


Neide Kalil Gaspar1; Antonio Pedro Andrade Gaspar2; Marcia Kalil Aidê3
Keywords: TRICHLOROACETIC ACID; RHINOPHYMA; THERAPEUTICS.
Rhinophyma is a disfiguring and progressive disorder of the nasal skin, characterized by hyperplasia of the sebaceous glands with occlusion of the ducts and dermal fibrosis, typically affecting middle aged Caucasian men.
This process occurs most commonly in rosacea patients and can affect the frontal region (metophyma) or, more rarely, the ears (otophyma), eyelids (blepharophyma), or the mentum (gnatophyma).
Its development is progressive and deforming, and in some patients there can be intermittent inflammation, which may result in scars and fibrous tissue.
The process of removing hyperplastic tissue through incisional surgery,1-6, electrosurgery,7-8 or laser 5, 9-13 is always laborious, requiring efficient preparation by the dermatologist, and always presents a substantial risk of scarring.
The authors describe a method for treating rhinophyma that was developed by Gaspar NK five decades ago, and which has been performed in countless patients without any complications.
The present paper is aimed at demonstrating the applicability of this method.
No age, gender, or somatic disease restrictions were used in the selection of patients. This process is not indicated for the few patients with scarring and a xerotic and whitish appearance.
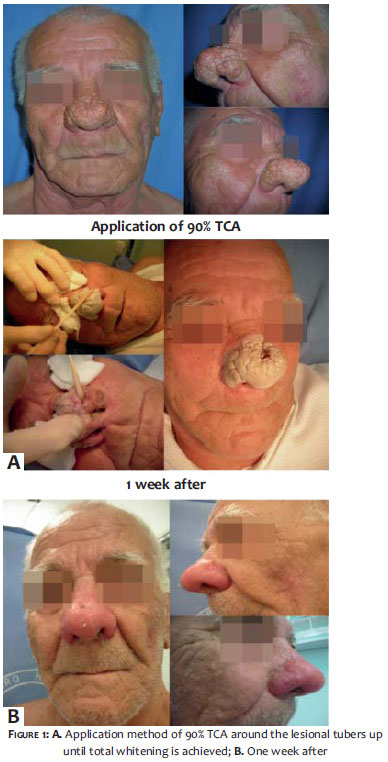
Patients should be warned beforehand that there will be a formation of thick and dark crusts, which will remain for 7 to 10 days but which should detach spontaneously and non-traumatically.
It is necessary to administer oral acyclovir to patients with a history of herpes simplex, and tetracycline and ibuprofen to those with a very intense inflammatory process. The emptying of the comedones is then carried out by vigorous expression in order to avoid inflammation underneath the crusts.
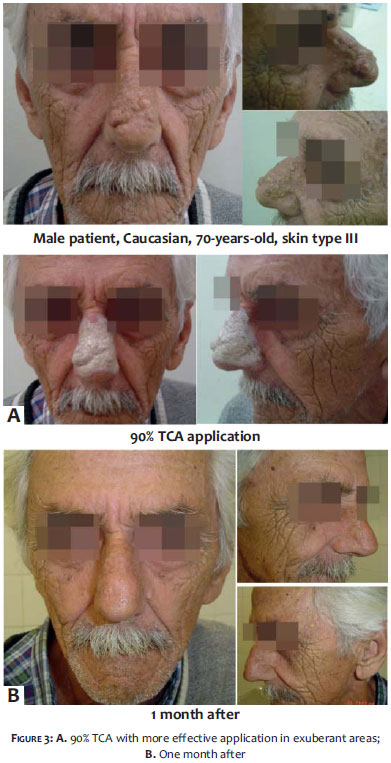
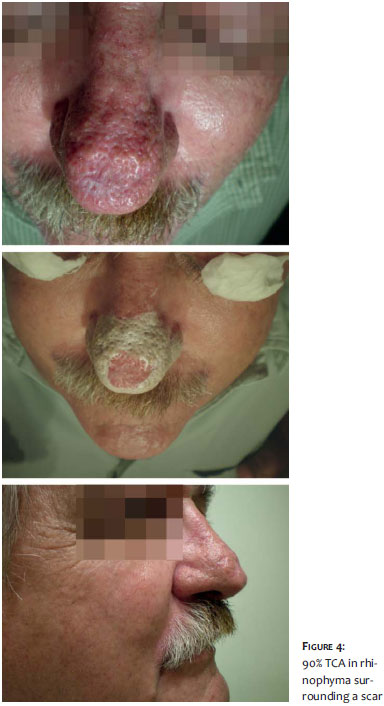
The procedure begins with removing all grease from the skin, using acetone immediately before, then evolving to the application of 70% or 90% trichloroacetic acid (TCA) with a stick wrapped in cotton (forming a flat swab) up until the total and intense local whitening of the area occurs, which happens a few seconds after the application (Figures 1 and 2). In very exuberant and hypertrophic lesions, the application must be more intense (2 or more times in a row) (Figure 3). The areas of normal skin or containing atrophic lesions should always be left untouched (Figure 4).
