


Indira Saraswati Sanjaya1; Kelvin Kohar1; Chastine Harlim1; Lili Legiawati2; Nandita Melati Putri3
Funding: The authors received no financial support for the research, authorship, and/or publication of this article.
Submitted on: 09/01/2025
Final decision: 12/17/2025
How to cite this article: Sanjaya IS, Kohar K, Harlim C, Legiawati L, Putri MN. Safety and efficacy of intense pulsed light therapy combined with fractional laser therapy for scar management: a systematic review. Surg Cosmet Dermatol. 2026;18(1):e20260513.
BACKGROUND: Wound healing is a complex process, and various factors can disrupt this process, leading to non-healing wounds or scarring. Conventional treatments for scar management often have low efficacy and high recurrence rates. The combination of intense pulsed light (IPL) and fractional laser therapy (FLT) has emerged as a minimally invasive alternative with promising results. The goal of this study was to evaluate the safety and efficacy of combined IPL + FLT therapy and to manage pathological scars.
METHODS: This study followed PRISMA guidelines. Systematic searches were performed in PubMed, ProQuest, Scopus, and the Cochrane Library up to December 2025. Studies involving patients with pathological scars treated using combination IPL and FLT were included.
RESULTS: Five studies met the eligibility criteria, comprising 3 randomized controlled trials, 1 retrospective cohort study, and 1 case series, totaling 288 patients. Across all studies, combination therapy produced significant reductions in POSAS, MSS, and VSS scores in hypertrophic and postoperative scars. One study reported significantly higher patient satisfaction rates (p<0.05). Adverse effects were minimal, primarily mild transient erythema.
CONCLUSION: Combined FLT and IPL safely enhance scar appearance, with low adverse effect rates, offering an effective and minimally invasive therapeutic option.
Keywords: Keloid; Cicatrix, Hypertrophic; Laser Therapy; Intense Pulsed Light Therapy
Pathological scars, particularly hypertrophic scars and keloids, result from abnormal wound healing and are characterized by excessive collagen deposition and persistent fibroblast activity. These scars may cause pain, pruritus, contractures, and cosmetic disfigurement, leading to functional impairment and a serious psychosocial burden for affected patients. Because their pathogenesis is multifactorial and chronic, achieving durable and satisfactory scar improvement remains clinically challenging.1–3
Conventional non-laser treatments, including surgical excision, pressure garments, silicone sheeting, intralesional corticosteroids or other pharmacologic agents, cryotherapy, and radiotherapy, have shown variable and often limited efficacy.3,4 Recurrence rates, especially after excision of keloids and hypertrophic scars, remain high, and many modalities are associated with discomfort, prolonged downtime, or adverse effects that may further compromise cosmetic outcomes. These limitations have driven the search for alternative, minimally invasive approaches that can target multiple components of scar pathology simultaneously.5,6
Laser and light-based therapies have emerged as important options for scar management. Fractional laser therapy (FLT) delivers energy in a pixelated pattern to generate microthermal zones within the dermis, promoting collagen remodeling, softening scar texture, and improving thickness, pliability, and pigmentation.7,8 Intense pulsed light (IPL), a noncoherent, polychromatic light source, acts through selective photothermolysis of hemoglobin and melanin to reduce erythema and dyschromia while exerting modest effects on dermal remodeling.9 Given the complementary mechanisms of the two modalities (vascular and pigment targeting by IPL and deep structural remodeling by FLT), their combination has been proposed as a rational strategy to address the multifaceted nature of pathological scars. Early clinical studies suggest that IPL-FLT combinations can enhance overall scar improvement and patient satisfaction without substantially increasing adverse events.10,11
With growing interest in scar management and more studies on the use of combined IPL-FLT, synthesizing high-quality evidence is warranted. Accordingly, we conducted a systematic review on the safety and efficacy of IPL-FLT combination therapy for scar management. The goal was to provide clinicians with insight into an alternative therapeutic modality for managing scars.
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines. The protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO), registration number CRD420251012803.
