


Gabriela Roncada Haddad1; Ana Carolina Salomão Gerolamo2; Nicole Dias Sbrissa2; José Ferreira de Oliveira Neto3; Isabela Novello 3; Ricardo Henrique Marcelino3
Funding: None
Conflict of interest: None
Submitted on: 06/23/2025
Final decision: 10/15/2025
How to cite this article: Haddad GR, Gerolamo ACS, Sbrissa ND, Oliveira Neto JF, Marcelino RH, Novello I. Phenol peels: indications, complications and patient management, a literature review. Surg Cosmet Dermatol. 2025;17:e20250486.
Phenol peels are a deep chemical exfoliation technique used for decades for facial rejuvenation, acne scars, and hyperpigmentation. The Baker-Gordon formula is the most commonly used, providing effective results but with significant risks. The procedure requires anesthesia and strict postoperative care due to possible complications such as hyperpigmentation, hypopigmentation, infections, scarring, and systemic toxicity, especially cardiotoxicity. This descriptive and exploratory literature review, based on articles from 2000 to 2025, highlights the method’s effectiveness but emphasizes the need for further studies on its long-term safety and on proper patient management.
Keywords: Phenol; Chemexfoliation; Drug-Related Side Effects and Adverse Reactions
Chemical peels consist of the application of a chemical agent to the skin, which causes controlled destruction of the epidermis and part of the dermis by chemical exfoliation, followed by the promotion of cellular regeneration, ie, re-epithelialization.1,2
Peels are categorized according to depth as superficial, medium, or deep. The deeper the procedure, the more apparent its effects, but also the greater the risks and the discomfort. Superficial peels act only on the epidermis, medium peels act on the epidermis and papillary dermis, and deep peels penetrate to the reticular dermis. Phenol peels are an example of deep peels.3
Phenol, or carbolic acid (C6H5OH) (Figure 1), is a chemical agent that promotes facial rejuvenation. In addition, it causes coagulation of skin proteins, has an anesthetic effect on nerve endings, produces bacteriostatic effects when used in concentrations of up to 1%, and is bactericidal in higher concentrations.
Phenol-based peels were developed after the First World War. In England, scholars already used phenol to treat blemishes and scars, but the technique did not develop further. In the 1960s, new advances ushered in the era of peels using modified phenol solutions (with the addition of croton oil, septisol, and water) and histological evaluations of their results, allowing for comparisons between the effects of phenol and those of other peel subtypes.3 In 1962, Baker and Gordon discovered the current formula used in phenol peels, in which the substance is diluted in concentrations ranging from 45% to 55%.4,5
Its use requires thorough history taking and physical examinations as well as laboratory tests, since phenol is highly toxic and is absorbed systemically through the skin barrier. Phenol can cause local edema and erythema and has possible cardiac (tachycardia, ventricular extrasystoles, atrial and ventricular fibrillation, and electromechanical dissociation), renal, and hepatic side effects, and may cause central nervous system depression.4,5
In June 2024, Brazil’s National Health Surveillance Agency (Anvisa) issued Resolution no. 2384/2024, forbidding the importation, manufacturing, compounding, marketing, advertising, and use of phenol-based products in health or aesthetic procedures.6,7 Since then, phenol peels have been banned in Brazil, despite reports on its safety and effectiveness.
Therefore, the aim of this study is to conduct a literature review on the importance, safety, and effectiveness of phenol-based peels and their risks and benefits for patients. In addition, it provides information on current techniques, indications and contraindications for their use in treatment plans, and possible complications associated with their management.
This study is a descriptive and exploratory literature review conducted through searches in Google Scholar and PubMed databases. In Google Scholar, the search strategy used the DeCS descriptors “Abrasão Química” AND Fenol AND Rejuvenescimento. In PubMed, the Chemexfoliation AND Phenol AND Rejuvenation MeSH descriptors were used.
Full-text articles published between 2000 and 2025, in Portuguese or English, were included. Studies without published and available full text, those conducted on animal models, or those addressing different techniques and procedures, as well as duplicate articles, were excluded.
