


Doris Hexsel1; Lilia Maria Lima de Oliveira2; Indira Valente Bezerra1; Ana Carolina Krum dos Santos1; Camile Hexsel1,3,4; Fabio Saito5; Vitor Costa Fabris6
Funding: None.
Conflict of interest: Dr. Doris Hexsel serves as speaker and consultant for Galderma. Dr. Fabio Saito is an Associate Director for Customer Educataion & Training - Brazil and LATAM at Galderma. No other authors report conflicts of interest.
Submitted on: 03/18/2025
Final decision: 08/26/2025
How to cite this article: Hexsel D, Oliveira LML, Bezerra IV, Santos ACK, Hexsel C, Saito F, Fabris VC. Current evidence on the pathophysiological mechanisms of skin laxity: a narrative review. Surg Cosmet Dermatol. 2025;17:e20250453.
Skin laxity is defined as sagging and reduced tightness of the skin. A literature review was conducted using PubMed, Embase, and Cochrane databases to identify studies about skin laxity, focusing on causal mechanisms. Two main distinct processes of skin laxity have been previously reported, proposed here as superficial cutaneous laxity (SCL) and deep cutaneous laxity (DCL). SCL results from structural alterations in the dermis and leads to fine wrinkles and a superficial draped pattern. DCL is the result of subcutaneous sagging, mainly through relaxation and stretching of the complex formed by the adipose tissue, its septa, and the superficial fascia.
Keywords: Review; Skin; Skin Aging; Anatomy; Physiology
“Skin laxity,” “flaccidity,” “sagging,” “loose skin,” and “cutaneous laxity” are terms used to describe a loss of tightness in the skin and subcutaneous tissue. Clinically, it presents as redundant, loose, sometimes wrinkled and distended skin. It is a common complaint in both men and women, particularly at older ages.1
Flaccidity and wrinkles result from dermal alterations caused by the aging process,2,3 and from anatomical changes in the subcutaneous compartment, such as volumetric reduction of subcutaneous adipose tissue and laxity of cutaneous ligaments and fibrous septa.1,4
Previous studies on skin laxity have focused primarily on a single causal mechanism. This narrative literature review examines the ultrastructural and anatomical changes of the skin and subcutaneous tissue, describing their different clinical signs and proposing treatment options for each type of skin laxity. In addition, this study proposes an operational nomenclature based on clinical presentation: superficial cutaneous laxity (SCL) and deep cutaneous laxity (DCL).
Superficial cutaneous laxity is characterized by decreased skin elasticity, presenting as superficial lines, shallow furrows, and linear and draped patterns in the skin (Figure 1). This type of laxity is strongly associated with loss of epidermal thickness and dermal atrophy, frequent in aged patients, caused by structural alterations in the dermis.2,3
With aging, the epidermis and dermis, which are responsible for the mechanical properties and containment forces of the skin, undergo progressive atrophy and architectural disorganization.5,6 There is a decrease in fibroblast metabolic activity and in the synthesis of extracellular matrix (ECM) components, such as collagen, elastic fibers, proteoglycans, and glycosaminoglycans.7 Aging also leads to an increase in reactive oxygen species and increased matrix metalloproteinase (MMP) activity. MMPs are endopeptidases that degrade ECM proteins, and their increased activity contributes to further collagen and elastin fragmentation.2,7-9 The aged epidermis becomes thinner, the dermo-epidermal junction flattens, and the proliferative capacity of basal keratinocytes diminishes, leading the dermis to lose elasticity, tensile strength, and hydration.10 Consequently, superficial skin laxity is more pronounced in older patients and in sun-exposed areas such as the dorsum of the hands, neck, and face.11
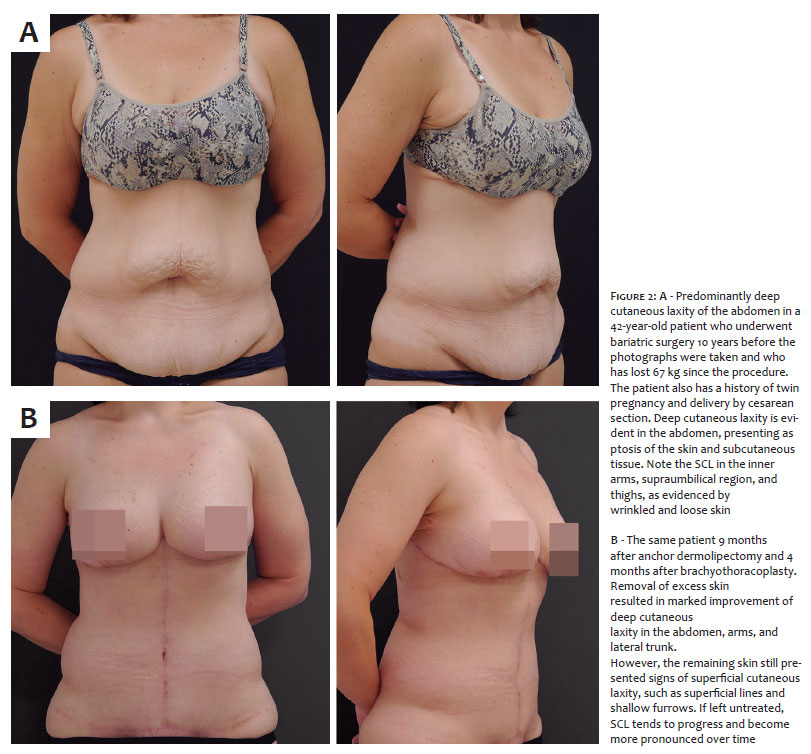
