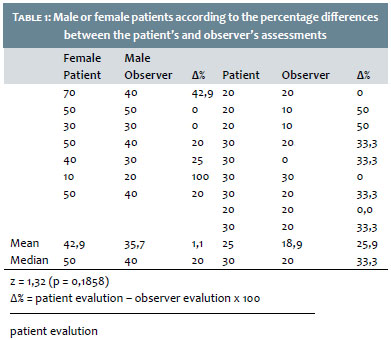
The results are shown in Table 1.
All patients showed some degree of improvement both in his or her own assessment and in the external observer's evaluation. (Figures 3 to 6)
Chart 3 shows the patients' degree of improvement regardless of gender.
1. The Mann-Whitney test25 was applied in order to compare the female or male patients regarding the differences in percentages (Δ%) observed between the patients' own evaluations and those of the external observer (Chart 1). For calculating the values of Δ%, the following formula was applied:
1. The Wilcoxon test25 was used in order to compare the evaluation scores (%) of each patient and the observer regarding the degree of improvement. This test was applied regardless of the patient's gender (Chart 2). As can be seen, in the women's group the average improvement was 42.85% in the evaluation of the patients themselves, while for the external observer it was 35.71%. In the men's group, the average improvement according to the patients was 25.55%, while for the external observer it was 18. 88%. The percentage of improvement in all patients was 33.12% according to the patients, and 26.25% for the external observer.
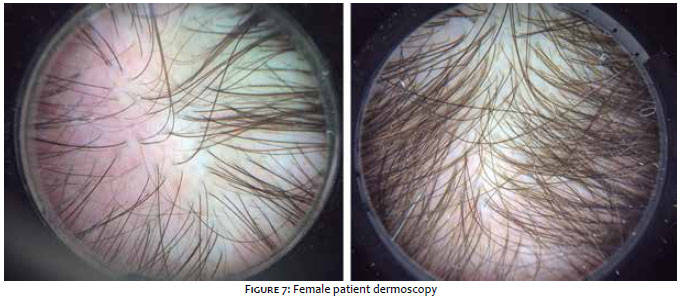
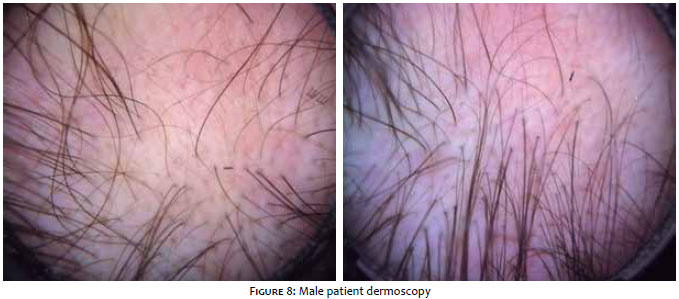
From the dermoscopy, the following alterations were observed: thickening of the hair shafts, improvement of local circulation, and an increased number of hair follicles (Figures 7 and 8).
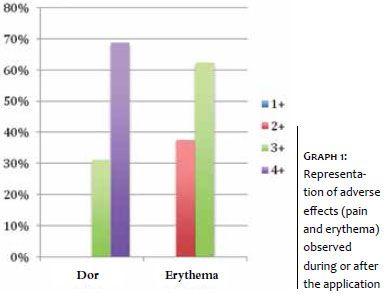
Regarding adverse effects, only local pain at the time of the application was reported by all patients. Two patients had persistent pain for two days, one patient reported a headache picture one day after the application, and the other 12 patients reported improvement in pain a few hours after the procedure. Also, an erythematous halo was also observed at the point of injection, with an absence of cases of local hematoma. The pain and erythema were classified according to a scale ranging from 1+ to 4+ (maximum) and are depicted in Graph 1:
No other symptoms or adverse effects were reported by the patients.