A systematic search of 4 large scientific and medical databases, PubMed, ProQuest, Scopus, and Cochrane, was performed to identify all relevant studies published up to December 2025. In addition, reference lists from all eligible articles were screened for additional studies. The inclusion criteria were studies in which patients had pathological scars (keloids or hypertrophic scars) and treated with a combination of FLT and IPL. Primary outcomes were assessed using standardized scar evaluation tools, such as the Patient and Observer Scar Assessment Scale (POSAS), Manchester Scar Scale (MSS), Vancouver Scar Scale (VSS), and other validated scar assessment tools. Incomplete studies, studies lacking an available full-text versions, studies in languages other than English, and those published more than 15 years prior to the search period were excluded.
Data extraction was conducted in accordance with the Cochrane Handbook for Systematic Reviews of Interventions. Three independent reviewers screened and extracted data using Google Sheets and Microsoft Excel for systematic organization and analysis. Discrepancies arising from the extraction process were resolved through discussion and consensus. The extracted data included study (authors, year of publication, level of evidence, country, study duration, study design, and follow-up period) and patient characteristics (sample size, sex distribution, age range, Fitzpatrick skin type, pathological scar type, anatomical site, and etiology). Intervention details were also documented, including type of fractional laser, type of IPL parameters, number of treatment sessions, energy settings, pulse duration, and any adjunctive treatment protocols. Outcomes were measured using standardized scar scoring tools such as POSAS, MSS, and VSS. Complications and both physician- and patient-reported adverse events were also noted. The level of evidence for each study was assessed according to Oxford Centre for Evidence-Based Medicine criteria.
Studies were systematically assessed using tools appropriate to each study design. Three independent reviewers assessed study quality using the Cochrane Risk of Bias 2 (RoB 2) tool for randomized controlled trials (RCTs) and the Joanna Briggs Institute (JBI) checklist for case series and cohort studies. Disagreements were resolved through discussion to achieve consensus.
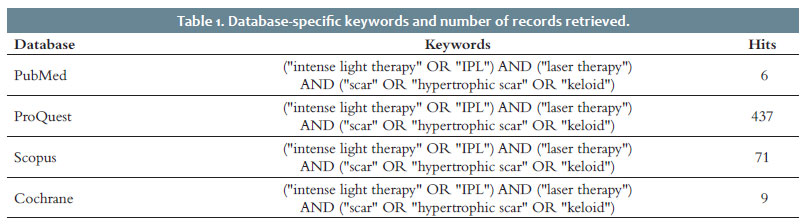
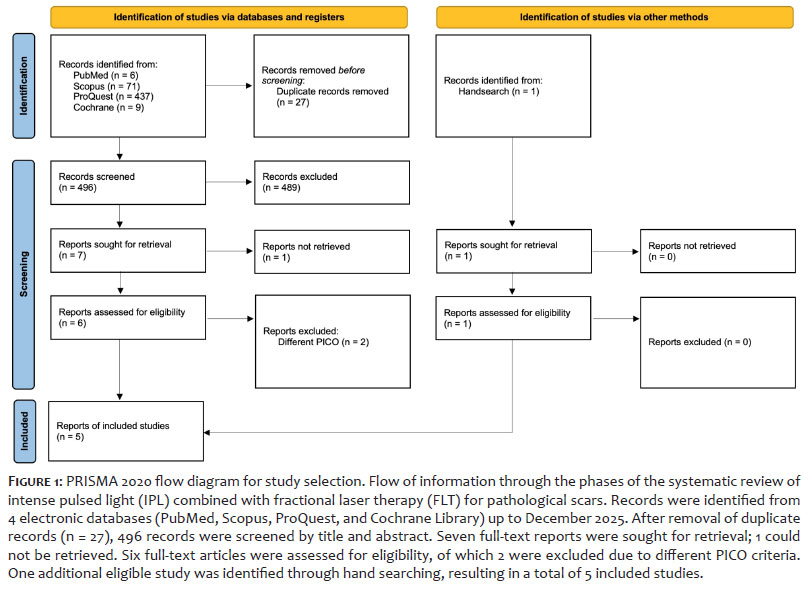
The literature search was limited to English-language publications and over a 15-year period. Database-specific keywords, along with the corresponding search results, are presented in Table 1. The study selection process is depicted in Figure 1.
