


Ellem Tatiani de Souza Weimann1; Thaísa Saddi Tannous Silvino1; Lissa Sabino de Matos1; André Luiz Simião2; Adilson Costa3
Keywords: MELANOMA, EPIDEMIOLOGY, SKIN NEOPLASMS.
The incidence of skin cancer has increased worldwide in the last three decades. The propensity to develop skin cancer during one's lifetime is linked to both individual and environmental characteristics, including skin type and phenotype, family history of skin cancer, and level of exposure to ultraviolet radiation (UV), which is cumulative over a lifetime.1 Cutaneous melanoma is of significant relevance among malignant skin tumors, for despite its low incidence (3-4%) it has the highest mortality rate.
On a global scale, cutaneous melanoma is estimated to be between the 12th and 15th most commonly diagnosed cancers. However, in some developed countries, it is the first or second most frequent tumor in young adults. A high prevalence is observed in Australia and regions where the population is predominantly Caucasian or light-skinned. Low to intermediate levels are seen in Latin America, and the lowest rates are found in regions with a high population of Asian or African individuals.4 Between the years of 1998 and 2002, Sortino-Rachou (2011) found a total of 4,465 cases of melanoma reported in Latin America, corresponding to 1.2% of all cutaneous melanomas registered in CI5IX Data Base. The same author recorded the incidence of melanoma among inhabitants of Latin America as ranging from 1.1 and 6.5 cases/100,000 (4.6/100,000 inhabitants for females and 4.3/100,000 for females).5
In Brazil, estimates for the year 2014 are for 5,890 new melanoma cases (2,960 in men and 2,930 in women), totaling 10% of all neoplasias. For the Brazilian State of São Paulo, 830 new cases are estimated in male patients (incidence of 3.97 new cases/100,000) and 1,010 new cases in female patients (incidence of 4.59 cases/100,000), correlating to a serious public health problem.6 The present study was aimed at presenting epidemiological data related to melanoma skin cancer in a region of the city of Campinas (São Paulo State, Brazil), since there are few studies describing population data for specific regions of the country.
A cross-sectional, retrospective, descriptive study was carried out using secondary data from medical records of all patients diagnosed with melanoma, at the Dermatology Department of the Pontifícia Universidade de Campinas - PUC Campinas, São Paulo, Brazil.
The inclusion criterion was a diagnosis of melanoma with primary cutaneous neoplasia. Primary non-cutaneous melanoma was an exclusion criterion. Data were collected on age, gender, race, comorbidities, time since onset of the lesion, referral method, personal and family history, anatomic site of the primary lesion, histological type, Clark level, Breslow thickness, presence of mitosis, ulceration, and regression.
Descriptive analyses with study of frequency and percentage were carried out. For the quantitative variables, the measure of central tendency (mean) was calculated. Excel® was used to analyze the data. Due to the fact that the study is dependent on data obtained from patient records, it is subject to measurement and information bias. The study complied with the principles outlined in the Declaration of Helsinki.
The service identified 99 cases of melanoma that were receiving follow-up. Of the total, 29% (29 cases) were male and 71% (70 cases) were female. According to skin color, 78% (77) of the patients were light-skinned, 9% (9) were mixed and only 1% was dark-skinned. Twelve percent (12) of the patients did not have their skin color mentioned in the initial anamnesis.
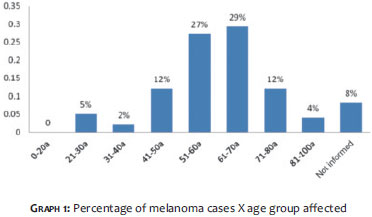
The mean age for the entire group was 61 years. The mean age by gender was 58 years for females and 59 for males. The distribution by age group shows a prevalence of cases in the 51 to 70 years group (56%), as shown in Graph 1.
When asked about the time of onset of the lesions, the patients either could not inform and/or this datum was not recorded (49% or 48 cases). Only 3 patients (3%) reported that the lesion was congenital, and once realizing a change in the pattern, were motivated to seek medical attention. Of the total, about 20% sought care within 1 year of identifying the lesion or perceiving a change in it. The lesion had been in place more than 3 years in 17% of cases and between 1 and 2 years in 11% of them.
