


Leticia Midori Kondo Iwamoto1; Flavia Rodrigues Dias2; Otavio Augusto Noschang Moreira3; Helio Amante Miot3; Ana Claudia Athanasio Shwetz1,3
Funding: None
Conflict of interest: None
Submitted on: 10/28/2025
Final decision: 12/26/2025
How to cite this article: Iwamoto LMK, Dias FR, Moreira OAN, Miot HA, Shwetz ACA. Cemiplimab therapy for Marjolin ulcer arising in folliculitis decalvans: a case report. Surg Cosmet Dermatol. 2026;18(1):e20260531.
Malignant transformation of folliculitis decalvans (FD) into squamous cell carcinoma (SCC) is rare but relevant due to its aggressive clinical course. We report the case of a 53-year-old man, a Jehovah's Witness, with a long-standing history of FD who developed rapidly progressive metastatic scalp SCC. Due to refusal of surgery, cemiplimab monotherapy (a PD-1 inhibitor) was initiated, resulting in complete resolution of the neoplasm within 12 weeks. This case highlights the risk of malignant transformation in chronic inflammatory dermatoses and suggests cemiplimab as an effective treatment option for advanced SCC when surgical resection is not feasible.
Keywords: Carcinoma, Squamous Cell; Skin Ulcer; Alopecia; Immune Checkpoint Inhibitors; Cicatrix; Skin Neoplasms
Folliculitis decalvans (FD) is a rare neutrophilic cicatricial alopecia characterized by perifollicular inflammation, pustules, and progressive fibrosis, often difficult to manage and resulting in scarring.1 Marjolin ulcer (MU) is a rare cutaneous malignancy arising in chronic wounds and scars, most commonly represented histologically by squamous cell carcinoma (SCC).2 SCC is most frequently associated with deep burn wounds, and its occurrence in the context of FD is exceedingly uncommon.1,2 The treatment of MU generally involves wide excision combined with adjuvant therapies.3 We report a case of advanced SCC arising in chronic FD successfully treated with cemiplimab monotherapy, highlighting its clinical implications.
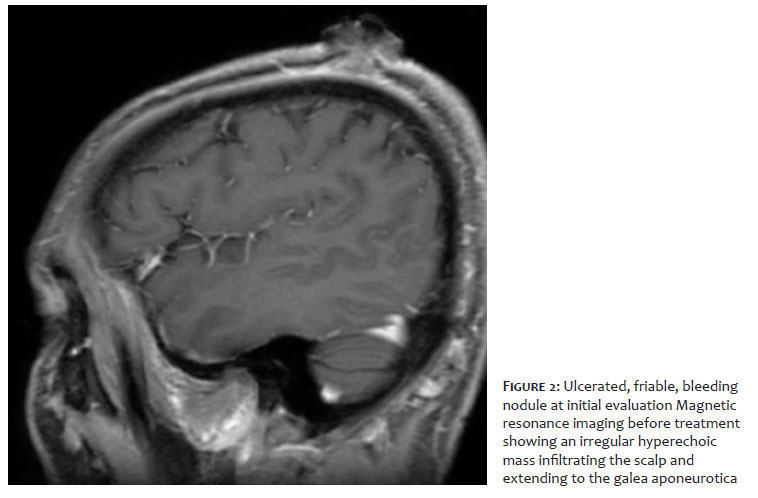
A 53-year-old man, a Jehovah's Witness, undergoing treatment for FD with doxycycline for 4 years, presented with a friable, bleeding nodular lesion on the scalp, with rapid growth over 2 months (Figure 1). Physical examination revealed palpable cervical and supraclavicular lymphadenopathy. Histopathological analysis confirmed invasive, ulcerated, well-differentiated SCC. Magnetic resonance imaging demonstrated an infiltrative lesion involving the dermis, subcutaneous tissue, and galea aponeurotica, in close proximity to the skull (Figure 2). Positron emission tomography (PET) identified cervical and supraclavicular lymphadenopathy, consistent with non-regional metastases. The tumor was classified as stage IV SCC (T4N1/N2M0) according to the 8th edition of the American Joint Committee on Cancer (AJCC) staging system.