Deep cutaneous laxity is characterized by ptosis of the skin and subcutaneous tissue resulting from deep structural alterations in the subcutaneous compartments of the skin, including fat, muscles, fascia, and bones. This type of laxity is more pronounced in areas such as the abdomen, breasts, buttocks, and inner regions of the arms and thighs. On the face, signs of DCL are most noticeable in the eyelids, submental area, and prejowl sulcus.11-15 The same patient may present both SCL and DCL (Figure 2 A and B). To better understand DCL, it is necessary to review the structures that make up the subcutaneous compartment.
The subcutaneous adipose tissue consists of a superficial and a deep layer, separated by the superficial fascia, a membranous layer composed of fibroelastic tissue. The first layer, called superficial adipose tissue (SAT) or areolar tissue, comprises fat lobules encased in fibrous septa arranged in a honeycomb-like structure.15 These septa are well-defined, oriented perpendicularly to the skin, and firmly anchor the dermis to the membranous layer.14,15 They make up a stable and elastic structure that returns to its original position after distention in compression tests. This structure covers the entire body, and its thickness varies according to the amount of body fat.15,16
Beneath the SAT, the superficial fascia provides structural support for the skin and adipose tissue.14,15 Composed of wavy elastic fibers and collagen bands, this fascia is thicker closer to bony prominences, where it adheres more firmly. In some regions, the superficial fascia adheres more tightly to the musculoskeletal surface. In others, it is loosely attached, covering deeper fat deposits. Areas where this fascia is less adherent are more prone to DCL.17
The second layer, known as deep adipose tissue (DAT) or lamellar tissue, is located between the superficial fascia and the muscle fascia.15,16 This layer has loosely packed fat lobules, with less evident, obliquely oriented fibrous septa, which connect to the deep muscle fascia. DAT functions as an area for lipid deposition and is present only in specific regions, such as the abdomen, flanks, trochanteric regions, knees, posterior side of the arms, and upper third of the medial thighs. It varies in thickness across those areas, and is more fragile, less adherent, and more poorly vascularized than SAT.14-16
Excess accumulation of subcutaneous fatty tissue, more common in patients with higher BMIs, promotes a degenerative state that damages the neurovascular structures of the fascia. This triggers a fibrotic reaction in the subcutaneous adipose tissue that can lead to the development of lipedema.18,19
Aging, liposuction, and excessive weight fluctuations primarily affect the subcutaneous tissue by relaxing the complex formed by the adipose tissue and superficial fascia, as fat loss decreases the overall volume of the subcutaneous compartment.20,21 Depending on the region, different grades of subcutaneous laxity may be observed. Usually, sagging is greater in areas with poorer adherence, such as the abdomen and inner thighs.13-15
In the breasts and buttocks, DCL presents as loss of round contour, as gravitational forces redistribute sagging tissue downward, changing these regions from round to pendulous shapes. In the buttocks, DCL also causes the linear shape of cellulite depressed lesions and presents as fat accumulation in the lower part of the buttocks and gluteal ptosis, resulting in the widening of the infragluteal fold.22 In the medial and lower parts of the thighs, DCL causes the “curtain valance” appearance and fat deposition around the knees.11 DCL can also cause linear folds in thinner patients. In the arms, the decrease in the supportive structures along the inferior curve of the arm causes brachial ptosis and the formation of the brachial sulcus.12
SCL can be assessed objectively using noninvasive methods based on various physical principles, such as torsional power, suction generated by negative pressure, skin surface indentation, and acoustic shockwave emission.23 The Cutometer® MPA 580 (Courage and Khazaka, Koln, Germany) is frequently used to assess skin elasticity, particularly SCL.24, 25 It measures the capacity for skin indentation, which makes it especially suitable for assessing SCL. Other methods for measuring SCL include the pinch test26 and the placement of microtattoos on the skin for measurement purposes.27 The Skin Distension Test proposed by Hexsel et al. is also an easy-to-use, fast, reproducible, and inexpensive tool to measure SCL based on facial skin extension.28