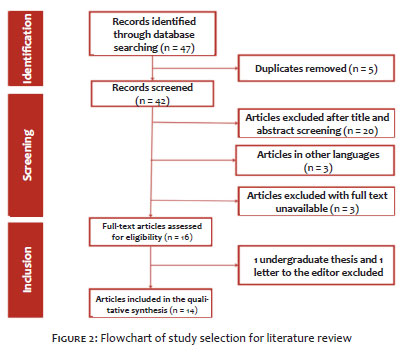
The initial search yielded a total of 47 results, 24 from Google Scholar and 23 from PubMed. Of these, 14 articles were included. Twenty-five studies were excluded based on their titles and 8 based on the abstract or full text (Figure 2).
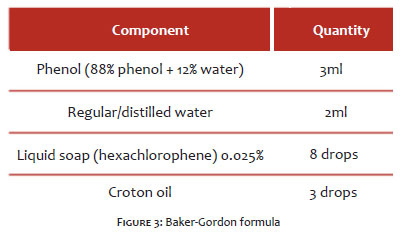
The Baker-Gordon formula, still the most widely used in phenol peels, contains components that enhance the activity of phenol on the skin, such as croton oil and liquid soap (Figure 3). In their absence, cellular regeneration tends to be less effective.4
Croton oil increases local vascularization, enhancing the keratocoagulative action of phenol and promoting deeper cutaneous infiltration.8 Because it is highly toxic to the skin, it can cause edema and local erythema. Liquid soap, in turn, acts as a tensoactive agent, primarily responsible for reducing the lipid surface tension of the skin, promoting emulsification and exfoliation and facilitating permeability.4
It is important to remove the lipid barrier and local hair before the procedure to ensure uniform penetration and minimize discomfort during the procedure. The face should be divided into sections, and the application begin with the largest area, using cotton or gauze. To avoid increasing toxicity, vigorous rubbing movements should be avoided. Contact time varies between 10 and 15 minutes per area.4,9
Studies show that phenol absorption through the skin can vary according to the pressure applied, the degree of friction, and exposure time. Fractionated application, with intervals between treated areas, is recommended to reduce systemic absorption and increase safety. Furthermore, phenol penetration is directly related to the composition of the formula, with croton oil and liquid soap being essential to optimize dermal diffusion and enhance clinical response.
Despite the development of new technologies in aesthetic dermatology, phenol peels remain relevant due to their relative simplicity and high efficacy, and are the most commonly used agents for deep chemical peels.10,11,12,13 The Baker formula, whether applied using a punctuated technique or to the entire face, is primarily indicated for the treatment of severe facial aging associated with sun exposure, characterized by deep rhytides.4,11,12 Studies report positive outcomes with the use of 88% phenol peels for rejuvenation of the perioral and periorbital regions.14,15
Phenol may also be used to treat scarring, particularly acne scars,12,16 and promotes skin-lightening. It also appears to be effective in addressing malignant and premalignant lesions such as actinic keratoses.11,14,15,16
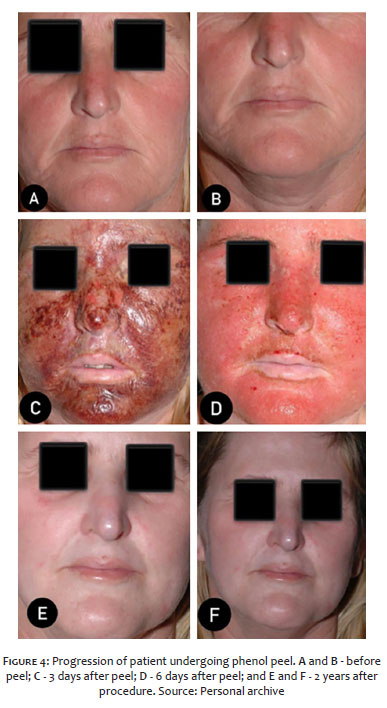
The efficacy of phenol was demonstrated in a clinical study assessing the punctuated application of 88% phenol to treat photoaging, which showed significant improvement in skin quality and histological reorganization of collagen fibers.10 A recent review highlighted that, even with the advent of modern techniques such as lasers and botulinum toxin, phenol remains a method of choice for static periorbital and perioral rhytides, producing superior results in certain cases15,18 (Figure 4).
