


Simone Ramos Nogueira Guerra Neri1; Flávia Alvim Sant'Anna Addor2; Meire Brasil Parada3; Sergio Schalka4
Keywords: HYALURONIC ACID; ACCIDENTS; DERMIS.
Hyaluronic acid (HA) based fillers have been the most frequently used filling substances in recent years for the treatment of wrinkles and folds, due to their practical application and good safety margins, in addition to their effects (which are immediately visible after application and have a long-term duration). The biocompatibility of HA and its relatively simple-tolearn technique has helped it become a frequent choice when addressing wrinkles and other alterations of the skin relief, especially on the face, but also in other areas such as the dorsum of the hands.1
More recently, HA has been used in facial volumization, for correcting the loss of fat pads due to aging, especially in the malar and mandibular areas. For these indications, the choice of HA has some particularities that differentiate it from its use for simple filling procedures. These include particle size, more viscoelasticity, different length of the polymer chain, and the type and density of the crosslinker, all of which play a part in obtaining the best result in the accommodation of the product into the skin, without the risk of migration from the injection site.
The application must be carried out in the supraperiosteal or deep subcutaneous planes; and cannulas-which reduce the risk of bleeding-can be used.2 Although all commercially available options for HA volumization present good tolerance, there is no filling substance available that is totally devoid of risk and even seasoned professionals can come across immediate reactions, such as erythema and bleeding, or others that manifest later, such as nodulations.3
The management of complications must be well known to the specialist physician, for while they may also result from poor technique, accidents in the application and anatomical variations may contribute to their onset.
A thirty-five year-old female patient underwent a filling procedure with HA (Juverderm Voluma®, Allergan) aimed at facial volumization through the retroinjection technique in the zygomatic arch region. An 18G, 70mm cannula was used without immediate complications (erythema or echymosis) and no particularities regarding the appearance. The patient was instructed to return within 15 days.
After that period, the patient returned with a pearly nodule 3cm in diameter, which extended from the zygomatic arch to the infraorbital region on the left-hand side, as well as with a deeper nodule1cm in diameteron the right-hand side infraorbital region. The patient reported mild pain on palpation of both nodules; nonetheless there were no phlogistic signs. The diagnostic hypothesis was that of the formation of nodules due to the accumulation of the filler itself, while the left-hand side, more medially, showed signs consistent with the Tyndall effect ("blue bump"). (Figure 1)
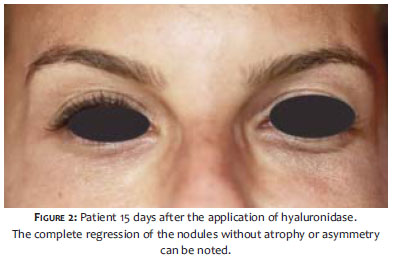
The patient was advised to use Prednisone 10mg every 12 hours for three days and apply warm and cold compresses alternately, for 15 days. As after that period there was no improvement seen at the reassessment visit, a decision was made for the application of lyophilized hyalurodinase (HYALOZIMA®/2,000UTR) diluted in 5ml, resulting in 400UTR/ml hyaluronidase doses; 0.3 ml and 0.1 ml were applied in the left and in the right-hand side of the patient's face, respectively. The injection was applied exactly within the nodules, pinching and isolating them with the thumb and forefinger. The patient was reevaluated after 15 days, with complete regression of the nodules and a satisfactory appearance, without signs of atrophy or asymmetry (Figure 2).
The formation of nodules after injection of HA fillers, due to its accumulation, is described as an early and relatively rare complication, among other observed adverse effects, for the total percentage of complications described with HA fillers is already low (less than 1%).4
Although nodules resulting from the accumulation of the product itself do not necessarily constitute a serious complication, they are nonetheless aesthetically undesirable, and treatment must be agile and careful in order to preserve the aesthetic outcome-especially in the presence of the Tyndall effect ("blue bump").
Nodules must be differentiated from granulomatous reactions, which are most often more delayed in onset. This might, however, be clinically difficult, particularly in cases of deep nodules, demanding nodule biopsy with pathological examination in order to differentiate the type of adverse reaction that has occurred.5,6
As volumization filling procedures are applied more deeply, in theory there would be reduced risk of superficial nodules, however in areas of very thin dermis-such as in the periorbital and upper malar regions-the risk of nodule formation may increase. The use of thinner cannulas, such as 21G or 22G, can also assist in the homogeneous aspect of the filler, or in the use of less dense fillers, with lower visco-elasticity or smaller particule size.7
Tyndalization is described in reference to the Tyndall effect, which occurs when the filler has been applied too superficially, and a bluish hue is observed in the overlying skin, observed through the thinner skin's transparency. That result is unaesthetic and can be seen even without palpation.
For correcting nodules and granulomas, local application of hyaluronidase is the treatment of choice; its use leads to faster and superior results than those obtained with the use of oral or injectable corticosteroids.