Growth factors can act as mitogenic agents - enhancing the proliferation of certain cell types or morphogenic agents - thereby altering the cellular phenotype. PRP specific studies identify a complete list of growth factors, including PDGF, FGF, TGF, IGF, EGF, and VEGF. 6-8
For cases of alopecia there are studies showing the PRP efficiency in hair growth. In his thesis on the application of PRP in hair micro-implant surgeries, Mates 26 verified the effectiveness of growth factors in hair density and growth, rapid decrease of apoptosis, and using angiogenesis, he succeeded in stimulating new and efficient mitoses for the resumption of the new anagen phase, thus acting as an accelerator of the regeneration and tissular remodeling in several lesion types.
Based on the scientific evidence of the reported effects of PRP, the authors of the present study proposed to evaluate the isolated response from the PRP in AGA cases. As stated, all patients showed some degree of improvement, resulting in an average of 33%. Statistical analysis also showed that the percentages of satisfaction informed by the patients were significantly higher than those observed by the external observer (p = 0.0072). This fact was aligned with the positive answer of most patients when asked if they would undergo additional sessions of the procedure for better results. Regarding adverse effects, the complaint of all patients was pain at the time of the application, with resolution within a few hours.
Regarding the changes observed through dermoscopy in the present study, an improvement in local circulation, improved miniaturization, and increased follicles could be observed. Those findings were in line with an article published in 2013, which evaluated the action of PRP in the hair follicle, revealing a significant difference in the number of new follicles in the treated area. 27
In the treatments already recommended for AGA, pharmacological measures differ between men and women. 1, 4 Uneven results were observed between the genders in the present study, with a clearer and more satisfactory response in the female group (mean = 42.9%) as compared to the men's (mean = 25.6%).
Although the etiologies of male and female AGA are different, the follicular alteration appears to be similar, with the presence of follicular miniaturization. In women, however, the hormonal interference is uncertain and it is suspected that other hormones, such as estrogen and prolactin, may be involved. 2, 3
The authors have questioned whether this difference found in the present study's results could be simply attributed to the lower androgen influence or the picture's clinical stage regarding the male volunteers., as has been described by JM Pereira et al.. 28
Regarding side effects, the authors observed only pain and erythema, with spontaneous regression. Published studies also show that the biological action of growth factors only accelerates the entire process of regeneration and recovery, without posing any carcinogenic potential. 29 A study conducted in 2009 aimed at treating a basal cell carcinoma in a 54-year-old patient showed a possible regression in the tumor's stage after treatment with PRP. 29
According to the literature, the PRP's growth factors act as mediators in cell maturation and are responsible for the tissue damage repair processes. They have an important angiogenesis action, increasing the local microcirculatory process and activating various cell groups in the integration and vitality of tissues. 26, 30,31
The fundamental objectives in the treatment of AGA are to increase the scalp's coverage and to slow down the progression of the loss of hair. In addition, explaining the condition's mechanisms to the patient and managing their expectations with the therapy is critical for treatment adherence.
According to the Brazilian Society of Dermatology, alopecia complaints are among the ten most frequent received by dermatology practices from patients of 15 to 39 years of age. 3 Despite this high frequency and the already available therapeutic measures, satisfactory treatment of AGA remains a challenge for the dermatologist. Thus, although there are many studies on the subject, scientific studies that demonstrate new therapeutic options become relevant.
In this study, the authors found an efficient and satisfactory response with the technique of PRP injection, even as an isolated therapy. It is known that in AGA the action of DHT is important for triggering the picture, and treatments that act on that front are required. As the PRP does not have this action, it emerges as an important measure in the association with androgenetic blockage therapies for the maintenance and improvement of the therapeutic response.
Based on the literature review and the results of the present study, this method offers an interesting alternative for the treatment of AGA, which suggests the availability of an effective option to associate with the existing ones in order to improve the therapeutic results of AGA.