The initial search yielded 523 records. After removal of duplicates, 496 studies underwent title and abstract screening. Six were assessed for full-text eligibility. Two studies were excluded due to a lack of relevant outcome and population data, leaving 4 studies from the database search for inclusion. One additional eligible retrospective comparative study was identified through manual searching, resulting in a total of 5 studies. The studies included in this review consisted of 3 RCTs, 1 retrospective cohort study, and 1 case series. Due to heterogeneity in study design and outcome measures, no meta-analysis was performed; instead, a qualitative synthesis was conducted.
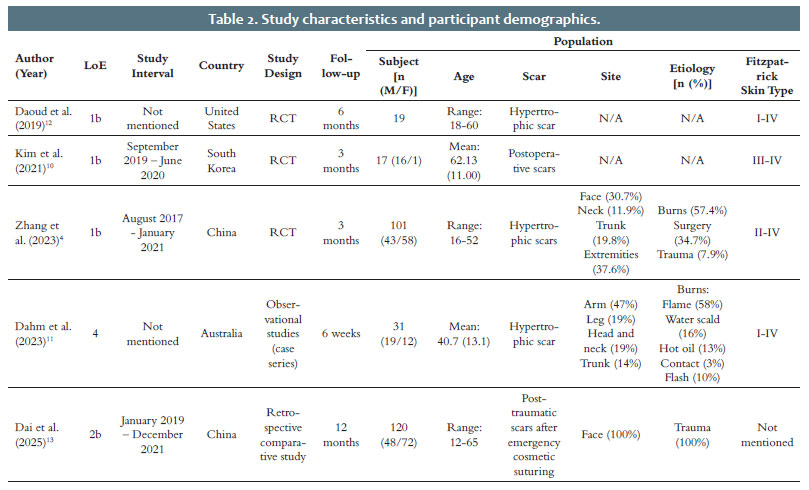
A total of 288 patients were included across the studies, which were conducted in the United States, China, South Korea, and Australia. Participant ages ranged from 16 to 65 years, and follow-up intervals ranged from 6 weeks to 12 months. The studies primarily included pathological scars (hypertrophic and postoperative scars). One study evaluated early post-traumatic facial wounds following cosmetic suturing, focusing on preventing hypertrophic scarring. Fitzpatrick skin types I–IV were most prevalent, with few studies involving individuals with darker skin type (III–IV). Scar locations varied, including the face, neck, trunk, extremities, and limbs. Etiologies included burns (flame, scald, hot oil, contact, flash burns), surgery, and trauma. An in-depth description of participant characteristics can be found in Table 2.