Due to its action on the intermediate reticular dermis, phenol peels are highly painful procedures and must be accompanied by appropriate anesthesia and analgesia.11 Some studies report the use of hypnotic agents for conscious sedation.17 Analgesics may be prescribed for pain control following the procedure.4
Because it is a deep peel, phenol application leads to the formation of thick crusts, so post-peel care may require the use of vaseline-based moisturizers or topical antibiotics.4,11 Pruritus is a common side effect and can be alleviated with low-potency corticosteroids and cold compresses.11
After the procedure, an occlusive mask, generally made of adhesive tape or vaseline ointment, is applied and removed after 48 hours.4 Follow-up appointments in the first days and throughout the postoperative period are essential. Epidermal regeneration begins around 48 hours after the procedure, but full recovery may take up to 3 months.11,17
Despite extensive clinical practice, there is still no standardization regarding analgesia. Di Santis et al. observed that intense pain during the first 12 hours after the peel remains a challenge, with pain control largely relying on the practitioner’s experience rather than on an established protocol.17 Continuous monitoring in an appropriate clinical setting is also crucial given the risk of cardiovascular adverse events, even in patients with no comorbidities.20
Post-phenol peel complications are rare, particularly when performed by professionals familiar with the formula and application technique.18 Due to disruption of the skin barrier, there is a risk of secondary bacterial infection or herpetic eruption.4,9 Permanent deeper scarring may occur, especially in regions such as the lips, eyelids, and jawline.8,10 Therefore, it is important to assess the patient’s history of keloids prior to the procedure to anticipate potential unsightly scarring.9,17 Other possible complications include post-inflammatory hyperpigmentation, areas of depigmentation, and prolonged erythema.4,13,14,21 Small white cysts known as milia may also appear due to rapid re-epithelialization.4
Regarding systemic toxicity, cardiac, hepatic, and renal toxicities are of particular concern.11,19 A study assessing adverse effects associated with improper phenol use highlighted the importance of cardiotoxicity.19 In another retrospective study, phenol did not impair renal or hepatic function but was associated with arrhythmias in susceptible individuals, regardless of concentration or technique used.20 Even pre-screened and adequately hydrated patients may develop transient cardiac arrhythmias.9 Kadunc and Vanti emphasize the need for continuous ECG monitoring during the procedure,20 particularly in individuals with subclinical cardiovascular risk. Therefore, in addition to prior patient assessments with clinical and laboratory tests, it is advisable to space out phenol peel applications across different areas and ensure continuous intravenous hydration to facilitate proper metabolite elimination.4,11,19
Finally, the relationship between phenol and carcinogenesis remains unclear. One hypothesis suggests that certain formulations may have carcinogenic potential.9
Although the procedure has gained visibility in recent years, there are still few studies on phenol peels, and particularly few clinical studies. It is an aggressive approach with significant reported benefits, mainly in combating skin aging, and can be performed safely and effectively by knowledgeable physicians. Given the potential for systemic complications, such as cardiotoxicity and arrhythmias, and ongoing regulatory debates, the development of standardized safety protocols, proper monitoring, and careful patient screening are essential. Nevertheless, phenol peels remain a relevant and effective therapeutic alternative and deserve re-evaluation in light of more robust scientific evidence.
Gabriela Roncada Haddad
ORCID: 0000-0002-7516-9586
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Ana Carolina Salomão Gerolamo
ORCID: 0009-0001-4831-5728
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Critical review of the literature, Critical revision of the manuscript.
Nicole Dias Sbrissa
ORCID: 0009-0009-5425-3584
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Critical review of the literature, Critical revision of the manuscript.
José Ferreira de Oliveira Neto
ORCID: 0009-0000-8721-2732
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Effective participation in the conduct of the study, Critical review of the literature, Critical revision of the manuscript.
Ricardo Henrique Marcelino
ORCID: 0009-0003-4759-781X
Author’s contribution: Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Effective participation in the conduct of the study, Critical review of the literature, Critical revision of the manuscript.
Isabela Novello
ORCID: 0000-0002-2496-4475
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Effective participation in the conduct of the study, Critical review of the literature, Critical revision of the manuscript.