1. Sampaio SAP, Rivitti EA. Dermatologia Básica. 3a ed São Paulo: Artes Médicas; 2007. p .432-34.
2. Torres F, Tosti A. Atlas de Doenças do Cabelo. Rio de Janeiro: Revinter; 2013. p .13-63.
3. Brenner-Mulinari F, Seidel G, Hepp T. Entendendo a alopecia androgenética. Surg Cosmet Dermatol. 2011;3(4): 329-37.
4. Junior WB, Chiacchio ND, Criado PR. Tratado de Dermatologia. São Paulo: Atheneu: 2010. p.984-99
5. Pontual MAB, Magini RS. Plasma Rico em Plaquetas PRP e Fatores de Crescimento das Pesquisas Científicas à Clínica Odontológica. São Paulo: Ed.Santos; 2004. p .163-87.
6. Lieberman J, Daluiski A, Einhorn TA. The Role of Growth Factors in the Repair of Bone. Biology and Clinical Applications. Investigation performed at the Department of Orthopaedic Surgery, University of California at Los Angeles Medical Center, Los Angeles, California, and the Department of Orthopaedic Surgery, Boston University Medical Center, Boston, Massachuset. J Bone Joint Surg Am. 2002;84(6):1032-44.
7. Landesberg R, Roy M. Glickman RS. Quantification of Growth Factor Levels Using a Simplified Method of Platelet-Rich Plasma Gel Preparation. J Oral Maxillofac Surg. 2000;58(3):297-300
8. Sierra ALP, Aranegui RO, Ares MM, Martínez JLQ, González JMM. Quantiication of growth factors by using a new system for obtaining platelet-rich plasma. Med Oral Patol Oral Cir Bucal. 2011;16(4): 614-8.
9. Redaelli A, Romano D, Marciàno A. Face and Neck Revitalizaton with Platelets - Rich Plasma (PRP). Clinical Outcome in a series of 23 Consecutively Treated Patients. J Drugs Dermatol.2010;9(5):466-72
10. Uebel CO. Ação do plasma rico em plaquetas e seus fatores de crescimento na cirurgia dos microimplantes capilares [tese]. Porto Alegre: PUCRS, 2006.
11. Li ZJ, Choi HI, Choi DK, Sohn KC, Im M, Seo YJ, et al. Autologous platelet-rich plasma: a potential therapeutic tool for promoting hair growth. Department of Dermatology, School of Medicine, Chungnam National University, Daejeon, Korea. Dermatol Surg. 2012;38(7):1040-6
12. Takikawa M, Nakamura S, Nakamura S, Ishirara M, Kishimoto S, Sasaki K, et al. Enhanced Effect of Platelet-Rich Plasma Containing a New Carrier on Hair Growth. Dermatol Surg. 2011;37(12):1721-9.
13. Bennett SP, Griffiths GD, Schor AM, Leese GP, Schor SL. Growth factors in the treatment of diabetic foot ulcers. J Surg. 2003;90(2):133-46.
14. Buza PW. Combination Platelet Leukocyte Rich Plasma (PLRP/PRP) and Hyperbaric Systemic Oxygenation (HBO) is Safe and Effective in the Treatment of Refractory Wounds. 2003, 2-13 Não localizei publicação!
15. Cervelli V, Palla L, Pascali M, Angeli B de, Curcio BC, Gentile P. Autologous Platelet-Rich Plasma Mixed with Purified . Fat Graft in Aesthetic Plastic Surgery . Aesth Plast Surg. 2009,33(5):716-21.
16. Clevens RA . Autologous Platelet Rich Plasma in Facial Plastic Surgery. Proceedings. 8th International Symposium of Facial Plastic Surgery. NewYork city, USA. Center for Facial Cosmetic Surgery - Melbourne, FL. 2002, May; 1-5.
17. Sclafani AP, McCormick AS . Induction of Dermal Collagenesis, Angiogenesis, and Adipogenesis in Human Skin by Injection of Platelet-Rich Fibrin Matrix. Arch Facial Plast Surg. 2012;14(2):132-6.