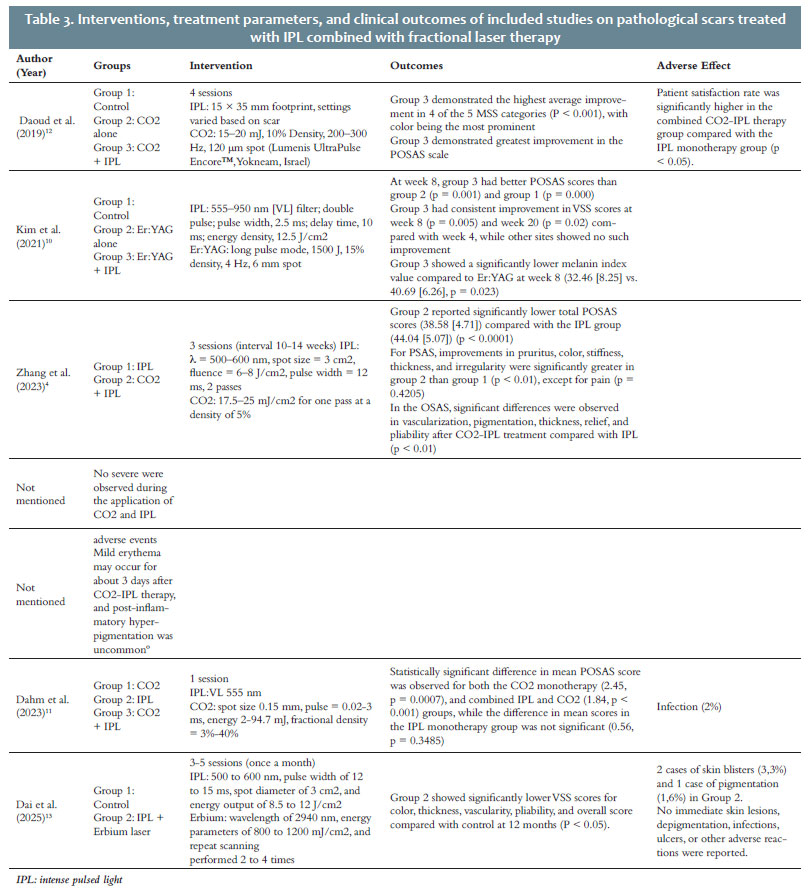
Scar outcomes were assessed using standardized instruments such as POSAS, MSS, and VSS. Across all studies, combination therapy with IPL and FLT consistently outperformed monotherapy. In a study by Dahm et al.,11 a single treatment pass of combined IPL and CO2 laser significantly improved POSAS scores, with a mean reduction of 1.93 for the overall score (p < 0.0001), and significant improvements in color (–1.97), thickness (–2.10), and stiffness (–2.47), among others. Daoud et al.12 found a statistically significant (p < 0.001) greater improvement in scar color (–2.21) and texture (–1.97) in the combination group compared with CO2 laser alone.
Kim et al.10 reported that early intervention with IPL and Er:YAG laser significantly lowered POSAS scores at week 8 (p = 0.001) and week 20 (p = 0.012) compared with Er:YAG monotherapy. In a retrospective cohort study by Dai et al.,13 early preventive treatment with IPL combined with fractional erbium laser resulted in significantly lower VSS scores for color, thickness, vascularity, pliability, and overall score at 12 months compared with conventional therapy (p < 0.05). Finally, Zhang et al.4 reported significantly better outcomes in color, pruritus, thickness, and irregularity in the CO2+IPL group (p < 0.01), and 100% patient satisfaction versus 84% in the IPL-only group. Table 3 presents additional information on interventions and outcomes.
Adverse events were generally mild and self-limited. The most common adverse events were transient erythema, edema, and discomfort, resolving within days. Dahm et al.11 reported 2 minor infections requiring oral antibiotics, while Daoud et al.12 observed no adverse events. Kim et al.10 reported no complications, and Zhang et al.4 found no significant difference in adverse event rates between combination and monotherapy groups. Dai et al.13 reported 3 complications in the combination group, 2 cases of transient blistering and 1 case of temporary pigmentation, all of which resolved without long-term sequelae. Overall, combination therapy was well tolerated and demonstrated a favorable safety profile.
Study quality was assessed using design-appropriate critical appraisal tools. Three RCTs were evaluated using the Cochrane RoB-2 tool. All RCTs (Daoud et al.,12 Kim et al.,10 and Zhang et al.4) demonstrated low risk of bias across most domains, particularly in randomization, intervention delivery, and outcome measurement. - However, each study raised concerns regarding selective reporting due to unclear pre-specified analysis plans or lack of trial registration, which may introduce reporting bias (Table 4). Nevertheless, outcome assessments were largely blinded and used validated scar assessment scales, supporting the reliability of their findings.