Several scales assess skin laxity, including the Facial Laxity Grading Scale,29 the Classification of Brachial Ptosis,12 the Neck Skin Laxity Scale,30 the Merz Aesthetics Skin Laxity Grading Scales,11 and the Buttocks’ Skin Laxity Severity Scale.21 Most either combine SCL and DCL in their assessments or evaluate a single clinical sign of laxity. For example, the Neck Skin Laxity Scale and the Classification of Brachial Ptosis focus on DCL, while the Merz Aesthetics scales and the Facial Laxity Grading Scale combine both types in their assessments. The Buttocks’ Skin Laxity Severity Scale developed by Hexsel et al.21 grades the clinical signs of DCL in the gluteal region, where it is more common. Scales used in plastic surgery primarily assess DCL and the consequent soft-tissue ptosis, excess skin, and loss of body contour.31,32
Defining the best treatment for each patient requires a proper assessment of both SCL and DCL, as different treatment modalities are more suitable for each type of cutaneous laxity. A combined approach, using different scales and measurement options, is best suited for both clinical and research purposes.
The goals of treating SCL are to restore skin hydration and plumpness, stimulate the production of new collagen fibers, and reduce the oxidative stress caused by aging, giving the appearance of younger and healthier skin. It primarily targets the epidermis, dermis, and superficial subcutaneous tissue.
Topical treatments such as alpha-hydroxy acids, retinoids, ascorbic acid, peptides, and hyaluronic acids (HA) have traditionally been used in topical preparations to achieve these goals.
Improvements in skin atrophy, superficial wrinkles, and general skin smoothness have been reported.10 Mild outcomes can be achieved using chemical peels; results depend on agents used and depth of procedure. Chemical peels restore epidermal architecture, produce new collagen bands, and restore the elastic fiber network.33
Energy-based devices such as Intense Pulsed Light, fractional ablative and nonablative lasers and technologies, radiofrequency, and high-intensity focused ultrasound (HIFU) are useful for improving SCL. Skin resurfacing with fractional lasers heats the dermis, destroying specific layers of the epidermis and dermis with a controlled depth of thermal injury, promoting matrix remodeling and neocollagenesis.34 Radiofrequency has been suggested as an ancillary treatment for skin laxity, as it also promotes dermal heating, collagen formation, and tissue remodeling through thermal damage. However, there is no consensus in the literature regarding its efficacy.35 HIFU uses acoustic energy to induce coagulative necrosis through tissue heating, resulting in a tightening effect on the skin.36
Collagen biostimulators, such as injectable poly-L-lactic acid (PLLA), calcium hydroxyapatite, and polycaprolactone, are used in facial and body areas to induce neocollagenesis. These substances are usually injected into the superficial subcutaneous tissue to treat SCL. They induce a controlled foreign-body inflammatory response that activates fibroblasts and promotes neocollagenesis, improving the elasticity and overall skin quality in treated areas.37-39 Superficial HA fillers with low G prime, also known as skin boosters, and hybrid cooperative HA complexes can also be used to treat SCL, as they reduce fine lines on the skin.40-41
DCL treatment should address changes in the skin and deep subcutaneous tissue. Invasive surgical treatments for DCL include body contouring procedures to remove excess skin, targeted liposuction of fat deposits,21 and volume replacement using autologous fat grafts or prostheses.42-45 DCL can be evidenced and illustrated using plication sutures, frequently employed in plastic surgery and lifting procedures.
