


Guilherme Augusto Gadens1, Paulo Rodrigo Pacola1, Arash Kimyai-Asadi1
Keywords: MOHS SURGERY, RECONSTRUCTION, EAR NEOPLASMS, EAR, SURGICAL FLAPS
The ear is a complex anatomical structure in which each subunit has unique characteristics. No single reconstruction technique could work in all situations; therefore, knowing different ways to reconstruct surgical defects in each one of these subunits is essential to achieving the best cosmetic results. We report here a detailed explanation of a superior helical advancement flap designated to repairs of the upper helical rim.
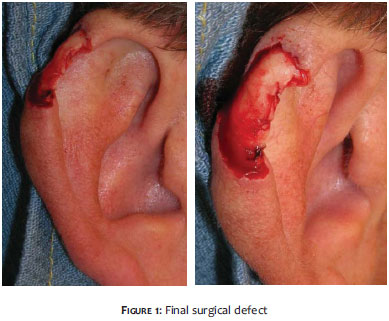
A 55-year-old Caucasian male (Fitzpatrick skin type II) presented with a 1. 0 cm x 0. 7 cm papule in his left superior auricular helix. The lesion had been previously biopsied by his attendant physician and the histological evaluation confirmed the diagnosis of basal cell carcinoma (BCC). After local anesthesia with 0. 5% lidocaine with 1:200,000 epinephrine, Mohs micrographic surgery was performed and the BCC was cleared in two stages. The final surgical defect size was 2. 0 cm x 1. 2 cm (Figure 1).
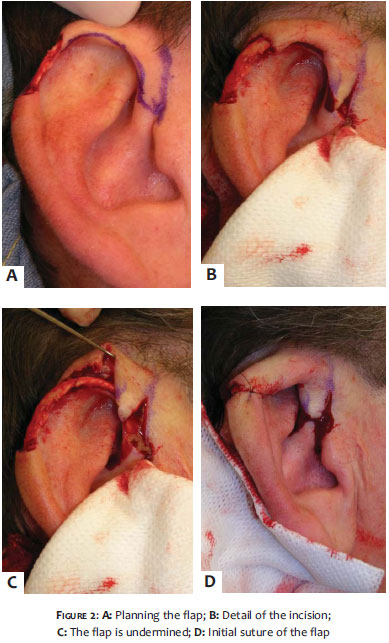
The superior advancement helix flap starts with an incision beginning from the anterior part of the defect and running until the superior border of the tragus. This incision parallels the inferior margin of the helix by approximately 1 mm and when it reaches its final length, a back cut is performed to allow the loose preauricular skin to advance freely (Figure 2A). Note that if the incision is made within the helical crease it will be much harder to suture later on. The whole flap is undermined until the postauricular sulcus and a Burow's triangle is taken from the posterior ear (Figures 2B and 2C). The initial suture of the flap places it into the right position (Figure 2D). After that, using 5. 0 nylon, the rest of the flap is sutured starting from the helix all the way down to the preauricular area (Figure 3).
The sutures were removed after seven days. No anatomic distortions were noted. The ear maintained its rounded, convex shape, its size, and no trapdooring occurred. Both the physicians and the patient were satisfied with the cosmetic outcome (Figure 4).
Repairing the superior helix usually requires flaps or grafts in order to maintain its rounded shape. Side-to-side sutures usually result in distortion of the local anatomy, with narrowing and notching of the helix. Second intention healing would have a very negative outcome because of the convexity of the area. Hence, many different techniques have been proposed to repair this region.
A wedge shaped resection of the lesion and primary suture would result in shortening of the ear, loss of the ear contour, and in unnecessary manipulation and loss of cartilage¹. Full thickness skin grafts also do not work well because of the convex shape and slender width of the area, making it difficult to properly place a pressure dressing needed to allow imbibition, and increasing the possibility of necrosis (which is already great since the graft might be placed over bare cartilage). A bilobed flap was recently described2 in the reconstruction of this area with good cosmetic results.
In our opinion though, the flap described here is much easier and less time consuming to perform, and achieves better cosmetic results since most of the incision is placed very close to the ear and in the same direction of a natural crease of the ear. Transposition flaps (from the preauricular region or postauricular sulcus) are also an option, but the risk of distal flap necrosis is greater, and it does not take advantage of the available spare skin of the proximal helix as the described flap does. The interpolation flap³ has the disadvantage of requiring two surgical stages-while the demands of most patients today are for only one-and the cosmetic results can be disappointing. There is also the traditional helical advancement flap4 (which can also be a condrocutaneous flap if necessary), which achieves excellent results when repairing the lateral helix but does not have the same outcome when dealing with defects located in the superior third of the helix. Moreover, there are numerous other techniques that can be used according to the preference of each physician.
The superior helical advancement flap described here has many similarities in its mechanism with the traditional helical advancement flap. The most important difference is that the superior flap uses the available preauricular skin, thus it advances from a region closer to the superior defect, whereas the traditional technique uses the available skin from the earlobe.
The superior helical advancement flap is an excellent technique when reconstructing surgical defects of 1. 0 cm to 2. 5 cm in the superior helix as long as the cartilage is preserved. It is simple to perform and its most important characteristic is that it provides outstanding cosmetic results.
1. Radonich MA, Zaher M, Bisaccia E, Scarborough D. Auricular reconstruction of helical rim defects: wedge resection revisited. Dermatol Surg. 2002;28(1):62-5.
2. Vergilis-Kalner IJ, Goldberg LH. Bilobed flap for reconstruction of defects of the helical rim and posterior ear. Dermatol Online J. 2010;16(10): 9.
3. Nguyen TH. Staged Cheek-to-Nose and Auricular Interpolation Flaps. Dermatol Surg. 2005; 31(8 pt 2):1034-45.
4. Krunic AL, Weitzul S, Taylor RS. Chondrocutaneous advancement flap for reconstruction of helical rim defects in dermatologic surgery. Aust J Dermatol. 2006;47(4):296-9.
5. Bastazini I Jr, Martins ALGP. Reconstrução de defeito condrocutâneo auricular usando fibra de silicone. Surg Cosmet Dermatol. 2011;3(2):163-5.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}