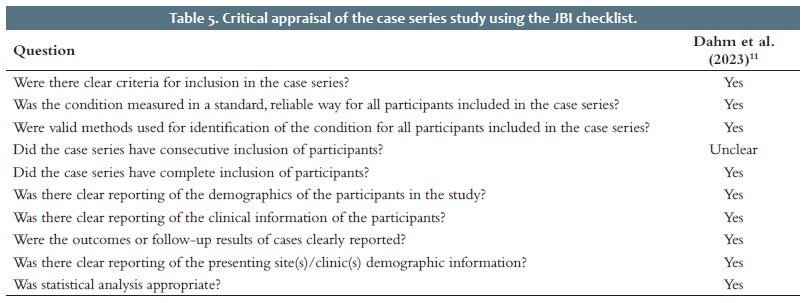
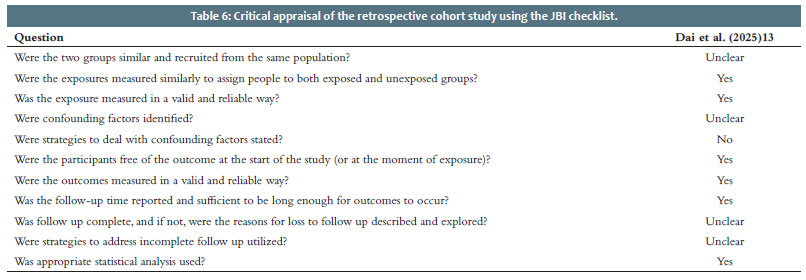
The case series by Dahm et al.11 was assessed using the JBI checklist and met most criteria, including clear inclusion criteria, standardized outcome measures, valid condition identification, and appropriate statistical analysis. - However, it remained unclear whether participants were included consecutively, which may introduce selection bias (Table 5). The retrospective cohort study by Dai et al.13 was assessed using the JBI Critical Appraisal Checklist for Cohort Studies. The study was judged to have moderate risk of bias, primarily due to non-random allocation, limited reporting of potential confounders, and absence of multivariable adjustment. However, outcome assessment used standardized scar scores with an adequate 12-month follow-up period (Table 6). Overall, the studies included were of moderate to high quality, supporting the validity of the synthesized findings.
Wound healing is a dynamic biological process that progresses through overlapping phases: inflammation, proliferation, and remodeling. Effective healing involves tightly regulated pro- and anti-inflammatory signaling, fibroblast proliferation, and extracellular matrix (ECM) remodeling. Dysregulation at any stage, most critically in the remodeling phase, can lead to pathological scarring, characterized by abnormal collagen deposition and persistent fibroblast activity.14,15
Hypertrophic scars and keloids are pathological scars characterized by fibrotic tissue overgrowth, although they vary in extent and histological features. Hypertrophic scars remain confined to the primary lesion site and may regress spontaneously, while keloids, which extend beyond wound boundaries, are permanent and symptomatic. Globally, over 100 million new scars are estimated to form annually, with approximately 11 million progressing to keloids. Their etiology is multifactorial, including chronic inflammation, dysregulated transforming growth factor-β (TGF-β) signaling, mechanical tension, hypoxia, and genetic predisposition.14–16
Current management strategies include surgical excision, intralesional corticosteroid injection, silicone therapy, pressure garments, cryotherapy, and laser therapy. However, traditional treatments often yield incomplete responses and have high recurrence rates, particularly in keloids, which have post-excision recurrence rates of up to 70%. These limitations have spurred exploration of combination therapies that target multiple pathways involved in scar formation.14,17,18 One promising breakthrough is the use of IPL in combination with FLT. IPL targets vascular and pigmentary components through selective photothermolysis, while FLT induces dermal remodeling and stimulates neocollagenesis via microthermal injury. Their synergistic mechanism aligns with the multifactorial nature of pathological scar formation, offering a more comprehensive, minimally invasive, and well-tolerated therapeutic approach.4,9,19
IPL is a nonlaser technology that generates high-intensity, polychromatic light across a broad wavelength (typically 500–1200 nm). Its mechanism of operation is based on selective photothermolysis, whereby targeted chromophores in the body, primarily hemoglobin and melanin, absorb specific wavelengths, generating controlled thermal damage. For scars, IPL selectively targets hemoglobin to induce coagulation in the neovasculature, reducing vascularity and erythema in hypertrophic scars. Additionally, thermal effects can limit oxygen availability to hyperproliferative fibroblasts, indirectly reducing collagen synthesis and promoting remodeling.9,12
In addition to vascular effects, IPL influences dyschromia by targeting melanin, thereby reducing the hyperpigmentation often found in hypertrophic scars. IPL also weakly induces dermal remodeling by causing low-level thermal damage, promoting matrix metalloproteinase (MMP) expression while inhibiting TGF-β1, a key profibrotic cytokine. Clinically, IPL has been shown to reduce scar thickness, erythema, and stiffness with low downtime and a good safety profile.4,9,12