Nonsurgical options include HIFU, deeper filler injections, and biostimulators. Different regions require different treatment plans, usually combining treatments mentioned above, in order to achieve optimal results.
HIFU uses acoustic energy to deliver heat to the targeted tissue, causing coagulative necrosis to stimulate collagen remodeling. Depth of treatment can be adjusted to target deeper structures of the skin, such as adipose tissue, deep ligaments, and fibrous septa, making it suitable for DCL. Although improvements in skin laxity may be evident after a single session, optimal results are achieved with multiple sessions, 3 to 4 weeks apart. Improvement occurs gradually over 2 to 6 months post-treatment.42,43
Volume replacement can be done using prosthetics, fillers, or autologous fat grafts, as major volume losses can cause DCL, especially in older patients or after significant weight loss. HA fillers are the most frequently used agents. They are commercially available in formulations with different rheological properties that allow them to be injected into different anatomical depths, in different volumes, in order to achieve a wide variety of results. HA can be safely injected in most areas of the face and body for volume replacement and to provide support for the overlying structures of the skin, improving both SCL and DSL.44 In larger volumes, collagen biostimulators can also be used for volume replacement.
In recent decades, cosmetic threads emerged as a minimally invasive option to tighten sagging skin. Suture threads were followed by new materials, such as gold and PLLA threads. At the moment, polydioxanone (PDO) threads are the most widely used. Various PDO threads allow different treatments for facial and body SCL and DCL in patients with mild signs of aging.45,46
Based on this literature review, skin laxity can be categorized into two types, SCL and DCL. Both occur to varying degrees in cutaneous tissue and present distinct clinical features. SCL is secondary to epidermal and dermal changes associated with histological alterations related to the aging process, and is characterized by thinner, less elastic skin and the presence of superficial wrinkling. DCL results from deeper structural changes, mainly but not limited to subcutaneous tissues. Gravitational forces play a role in DCL, manifesting as ptosis of the skin and subcutaneous structures, causing the affected regions to develop a sagged and draped appearance. Both types can coexist in the same patient, but it is critical that clinicians accurately diagnose the laxity mechanisms and structures responsible for the patient’s main complaints in order to choose appropriate therapeutic approaches and optimize outcomes.
Doris Hexsel
ORCID: 0000-0002-0615-9026
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Lilia Maria Lima de Oliveira
ORCID: 0000-0002-5672-2649
Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Critical review of the literature, Critical revision of the manuscript.
Indira Valente Bezerra
ORCID: 0000-0002-4350-9080
Preparation and writing of the manuscript, Critical review of the literature.
Ana Carolina Krum dos Santos
ORCID: 0000-0001-9863-1836
Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Critical review of the literature, Critical revision of the manuscript.
Camile Hexsel
ORCID: 0009-0001-1184-6285
Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Critical review of the literature, Critical revision of the manuscript.
Fabio Saito
ORCID: 0000-0002-6487-5987
Author’s contribution: Preparation and writing of the manuscript, Critical revision of the manuscript.
Vitor Costa Fabris
ORCID:0000-0002-3540-2769
Author’s contribution: Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Critical review of the literature, Critical revision of the manuscript.
1. Hexsel DM. Body repair. In: Parish L, Brenner S, Ramos-e-Silva M. Women’s Dermatology: from infancy to maturity. Lancaster: Parthenon; 2001. p. 586-95.
2. Xia W, Quan T, Hammerberg C, Voorhees JJ, Fisher GJ. ‘A mouse model of skin aging: fragmentation of dermal collagen fibrils and reduced fibroblast spreading due to expression of human matrix metalloproteinase-1’. J Dermatol Sci. 2015;78(1):79-82.
3. Farage MA, Miller KW, Elsner P, Maibach HI. ‘Intrinsic and extrinsic factors in skin ageing: a review’. Int J Cosmet Sci. 2008;30(2):87-95.
4. Sakata A, Abe K, Mizukoshi K, Gomi T, Okuda I. ‘Relationship between the retinacula cutis and sagging facial skin’. Skin Res Technol. 2018;24(1):93-8.
5. Archer CB. ‘Functions of the skin’. In: Burns DA, Breathnach SM, Cox NH, Griffiths CEM. Rook’s Textbook of Dermatology, 8th ed. Oxford: Blackwells; 2010. p. 4.1-4.11.