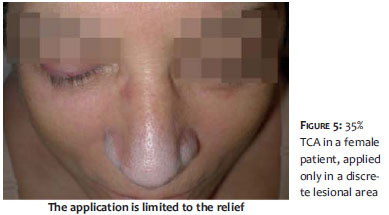
When the rhinophyma is partial, the treatment should cover only hypertrophic areas (Figure 5).
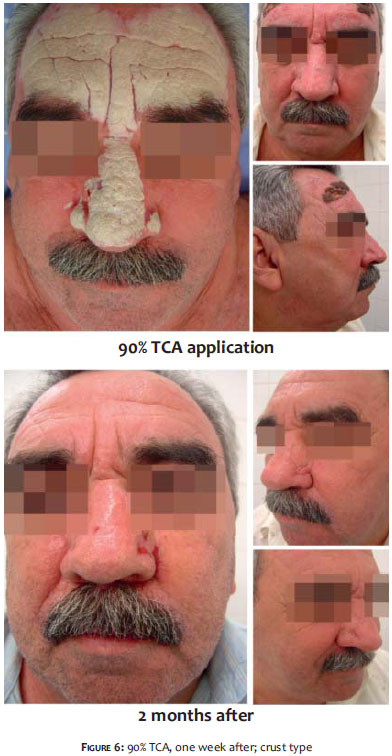
Lesions that reach other regions can also be treated immediately (Figure 6).
If a new application is necessary in the points where some hypertrophy remains, it can be performed as soon as the crusts come loose.
After 30-60 minutes the whitened appearance is replaced by a slight erythema.
Female patients often have very mild lesions and should be treated with a low TCA concentration (35%) in a single pass using the stick, which should not contain large amounts of acid (Figure 5).
Healing takes place within 7 to 10 days, after which the patient should use sunscreen in the region.
Almost all of the authors' patients achieved complete results with only one treatment session. No adverse effect has been observed in any of the treated patients, and most attended the return consultation with apparently higher self-esteem - which could even be noticed on their physiognomic aspects (Figure 7).
The procedure described in the present paper is simple, practical, cost-effective and requires no instrumental or special preparation of the patient, or special preparation by the dermatologist. The restriction of the procedure to "cicatricial" cases is due to the fact that TCA has no effect of reduction for that lesion type.
1. Wetzig T, Averbeck M, Simon JC, Kendler M. New rhinophyma severity index and mid-term results following shave excision of rhinophyma. Dermatology. 2013;227(1):31-6.
2. Sarifakioglu N, Sarifakioglu E. Simple, easy, and still effective treatment option in severe rhinophyma: shave and paste. Dermatol Ther. 2013;26(2):168-9.
3. Husein-ElAhmed H, Armijo-Lozano R. Management of severe rhinophyma with sculpting surgical decortication. Aesthetic Plast Surg. 2013;37(3):572-5.
4. Selig HF, Lumenta DB, Kamolz LP. The surgical treatment of rhinophyma-Complete excision and single-step reconstruction by use of a collagen- elastin matrix and an autologous non-meshed split-thickness skin graft. Int J Surg Case Rep. 2013;4(2):200-3.
5. Lazzeri D, Larcher L, Huemer GM, Riml S, Grassetti L, Pantaloni M, Li Q, Zhang YX, Spinelli G, Agostini T. Surgical correction of rhinophyma: comparison of two methods in a 15-year-long experience. J Craniomaxillofac Surg. 2013;41(5):429-36.
6. Faris C, Manjaly JG, Ismail-Koch H, Caldera S. Rapid treatment of rhinophyma with powered microdebrider. Case Rep Otolaryngol. 2013;2013:621639.
7. Wheble GA, Ahmed F, Pandya AN. Electro-rhinosculpture for the surgical management of rhinophyma. Ann R Coll Surg Engl. 2014;96(1):81.
8. Prado R, Funke A, Bingham J, Brown M, Ramsey Mellette J. Treatment of severe rhinophyma using scalpel excision and wire loop tip electrosurgery. Dermatol Surg. 2013;39(5):807-10.
9. Madan V, Ferguson JE, August PJ. Carbon dioxide laser treatment of rhinophyma: a review of 124 patients. Br J Dermatol. 2009;161(4):814-8.
10. Serowka KL, Saedi N, Dover JS, Zachary CB. Fractionated ablative carbon dioxide laser for the treatment of rhinophyma. Lasers Surg Med. 2014;46(1):8-12.
11. Corradino B, Di Lorenzo S, Moschella F. "Downward steps technique" with CO2 ultrapulsed laser for the treatment of rhinophyma: our protocol. Acta Chir Plast. 2013;55(1):16-8.
12. Singh S, Peterson JD, Friedman PM. Management of mild to moderate rhinophyma using ablative fractional photothermolysis. Dermatol Surg. 2013;39(7):1110-3.
13. Madan V, Ferguson JE, August PJ. Carbon dioxide laser treatment of rhinophyma: a review of 124 patients. Br J Dermatol. 2009;161(4):814-8.
This study was performed at the authors' private practices in Niterói (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}