FLT, particularly ablative fractional CO2 lasers, delivers energy in a pixelated pattern, creating microthermal zones (MTZs) that penetrate the epidermis and the dermis. The controlled injury to the dermis stimulates an exaggerated healing process in the wound that includes upregulation of MMPs (eg, MMP-1 and MMP-9), dissolution of disorganized collagens, and deposition of new, organized collagens.20,21
The fractional approach offers rapid re-epithelialization while preserving surrounding untreated tissue, attaining an improved safety-efficacy balance. Histologically, FLT reduces dermal fibrosis; normalizes the distorted architecture of the hypertrophic scar, flattening it; and improves pliability, vascularity, and pigmentation through ECM remodeling and regularization of fibroblast phenotype. FLT may also control inflammatory cytokines and suppress TGF-β1 signaling, limiting collagen overproduction in scar pathogenesis. Clinically, multiple studies and meta-analyses confirm major improvements in VSS and POSAS scores following FLT, especially in thickness, pliability, and pigmentation.19–21
IPL and FLT are effective as monotherapies, but their combination offers synergistic benefits by addressing different pathophysiological aspects of scar formation. IPL primarily targets vascularity and pigmentation, contributing to early modulation of the inflammatory response and reduction of erythema and hyperpigmentation. Meanwhile, FLT helps deep dermal remodeling, targeting scar thickness, collagen disorganization, and textural irregularities.4,10,12,19
The complementary use of IPL and FLT has demonstrated enhanced efficacy in scar management by targeting multiple pathological features. In the study by Dahm et al., combined CO2 and IPL therapy significantly improved scar parameters, including pain, pruritus, color, stiffness, and thickness, with notable improvements across all POSAS domains after a single session. Importantly, the treatment was well-tolerated, with no major adverse effects reported and only minor, self-limited infections in 2 cases.11 Similarly, Daoud et al. found that combination IPL and fractional CO2 laser resulted in superior improvement in scar texture and color compared with CO2 laser alone, and no adverse events were reported during the study, supporting the safety of the combined modality.12 In a split wound trial by Kim et al., early combined IPL and Er:YAG laser treatment provided significantly better scar prevention than Er:YAG alone or control, and was well-tolerated throughout follow-up, with no serious adverse events observed.10 Zhang et al. reported that the combination of CO2 fractional laser and narrowband IPL significantly improved pruritus, color, stiffness, and irregularity compared with IPL alone, with 100% patient satisfaction in the combination group and no reports of severe complications, indicating a favorable safety profile.4 Consistent with these interventional trials, Dai et al. demonstrated that early preventive treatment with IPL combined with fractional erbium laser resulted in significantly lower VSS scores for color, thickness, vascularity, pliability, and overall score at 12 months compared with conventional anti-scar therapy alone, suggesting that the benefits of combination therapy extend beyond established scars to the prevention of hypertrophic scar formation.13 Collectively, these findings suggest that combining IPL and fractional lasers offers synergistic benefits in scar improvement while but also maintaining a minimal and acceptable safety profile, making it a safe and comprehensive therapeutic strategy for pathological scar management. This multimodal approach is in line with current concepts of algorithmic scar therapy, in which vascular-targeting treatments such as IPL are initiated early, followed by structural remodeling with FLT. Such integrative strategies allow for individualized, comprehensive treatment plans with superior cosmetic and functional outcomes.