In about 40% of recorded cases, there was no reference to how the patient had discovered the lesion (selfexamination/spontaneous, referral by healthcare professional, or expert assessment). Thus, in the present study, 42% of patients noticed their lesions and sought medical attention. Only 4% were referred by a health professional that had noticed a suspicious lesion. In 14% of cases the exeresis of the lesion was recommended by a specialized professional, and in 49% of patients there was no information about the form of referral to the service.
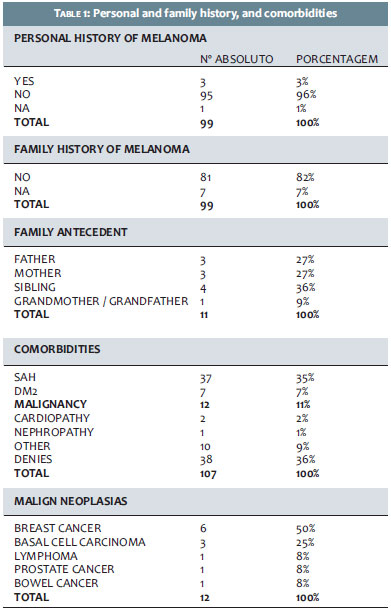
Table 1 below presents the epidemiological data of personal and family history, and the presence of comorbidities in the melanoma cases reported. It was observed that 96% of patients had no personal history of melanoma and 82% had no family history. Of the 11% with a positive family history, 54% had a family history linked to parents and 36% had a family history linked to siblings. The most prevalent comorbidity was Systemic Arterial Hypertension, present in 35% of cases. Of the 11% of patients who reported malignancy, breast cancer was the most prevalent, accounting for 50% of cases.
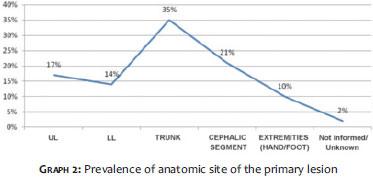
The prevalence of the primarily affected anatomical site is shown in Graph 2.
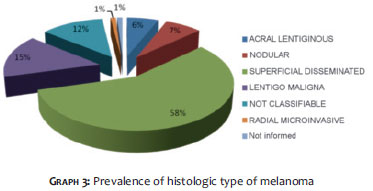
Regarding the histological type, the most prevalent in the dermatologic service in question was the superficial spreading melanoma (58%) as shown in Graph 3.
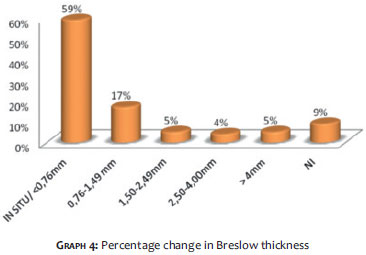
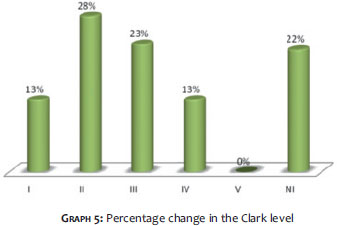
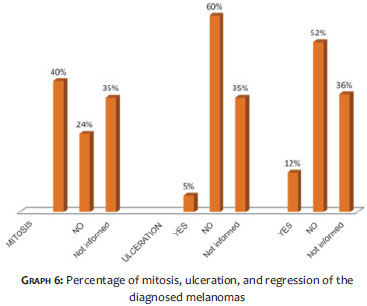
Graphs 4, 5, and 6 depict data on Breslow thickness, Clark level, and a presence/absence of mitosis, ulceration, and regression.