Hyaluronidase acts by reversibly depolymerizing existing HA around the cells of the connective tissue, thus temporarily reducing that tissue's viscosity and making it more permeable to the diffusion of liquids. Based on this mechanism of action, hyaluronidase started to be used in cases of complications and/or adverse reactions as a treatment option to promote the degradation of injected HA, with resulting improvement. In Brazil, there is availability of Hyalozima® 20,000UTR (Apsen), which after diluted in the solvent that accompanies the product, presents 4,000UTR / ml.8,9 Its use, however, should be administered very carefully in order to avoid excessive acid hydrolysis of HA, clinically entailing a depressed and atrophic appearance. Therefore, all dermatologists who perform filling procedures should master the application technique.10
The preparation should be carried out as follows: mix the entire contents of the diluent (5ml) with lyophilisate powder, in the vial. After the dissolution in complete, aspirate the contents and apply the minimum possible dose (0.1 to 0.2 ml per point), in the area where the HA is intended to be degraded. If necessary, repeat the application 10 to 15 days later. The remainder must be totally discarded and should not be stored and applied under any circumstances. This technique is similar to that of Brody, who suggests a five-minute interval between applicationsin order to observe any swelling, due to a rare but possible hypersensitivity to thedrug. In Dermatology, Crocco et al. corroborated this use in a recent article reviewing the complications of filling procedures.11
The necessity and usefulness of skin testing are questionable, due to its allergenic power.12
There are several brands of hyaluronidase available in the United States, however with different concentrations (Liporase,® Inno,® Hydase.®) In Brazil there is only one (Hyalozima®), and the use as described in the present study is considered off label.
The cautious use of hyaluronidase has consolidated itself in clinical practice as an effective drug in the management of nodules and granulomas arising from the application of HA, both in the case of superficial fillers and in the use of volumization substances.
The main focus of the authors in the present article is to highlight the fact that the use of hyaluronidase for degrading HA requires good technique and management by a dermatologist, as well as abiding by best practices and information, since there is no consensus on the use of this enzyme.
The type of complication described in the present article-which seems to happen more frequently in practice than the literature indicates-should be addressed promptly by the dermatologist, with a high probability of having favorable outcomes in most cases.
1. Bowman PH, Narins RS. Hialinos e Técnicas de Preenchimento. In: Carruthers J, Carruthers A. Técnicas de Preenchimento. New York: Elsevier; 2005. p. 35-56.
2. Requena L, Requena C, Christensen L, Zimmermann US, Kutzner H, Cerroni L.. Adverse reactions to injectable soft tissue fillers. J Am Acad Dermatol. 2011;64(1):5-7.
3. Junkins-Hopkins JM. Filler complications. J Am Acad Dermatol. 2010;63(4):703-5.
4. Carruthers J, Carruthers A. A prospective, randomized, parallel group study analyzing the effect of BTX-A and nonanimal sourced hyaluronic acid in combination compared with NASHA alone in severe glabellar rhytides in adult female subjects. Dermatol Surg.2003;29(8):802-9.
5. Dadzie O, Mahalingam M, Parada M, El Helou T, Philips T, Bhawan J.Adverse cutaneous reactions to soft tissue fillers - a review of the histological features. J Cutan Pathol. 2008;35(6):536-48.
6. Parada M, Michalany N, Hassun K, Bagatin E, Talarico S. A Histologic Study of Adverse Effects of Different Cosmetic Skin Fillers. New York: SkinMed; 2005. p. 345-49.
7. Braz AV, Sakuma TH. Preenchimentos e técnicas para o terço inferior da face. In: Kadunc B, Palermo E, Addor F, Metsavaht L, Rabello L, Mattos R, et al. Tratado de cirurgia dermatológica, cosmiatria e laser da Sociedade Brasileira de Dermatologia. Rio de Janeiro: Elsevier; 2012.
8. Soparkar CN, Patrinely JR, Tschen J.Erasing restylane. Ophthal Plast Reconstr Surg. 2004;20(4):317-8.
9. Sclafani AP, Fagien S.Treatment of injectable soft tissue filler complications. Dermatol Surg. 2009;35(Suppl 2):1672-80.
10. Hirsch RJ, Brody HJ, Carruthers JD Hyaluronidase in the office: a necessity for every dermasurgeon that injects hyaluronic acid. J Cosmet Laser Ther. 2007;9(3):182-5.
11. Harold J. Brody. Use of Hyaluronidase in the Treatment of Granulomatous Hyaluronic Acid Reactions or Unwanted Hyaluronic Acid Misplacement. Dermatol Surg. 2005;31(8):893-7.
12. Crocco EI, Alves RO, Alessi C. Eventos adversos do ácido hialurônico injetável. Surg Cosmet Dermatol 2012;4(3):259-63.
Study performed at Medcin Instituto da Pele-São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}