This systematic review has several strengths. First, it was conducted in accordance with PRISMA guidelines and preregistered in the PROSPERO database, supporting methodological rigor and transparent reporting. The studies included spanned multiple countries as well as diverse pathological scar types, such as postoperative and hypertrophic scars, enhancing the generalizability of the findings. Many studies employed established outcome instruments such as POSAS, MSS, and VSS, allowing treatment efficacy to be assessed in a consistent and objective manner. Combination therapy with IPL and FLT demonstrated statistically significant decreases in scar prominence in all studies in terms of color, thickness, and stiffness, while maintaining a positive safety profile. Low-level, self-limited adverse events such as transient erythema and mild stinging were recorded, as were high levels of patient satisfaction. In addition, the inclusion of an early preventive cohort to assess combination IPL and fractional laser in a post-traumatic setting suggests that the benefits of this approach may extend beyond the management of established pathological scars to the prevention of hypertrophic scar formation, thereby broadening its potential clinical application across the scar continuum.
Despite these strengths, several limitations should be noted. Only 5 studies were included, involving a total of 288 patients, most with small sample sizes and short follow-up periods (≤6 months in most studies, with only one providing 12-month data), limiting the assessment of long-term outcomes. There was also heterogeneity in treatment parameters, including energy levels, number of sessions, and device types, which limit reproducibility and comparability. Three RCTs were included, but none had preregistered protocols or fully implemented blinding, which may be a source of bias. Moreover, direct head-to-head comparisons between combination IPL-FLT and standard non-laser therapies such as intralesional corticosteroids, pressure garments, and silicone sheeting, are lacking. Finally, none of the studies included in this review systematically evaluated cost-effectiveness, resource utilization, or workflow integration, which are critical for the widespread adoption of combined IPL-FLT therapy. Future studies should incorporate economic evaluations, include patients with a broader range of skin phototypes, and use standardized treatment protocols and outcome measures to strengthen the evidence base.
The combination of IPL and FLT is a promising approach in scar management. By targeting both vascular and structural components, this dual-modality therapy provides benefits in scar texture, color, thickness, and patient satisfaction. The evidence suggests combination therapy has a favorable safety profile with minimal adverse events. Based on these findings, IPL combined with FLT may represent a safe, effective, and minimally invasive therapy for managing of pathological scars. Additional large-scale, long-term studies are required to standardize treatment protocols and confirm clinical efficacy.
Indira Saraswati Sanjaya
ORCID: 0009-0000-6616-1657
Statistical analysis, Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Critical review of the literature, Critical revision of the manuscript
Kelvin Kohar
ORCID: 0000-0002-4789-0747
Statistical analysis, Approval of the final version of the manuscript, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Critical revision of the manuscript
Chastine Harlim
ORCID: 0009-0007-1979-249X
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Critical revision of the manuscript.
Lili Legiawati
ORCID: 0000-0002-5793-2525
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Effective participation in the conduct of the study, Critical revision of the manuscript.
Nandita Melati Putri
ORCID: 0000-0003-0839-7877
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Effective participation in the conduct of the study, Critical revision of the manuscript.
1. Wang ZC, Zhao WY, Cao Y, Liu YQ, Sun Q, Shi P, et al. The roles of inflammation in keloid and hypertrophic scars. Front Immunol. 2020;11:603187.
2. Lubczyńska A, Garncarczyk A, Wcisło-Dziadecka D. Effectiveness of various methods of manual scar therapy. Skin Res Technol. 2023;29(3):e13272.
3. Atiyeh B, Ibrahim A. Nonsurgical management of hypertrophic scars: evidence-based therapies, standard practices, and emerging methods: an update. Aesthetic Plast Surg. 2020;44(4):1345–7.