6. Rudolph C, Hladik C, Hamade H, Frank K, Kaminer MS, Hexsel D, et al. ‘Structural gender dimorphism and the biomechanics of the gluteal subcutaneous Tissue: implications for the Pathophysiology of Cellulite’. Plast Reconstr Surg. 2019;143(4):1077-86.
7. Varani J, Dame MK, Rittie L, Fligiel SE, Kang S, Fisher GJ, et al. ‘Decreased collagen production in chronologically aged skin: roles of age-dependent alteration in fibroblast function and defective mechanical stimulation’. Am J Pathol. 2006;168(6):1861-8.
8. Pittayapruek P, Meephansan J, Prapapan O, Komine M, Ohtsuki M. ‘Role of Matrix metalloproteinases in photoaging and photocarcinogenesis’. Int J Mol Sci. 2016;17(6):868.
9. Weihermann AC, Lorencini M, Brohem CA, Carvalho CM. ‘Elastin structure and its involvement in skin photoageing’. Int J Cosmet Sci. 2017;39(3):241-7.
10. Shin JW, Kwon SH, Choi JY, Na JI, Huh CH, Choi HR, et al. ‘Molecular mechanisms of dermal aging and antiaging approaches’. Int J Mol Sci. 2019;20(9):2126.
11. Kaminer MS, Casabona G, Peeters W, Bartsch R, Butterwick K, Yen-Yu Chao Y, et al. ‘Validated assessment scales for skin laxity on the posterior thighs, buttocks, anterior thighs, and knees in female patients’. Dermatol Surg. 2019;45(Suppl 1):S12-S21.
12. El Khatib HA. ‘Classification of brachial ptosis: strategy for treatment’. Plast Reconstr Surg. 2007;119(4):1337-42.
13. Lockwood TE. ‘Superficial fascial system (SFS) of the trunk and extremities: a new concept’. Plast Reconstr Surg. 1991;87(6):1009-18.
14. Sbarbati A, Accorsi D, Benati D, Marchetti L, Orsini G, Rigotti G, et al. ‘Subcutaneous adipose tissue classification’. Eur J Histochem. 2010;54(4):e48.
15. Lancerotto L, Stecco C, Macchi V, Porzionato A, Stecco A, De Caro R. ‘Layers of the abdominal wall: anatomical investigation of subcutaneous tissue and superficial fascia’. Surg Radiol Anat. 2011;33(10):835-42.
16. Markman B, Barton FE Jr. ‘Anatomy of the subcutaneous tissue of the trunk and lower extremity’. Plast Reconstr Surg. 1987;80(2):248-54.
17. Frank K, Hamade H, Casabona G, Gotkin RH, Kaye KO, Tiryaki T, et al. ‘Influences of age, gender, and body mass index on the thickness of the abdominal fatty layers and its relevance for abdominal liposuction and abdominoplasty’. Aesthet Surg J. 2019;39(10):1085-93.
18. Sandhofer M, Schauer P, Pils U, Anderhuber F. ‘Fascia glutealis as mediator of musculocutaneous dynamics in the buttocks region’. J Ästhet Chir 2008; 12:6-13.
19. Sandhofer M, Schauer P, Anderhuber F. ‘Skin-subcutaneous-fat-fascia: Banal structures or complex architectural entities?’ J Ästhet Chir 2015; 8:151-6.
20. Orpheu SC, Coltro PS, Scopel GP, Gomez DS, Rodrigues CJ, Modolin ML, et al. ‘Collagen and elastic content of abdominal skin after surgical weight loss’. Obes Surg. 2010;20(4):480-6.
21. Mendez BM, Coleman JE, Kenkel JM. ‘Optimizing patient outcomes and safety with liposuction’. Aesthet Surg J. 2019;39(1):66-82.
22. Hexsel D, Valente-Bezerra I, Dal'Forno T, Camozzato F, Mosena G, Parizotto JT, et al. ‘Buttocks' skin laxity severity scale’. Dermatol Surg. 2022;48(6):648-52.
23. Woo MS, Moon KJ, Jung HY, Park SR, Moon TK, Kim NS, et al. ‘Comparison of skin elasticity test results from the Ballistometer(®) and Cutometer(®)’. Skin Res Technol. 2014;20(4):422-8.
24. Kim MA, Kim EJ, Lee HK. ‘Use of SkinFibrometer® to measure skin elasticity and its correlation with Cutometer® and DUB® Skinscanner’. Skin Res Technol. 2018;24(3):466-71.