Melanoma is the cutaneous neoplasia with the worst prognosis, and therefore is a disease with a major impact on public health. It corresponds to approximately 5% of skin cancers and is responsible for roughly ¾ of deaths from that condition, a fact that makes its epidemiological knowledge of the utmost importance. 7
In the service in question, 29% of patients were male and 71% female. In a 30-year retrospective study carried out by Nasser (2011) in the city of Blumenau, in the southern Brazilian State of Santa Catarina, of the 1,002 cases of melanoma diagnosed, 44% were male and 56% female. 8 Another retrospective 20-year study conducted at a university hospital in Belo Horizonte, the capital of the southeastern Brazilian State of Minas Gerais, has shown that in a sample of 101 patients, 61% were female and 39% male. 9 As in the present analysis, those two studies also demonstrate a higher prevalence of the neoplasia in female patients - a trend that persists in most Brazilian studies. 10,11
In the present study, the average age of the sample was 61 (58 years for females and 59 for males). The distribution by age group shows a prevalence of cases in patients between 51 and 70 years old (56%). Unlike other malignancies, melanoma affects younger individuals, with an average age below that found in other types of tumors, as described by Brandão et al., who reported an average patient age of 55 years. 9 The mean age found in the present study is similar to that found in most studies conducted in Brazil and abroad, again confirming the trend of melanoma affecting patients at a younger age. 10,12_16
The predominant skin color on the present study was light-skinned (78%). Once again the present study was consistent with those carried out by Brandão et al., which revealed a prevalence of melanoma of 74% in light-skinned patients and 26% in darker-skinned patients. Another study by Pinheiro et al. also confirms a higher prevalence of melanoma in fair skin (87.5% versus 12.5% in darker skin). In the present study, the incidence found in non-Caucasian patients (10%) is higher than that found in the literature, 10, 11, 17, 18 as evidenced by Purim et al. (2013), who found a prevalence of only 0.18% in dark-skinned patients. 19
According to records, 96% of patients had no personal history of melanoma and 82% had no family history of melanoma. Of the 11% with a positive family history, 54% had parental history and 36% of cases had a history among siblings. In a study carried out at another university hospital in Brazil (Curitiba city, southern State of Paraná) 64.6% of patients had no history of skin cancer, however 24% of them described a family history of some type of skin cancer, not necessarily melanoma.19
In the present study, 42% of patients noticed their lesions on their own. Only 4% were referred by health professionals, for 14% of patients exeresis was recommended by a specialized professional, and in 49% of cases the form of referral to the service was not indicated. Almost half the cases are of patients who identified suspicious lesions on their own. This can be indicative of two scenarios: more well informed patients (awareness campaigns) or a lack of medical inspection of patients' skin. Maia & Basso (2006) reported that 54% of patients diagnosed with melanoma noticed the lesion themselves, while 24% were made aware by health professionals, and the remaining (22%) were made aware by spouses or others.20 In Brazil it is not known who typically first discovers the melanoma cases. This knowledge could serve as a basis for education programs of the public and of health professionals.
The most prevalent anatomic site for primary lesions was the trunk (35% of cases), followed by the cephalic region (21%), upper limbs (17%), lower limbs (14%), and hands/feet (10%). In the study by Brandão et al., the main affected site was the head and neck (30.7%), followed by the trunk (21.1%), acral region (19.3%), upper limbs (15.1%) and lower limbs (9.6%). The most affected anatomical sites tend to vary according to the patient's histological type and gender. Most studies show a greater involvement of the trunk in men and of the legs in women.12, 21-24
The most prevalent histological type in the service in question was the superficial spreading melanoma (58%), followed by lentigo maligna (15%), non-classifiable tumors/radial microinvasive (13%), nodular (7%), acral lentiginous (6 %), and uninformed (1%). International and Brazilian studies differ on the prevalence of histological type. There are reports of a prevalence of the extensive superficial type among Caucasians, 9, 25-27 and of the acral lentiginous type in non-Caucasians. 9,21,28 In the Brazilian literature, the authors also observed a variation in the histological type across different regions of the country, also with a predominance of the superficial spreading type where most of the population has fair skin. 9,29,30,31,32
The majority of the studied patients (59%) had melanoma in situ, 17% had a Breslow thickness of 0.76-1.5 mm, 5% with a thickness of 1.5-2.49mm, 4% with a thickness of 2.5-4.0 mm, and 5% had lesions greater than 4.0 mm. The data of the present study are similar to those reported by Pinheiro et al. (2003), in which there is evidence of a higher prevalence of Breslow thicknesses of less than 0.75 (42.3%), which may translate into specialists with a better ability to carry out early diagnoses, as this occurred in more developed countries. 29,30,33
Having a knowledge of the epidemiology of patients with melanoma in a given geographical region provides a better understanding of the disease, with evaluation of the prevalence and associated risk factors. This facilitates medical actions, with better-established strategies for primary and secondary prevention.