4. Zhang Y, Ye R, Dong J, Bai Y, He Y, Ni W, et al. Efficacy and safety of ablative CO2 fractional laser and narrowband intense pulsed light for the treatment of hypertrophic scars: a prospective, randomized controlled trial. J Dermatol Treat. 2023;34(1).
5. Tian Q, Zhang YX, Wang JJ, Huang GB. Advances in photoelectric therapy for the early intervention and treatment of traumatic scars. Clin Cosmet Investig Dermatol. 2023;16:869–77.
6. Barone N, Safran T, Vorstenbosch J, Davison PG, Cugno S, Murphy AM. Current advances in hypertrophic scar and keloid management. Semin Plast Surg. 2021;35(3):145–52.
7. Almeghawesh Y. The efficacy of low energy fractional carbon dioxide laser therapy in management of post-surgical hypertrophic scars. Int J Health Sci (Qassim). 2023;7(S1):2794–802.
8. Simbolon Sitohang IB, Sirait SAP, Safira FD. Fractional carbon dioxide laser for treating hypertrophic scars: a systematic review of randomised trials. Australas J Dermatol. 2022;63(1):27–35.
9. Thanh LT, Quan TS, Anh LV, Hung TQ, Vuong NL. The efficacy of intense pulsed light in the treatment of keloids and hypertrophic scars. J Lasers Med Sci. 2023;14.
10. Kim JC, Kang SY, Kim HO, Park CW, Kwon O, Chung BY. Efficacy of combined treatment with intense pulsed light and fractional erbium:YAG Laser in scar prevention: A randomized split wound trial. Dermatol Ther. 2021;34(5).
11. Dahm S, Lee G, Cleland H, Menezes H, Ng S. The use of carbon dioxide and intense pulsed light laser for the treatment of hypertrophic burn scars: A case series. Scars Burn Heal. 2023 Jan;9:20595131231202104.
12. Daoud AA, Gianatasio C, Rudnick A, Michael M, Waibel JS. Efficacy of combined intense pulsed light (ipl) with fractional co2-laser ablation in the treatment of large hypertrophic scars: a prospective, randomized control trial. Lasers Surg Med. 2019;51(8):678–85.
13. Dai Q, Cheng L, Wang C. The effectiveness of early treatment with intense pulsed light combined with fractional erbium laser in preventing post-traumatic hypertrophic scar formation. J Craniofac Surg. 2025;36(3):e342–5.
14. Riedemann HI, Schmidt MF, Baron JM. Therapy of pathological scars. JDDG - J German Soc Dermatol. 2023;21(7):761–76.
15. Ma Y, Liu Z, Miao LL, Jiang X, Ruan H, Xuan R, et al. Mechanisms underlying pathological scarring by fibroblasts during wound healing. Int Wound J. 2023;20(6):2190.
16. Li S, Ding H, Yang Y, Yu B, Chen M. Global research status of pathological scar reported over the period 2001–2021: A 20-year bibliometric analysis. Int Wound J. 2023;20(5):1725–38.
17. Bronte J, Zhou C, Vempati A, Tam C, Khong J, Hazany S, et al. A comprehensive review of non-surgical treatments for hypertrophic and keloid scars in skin of color. Clin Cosmet Investig Dermatol. 2024;17:1459.
18. Ogawa R. Keloid and hypertrophic scars are the result of chronic inflammation in the reticular dermis. Int J Mol Sci. 2017;18(3).
19. Wang J, Yu Q, Zhou Q, Tao M, Cao Y, Yang X. Application of fractional carbon dioxide laser monotherapy in keloids: a meta-analysis. J Cosmet Dermatol. 2024;23(4):1178–86.
20. Peng W, Zhang X, Kong X, Shi K. The efficacy and safety of fractional CO2 laser therapy in the treatment of burn scars: a meta-analysis. Burns. 2021;47(7):1469–77.
21. Almeghawesh Y. The efficacy of low energy fractional carbon dioxide laser therapy in management of post-surgical hypertrophic scars. Int J Health Sci (Qassim). 2023;7(S1):2794–802.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}