18. Roy S, Driggs J, Elgharably H, Biswas S, Findley M, Khanna S, et al. Platelet-rich fibrin matrix improves wound angiogenesis via inducing endothelial cell proliferation. Wound Rep Reg. 2011;19(6):753-66.
19. Peerbooms JC, Sluimer J, Bruijn DJ, Gosens T. Positive Effect of an Autologous Platelet Concentrate in Lateral Epicondylitis in a Double-Blind. Randomized Controlled Trial: Platelet-Rich Plasma Versus Corticosteroid Injection With a 1-Year. Am J Sports Med. 2010;38(2):255-62.
20. Asahara T, Bauters C, Zheng LP, Takeshita S, Bunting S, Ferrara N, et al. Synergistic Effect of Vascular Endothelial Growth Factor and Basic Fibroblast Growth Factor on Angiogenesis in Vivo. Circulation. 1995;92(9 Suppl):II365-71.
21. Matsui M, Tabata T. Enhanced Angiogenesis by Multiple Release of Platelet-Rich Plasma Contents and Basic Fibroblast Growth Factor from Gelatin Hydrogels. Acta Biomaterialia. 2012;8:1792-1801.
22. Anitua E, Sánchez M, Zalduendo MM, Fuente M de La, Prado R, Orive GI, et al. Fibroblastic response to treatment with different preparations rich in growth factors. Cell Prolif;. 2009;42(2):162-70.
23. Yoshikawa T, Tohyama H, Katsura T, Kondo E, Kotani Y, Matsumoto H, et al. Effects of Local Administration of Vascular Endothelial Growth Factor on Mechanical Characteristics of the Semitendinosus Tendon Graft After Anterior Cruciate Ligament Reconstruction in Sheep. Department of Sports Medicine, Hokkaido University School of Medicine, Sapporo, Japan, the Department of Orthopaedic Surgery, Keio University School of Medicine, Tokyo, Japan, and the Department of Orthopaedic Surgery, Hokkaido University School of Medicine, Sapporo, Japan. Am J Sports Med. 2006;34(12):1918-25.
24. Vang SN, Brady CP, Christensen KA, Allen KR, Anderson J E, Isler JR, et al. Autologous Platelet Gel in Coronary Artery Bypass Grafting: Effects on Surgical Wound Healing. J Extra Corpor Technol. 2007;39(1):31-8.
25. Siegel SE, Castellan JR, NJ. Estatística não paramétrica para ciências do comportamento. 2ª ed. Porto Alegre: Artmed; 2006. p .448
26. Mates PC. Plasma rico em plaquetas e seus fatores de crescimento na cirurgia de microimplantes capilares. Curitiba: Universidade Tuiuti do Paraná; 2011.
27. Miao Y1, Sun YB, Sun XJ, Du BJ, Jiang JD, Hu ZQ. Promotional effect of platelet-rich plasma on hair follicle reconstitution in vivo. Dermatol Surg. 2013;39(12):1868-76.
28. Yoshitake T, Takaeda A, Ohki K, Inoue Y, Yamawaki T, Otsuka S, et al. Five-year efficacy of finasteride in 801 Japanese men with androgenetic alopecia. J Dermatol. 2015;42(1): 1-4.
29. Kleintjes WG. Treatment of basal cell carcinoma with autogenous growth factors and adipose-derived stem cells. Plast Reconstr Surg. 2010,;126(6):312-13.
30. Weinberg WC, Brown PD, Stetler-Stevenson WG, Yuspa SH. Growth factors specifically alter hair follicle cell proliferation and collagenolytic activity alone or in combination. Differentiation. 1990;45(3):168-78.
31. Vick VL, Holds JB, Hartstein ME, Rich RM, Davidson BR. Use of autologous platelet concentrate in blepharoplasty surgery. Ophthal Plast Reconstr Surg. 2006;22(2):102-4.
This study was performed at the Faculdade de Medicina da Universidade de Santo Amaro (Unisa) - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}