1. Lages RB, Barbosa PB, Almeida IP, Lopes LRS, Lopes Filho LL. Detecção precoce do câncer de pele: experiência de campanha de prevenção no Piauí- Brasil. Rev Bras Promoç Saúde. 2012;25(2): 221-7.
2. Rizzatti K, Schneider IJC, d'Orsi E. Perfil epidemiológico dos cidadãos de Florianópolis quanto à exposição solar. Epidemiol Serv Saúde. 2011.20(4):459-69.
3. Curado MP, Edwards B, Shin HR, Strom H, Ferlay J, Heanue M, et al. editors. Cancer incidence in five continents - volume IX. Lyon: IARC; 2007
4. de Vries E, Bray F, Coebergh JW, Cerroni L, Ruiter DJ, Elder DE. Melanocytic tumours. In: LeBoit PE, Burg G, Weedon D, Sarasin A, editors. Skin tumours. Lyon: IARC Press; 2006.
5. Sortino-Rachou Ana Maria, Curado Maria Paula, Cancela Marianna de Camargo. Cutaneous melanoma in Latin America: a population-based descriptive study. Cad. Saúde Pública. 2011;27( 3 ):565-72.
6. Instituto Nacional de Câncer José de Alencar Gomes da Silva [homepage na internet]. Tipos de Câncer: Pele: Melanoma. [acesso em 06/02/2014]. Disponível em: http://www2.inca.gov.br .
7. Diepgen TL, Mahler V. The epidemiology of skin câncer. Br J Dermatol. 2002;146(Suppl 61):1-6.
8. Naser, N. Melanoma cutâneo: estudo epidemiológico de 30 anos em cidade do sul do Brasil, de 1980-2009. An Bras Dermatol. 2011.86(5):932-41.
9. Brandão FV, Pereira AFJR, Gontijo B, Bittencourt FV. Epidemiological aspects of melanoma at a university hospital dermatology center over a period of 20 years. An Bras Dermatol. 2013;88(3):344-53.
10. Lucas EA, Deps PD, Lima JGB, Toriblo R, Gomes CC. Malignant Melanoma: retrospective study in the period 1982-1992, in the University Hospital of UFES. Arq Bras Med. 1994;68:67-70.
11. Ferrari Júnior, NM, Muller H, Ribeiro M, Maia M, Sanches Júnior JA. Cutaneous melanoma: descriptive epidemiological study. Sao Paulo Med. J. 2008;126(1):41-7.
12. Gon AS, Minelli L, Guembarovski AL. Melanoma cutâneo primário em Londrina. An Bras Dermatol. 2001;76(5):413-26
13. Borges SZ, Bakos L, Cartell A, Wagner M, Agostini A, Lersch E. Distribution of clinical-pathological types of cutaneous melanomas and mortality rate in the region of Passo Fundo, RS, Brazil. Int J Dermatol. 2007;46(7):679-86.
14. Chang AE, Karnell LH, Menck HR. The National Cancer Data Base report on cutaneous and noncutaneous melanoma: summary of 84,836 cases from the past deca- de. The American College of Surgeons Commission on Cancer and the American Cancer Society. Cancer.1998;83(8):1664-78.
15. Cabrera R, Silva S, Días de Medina J, Hoell I, Gugliemetti A, Rohmann I. Clinical study of 113 cases of malignant melanoma. Rev Med Chil. 1994;122:900-6
16. Buettner PG, Leiter U, Eigentler TK, Garbe C. Development of prognostic factors and survival in cutaneous melanoma over 25 Years. An analysis of the Central Malignant Melanoma Registry of the German Dermatological Society. Cancer. 2005;103(3):616-24.