1. Oremović LBZSM. Chemical peelings--when and why? Acta Clin Croat. 2010:545-8.
2. Khunger N, Task Force IADVL. Standard guidelines of care for chemical peels. Indian J Dermatol Venereol Leprol. 2008;74(Suppl):5-12.
3. Brody HJ, Monheit GD, Resnik SS, Alt TH. A history of chemical peeling. Dermatol Surg. 2000;26(5):405- 9.
4. Velasco MVR, Okubo FR, Ribeiro ME. Rejuvenescimento da pele por peeling químico: enfoque no peeling de fenol. An Bras Dermatol. 2004;79(1):91-9.
5. Odo MEY, Chichierchio AL. Práticas em cosmiatria e medicina estética: procedimentos cirúrgicos de pequeno porte. São Paulo: Tecnopress; 1998.
6. Agência Nacional de Vigilância Sanitária. Anvisa proíbe venda e uso de produtos à base de fenol em procedimentos de saúde em geral ou estéticos [Internet]. 2024. Available from: https://www.gov.br/anvisa/pt-br/assuntos/noticias-anvisa/2024/anvisa-proibe-venda-e-uso-de-produtos-a-base-de-fenol-em-procedimentos-de-saude-em-geral-ou-esteticos
7. Agência Nacional de Vigilância Sanitária. Uso de fenol continua proibido para fins estéticos e outros não autorizados [Internet]. 2024. Available from: https://www.gov.br/anvisa/pt-br/assuntos/noticias-anvisa/2024/uso-de-fenol-continua-proibido-para-fins-esteticos-e-outros-nao-autorizados.
8. Hetter GP. An Examination of the Phenol-Croton Oil Peel: Part IV. Face Peel Results with Different Concentrations of Phenol and Croton Oil. Plast Reconstr Surg. 2000;105(3):1061–83.
9. Starkman SJ, Mangat DS. Chemical Peel (Deep, Medium, Light). Facial Plast Surg Clin North Am. 2020;28(1):45–57.
10. Mendonça MCC, Segheto NN, Aarestrup FM, Aarestrup BJV. Punctuated 88% phenol peeling for the treatment of facial photoaging: a clinical and histopathological study. Dermatol Surg. 2018;44(2):241–7.
11. Marta V, Maria T, Chisaki C, Benemond PH. Peelings químicos: revisão e aplicação prática. Surg Cosmet Dermatol. 2025;5(1):58–68.
12. Fabbrocini G, Padova M, Tosti A. Chemical Peels: what s new and what isn t new but still works well. Facial Plast Surg. 2009;25(5):329–36.
13. Atiyeh B, Oneisi A, Fadi Ghieh. Medium-depth trichloroacetic acid and deep phenol–croton oil chemical peeling for facial rejuvenation: an update. J Craniofac Surg [Internet]. 2021;32(8):e745–50.
14. Costa IMC, Peres AS, Costa MC, Figueira RBFC. Is there still a place for deep chemical peels in the treatment of perioral wrinkles? J Cosmet Dermatol. 2020;19(10):2634–6.
15. Antelo DAP, Vasconcellos JB, Orofino-Costa R. Estudo comparativo da aplicação regional de peeling de fenol e toxina botulínica: ainda um tratamento acessível e eficiente para rugas periorais e periorbitárias. Surg Cosmet Dermatology. 2020;12(3).
16. Fulton JE, Porumb S. Chemical Peels. American Journal of Clinical Dermatol. 2004;5(3):179–87.
17. Di P, Lopes B, Vieira R, Mandelbaum SH. Peeling profundo de fenol: como controlar a dor durante a aplicação e até 12 horas após? Surg Cosmet Dermatol. 2014;6(1):11–4.
18. Bagatin E, Hassun K, Talarico S. Revisão sistemática sobre peelings químicos. Surg Cosmet Dermatol. 2009;1(1):37–46.
19. Oliveira CN, Bisson GB, Ferreira Jr O. Adverse effects associated with the irresponsible use of phenol peeling: literature review. Oral Surg, Oral Med, Oral Pathol Oral Radiol. 2025;139(2):161–5.
20. Kadunc BV, Vanti AA. Avaliação da toxicidade sistêmica do fenol em peelings faciais. Surg Cosmet Dermatol. 2009;1(1):10–4.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}