Due to the patient's refusal of surgical intervention for religious reasons and the presence of lymph node and bone metastases, treatment with cemiplimab (350 mg intravenously every 3 weeks) was initiated. After 12 weeks, complete clinical and radiologic resolution was observed (Figures 3 and 4), with PET demonstrating no hypermetabolic activity in the scalp lesion and stable lymph nodes.
First described in 1828 by Jean Nicolas Marjolin, MU is an aggressive neoplasm classically arising in burn scars.4 Other conditions, including hidradenitis suppurativa, pressure ulcers, venous ulcers, and HPV infections, have also been identified as risk factors.1,2 Chronic inflammation increases the risk of cutaneous carcinogenesis, because continuous production of pro-inflammatory cytokines and tissue remodeling create a microenvironment conducive to malignant transformation.2 Furthermore, areas of chronic scarring can lose immune system cells, hindering immune surveillance and favoring tumor aggressiveness and metastatic potential.2 However, reports of MU arising in the setting of cicatricial alopecias remain scarce.1
Suspicion for MU should be raised in the presence of a non-healing, indurated lesion with rapid growth, foul odor, and elevated, infiltrated borders, typically arising in areas of chronic wounds or scars.2 Additional signs include exophytic granulation tissue, local bleeding, and regional lymphadenopathy.2
Treatment of MU generally involves wide excision with lymph node dissection, and adjuvant radiotherapy or chemotherapy may be considered.3 Cemiplimab, a high-affinity PD-1 inhibitor, is an immunotherapy agent approved by the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA) for patients with metastatic or locally advanced SCC who are not candidates for curative surgery or radiotherapy.5 Clinical trials have demonstrated rapid and substantial antitumor response, with an acceptable safety profile.5
In the present case, cemiplimab proved to be an effective and well-tolerated option, resulting in complete response.
In this case of stage IV SCC in a patient who declined invasive therapies due to religious beliefs, cemiplimab was selected as an alternative treatment and achieved complete response. This report underscores the importance of close clinical monitoring and early biopsy of suspicious lesions in patients with chronic inflammatory scalp diseases, given the risk of malignant transformation. Cemiplimab demonstrated efficacy in this case of advanced SCC, reinforcing the role of immunotherapy in metastatic or unresectable cutaneous malignancies when surgical intervention is not feasible.
Leticia Midori Kondo Iwamoto
ORCID: 0009-0001-5080-4619
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Flavia Rodrigues Dias
ORCID: 0009-0008-0821-3656
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Critical review of the literature, Critical revision of the manuscript.
Otavio Augusto Noschang Moreira
Approval of the final version of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature.
Helio Amante Miot
ORCID: 0000-0002-2596-9294
Author's contribution: Effective participation in the conduct of the study, Critical review of the literature.
Ana Claudia Athanasio Shwetz
ORCID: 0000-0002-9373-5019
Approval of the final version of the manuscript, Conception and design of the study, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
1. McMullen E, Maazi M, Te B, Donovan J. Folliculitis decalvans as a potential risk factor for cutaneous malignancy. Int J Dermatol. 2024;63(9):e223-4.
2. Bazaliński D, Przybek-Mita J, Barańska B, Więch P. Marjolin's ulcer in chronic wounds - review of available literature. Contemp Oncol (Pozn). 2017;21(3):197-202.
3. Aydogdu E, Yildirim S, Aköz T. Is surgery an effective and adequate treatment in advanced Marjolin's ulcer? Burns. 2005;31(4):421-31.
4. Cruickshank AH, McConnell EM, Miller DG. Malignancy in scars, chronic ulcers, and sinuses. J Clin Pathol. 1963;16(6):573-80.
5. Migden MR, Rischin D, Schmults CD, Guminski A, Hauschild A, Lewis KD, et al. PD-1 blockade with cemiplimab in advanced cutaneous squamous-cell carcinoma. N Engl J Med. 2018;379(4):341-51.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}