17. Fernandes NC, Cardoso ICL, Maceira J, Perez M. Melanoma: estudo retrospectivo de 47 casos. An Bras Dermatol. 1996;71(4):381-85.
18. Fernandes NC, Calmon R, Maceira JP, Cuzzi T, Silva CSC. Melanoma cutâneo: estudo prospectivo de 65 casos. An Bras Dermatol. 2005;80(1):25-34.
19. Purim KSM, Sandri CO, Pinto NT, Sousa RHS, Maluf EPC. Perfil de Casos de Melanoma em um Hospital Universitário, 2003 à 2007. Rev Bras Cancerologia. 2013;59(2):193-9.
20. Maia M, Basso M. Quem descobre o melanoma cutâneo. An. Bras. Dermatol. 2006.81(3):244-8.
21. Paek SC, Sober AJ, Tsao HT, Mihm Jr MC, Johnson TM. Cutaneous melanoma. In: Wolf K, Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, editors. Fitzpatrick's Dermatology in general medicine. New York: Mc Graw Hill; 2008. p.1134-57.
22. Bernardi CDV, Favaretto AL, Brancher MC, Ponzio HA. Freqüência de melanoma maligno no Serviço de Dermatologia da ISCMPA/UFRGS. [Rate of malignant melanoma in Service of Dermatology of ISCMPA/UFRGS]. An Bras Dermatol. 1998;73(Supl 1):8.
23. Criado PR, Vasconcellos C, Sittart JAS, et al. Melanoma maligno cutâneo primário: estudo retrospectivo de 1963 a 1997 no Hospital do Servidor Público Estadual de São Paulo. Rev Assoc Med Bras (1992). 1999;45(2):157-62.
24. Venegas LFP, Flores C, Blacher GG, Daudt AW, Cerski CTS. Melanoma maligno cutâneo no Rio Grande do Sul: estudo de 101 casos. Rev Assoc Med Bras (1992). 1992;38(3):122-6.
25. Cabrera R, Silva S, Días de Medina J, Hoell I, Gugliemetti A,Rohmann I. Clinical Study of 113 cases of malignant melanoma. Rev Med Chil. 1994;122:900-6.
26. Loria D, Matos E. Risk factors for cutaneous melanoma: a case-control study in Argentina.Int J Dermatol. 2001;40(2):108-14.
27. Garbe C, Mmleod GR, Buettner PG. Time trends of cutaneous melanoma in Queensland, Australia and Central Europe. Cancer. 2000;89(6):1269-78.
28. Cress RD, Holly EA. Incidence of cutaneous melanoma among no-Hispanic Whites, Hispanics, Asians, and Blacks: analysis of California Cancer Registry data, 1988-93.Cancer Causes Control. 1997;8(2):246-52.
29. Bakos L, Wagner M, Bakos R, Leite CSM, Sperhacke CL, Dzekaniak KS, et al. Sunburn, sunscreen, and phenotypes: some risk factors for cutaneous melanoma in southern Brazil. Int J Dermatol. 2002;41(9):557-62.
30. Borges SZ, Bakos L, Cartell A, Wagner M, Agostini A, Lersch E. Distribution of clinical-pathological types of cutaneous melanomas and mortality rate in the region of Passo Fundo, RS, Brazil. Int J Dermatol. 2007;46(7):679-86.
31. Lebsa-Weber A, Nunes DH, Filho JJS, Pinto CJC. Assessment of 496 pathological reports of melanoma diagnosed in the city of Florianopolis, SC, Brazil An BrasDermatol. 2007;82(3):227-32.
32. Bakos L. Melanomas malignos e etnia. An Bras Dermatol. 1991;66:299-302.
33. Pinheiro ANC, Cabral ALSV, Friedman H, Rodriguez HA. Melanoma cutâneo: características clínicas, epidemiológicas e histopatológicas no Hospital Universitário de Brasília entre Janeiro de 1994 e Abril de 1999. An Bras Dermatol. 2013;78(2):179-86.
The present study was carried out at the Universidade Federal de Goiás - Goiânia (GO), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}