25. Monteiro Rodrigues L, Fluhr JW; the EEMCO Group. ‘EEMCO Guidance for the in vivo Assessment of biomechanical properties of the human skin and its annexes: revisiting instrumentation and test modes’. Skin Pharmacol Physiol. 2020;33(1):44-60.
26. Sacks AC. ‘Grading system simplifies brachioplasty decisions’. Cosmetic Surgery Times 2003. p.8.
27. Alam M, Pongprutthipan M, Nanda S, Kim NA, Swary JH, Roongpisuthipong W, et al. ‘Quantitative evaluation of skin shrinkage associated with non-invasive skin tightening: a simple method for reproducible linear measurement using microtattoos’. Lasers Med Sci. 2019;34(4):703-9.
28. Hexsel D, Dal'Forno Dini T, Hexsel CL. ‘Skin distension test: a new simple tool to evaluate skin laxity’. Dermatol Surg. 2021;47(7):1026-7.
29. Silva HGL. ‘Facial laxity rating scale validation study’. Dermatol Surg. 2016;42(12):1370-9.
30. Guida S, Spadafora M, Longhitano S, Pellacani G, Farnetani F. ‘A validated photonumeric scale for the evaluation of neck skin laxity’. Dermatol Surg. 2021;47(5):e188-90.
31. Matarasso A. ‘Abdominolipoplasty: a system of classification and treatment for combined abdominoplasty and suction-assisted lipectomy’. Aesthetic Plast Surg. 1991;15(2):111-21.
32. Song AY, Jean RD, Hurwitz DJ, Fernstrom MH, Scott JA, Rubin JP. ‘A classification of contour deformities after bariatric weight loss: the Pittsburgh Rating Scale’. Plast Reconstr Surg. 2005;116(5):1535-44. Discussion 1545-6.
33. Ganceviciene R, Liakou AI, Theodoridis A, Makrantonaki E, Zouboulis CC. ‘Skin anti-aging strategies’. Dermatoendocrinol. 2012;4(3):308-19.
34. Badran KW, Nabili V. ‘Lasers, microneedling, and platelet-rich plasma for skin rejuvenation and repair’. Facial Plast Surg Clin North Am. 2018;26(4):455-68.
35. Araújo AR, Soares VP, Silva FS, Moreira Tda S. ‘Radiofrequency for the treatment of skin laxity: mith or truth’. An Bras Dermatol. 2015;90(5):707-21.
36. Laubach HJ, Makin IR, Barthe PG, Slayton MH, Manstein D. ‘Intense focused ultrasound: evaluation of a new treatment modality for precise microcoagulation within the skin’. Dermatol Surg. 2008;34(5):727-34.
37. Lacombe V. ‘Sculptra: a stimulatory filler’. Facial Plast Surg. 2009;25(2):95-9.
38. Goldie K, Peeters W, Alghoul M, Butterwick K, Casabona G, Chao YYY, et al. ‘Global consensus guidelines for the injection of diluted and hyperdiluted calcium hydroxylapatite for skin tightening’. Dermatol Surg. 2018;44(Suppl 1):S32-S41. Erratum in: Dermatol Surg. 2019;45(2):327.
39. Melo F, Nicolau P, Piovano L, Lin SL, Baptista-Fernandes T, King MI, et al. ‘Recommendations for volume augmentation and rejuvenation of the face and hands with the new generation polycaprolactone-based collagen stimulator (Ellansé®)’. Clin Cosmet Investig Dermatol. 2017;10:431-40.
40. Humzah D, Molina B, Salti G, Cigni C, Bellia G, Grimolizzi F. ‘Intradermal injection of hybrid complexes of high- and low-molecular-weight hyaluronan: where do we stand and where are we headed in regenerative medicine?’ Int J Mol Sci. 2024;25(6):3216.
41. Mazzoni D, Lin MJ, Dubin DP, Khorasani H. ‘Review of non-invasive body contouring devices for fat reduction, skin tightening and muscle definition’. Australas J Dermatol. 2019;60(4):278-83.
42. Khan U, Khalid N. ‘A systematic review of the clinical efficacy of micro-focused ultrasound treatment for skin rejuvenation and tightening’. Cureus. 2021;13(12):e20163.
43. Kapoor KM, Saputra DI, Porter CE, Colucci L, Stone C, Brenninkmeijer EEA, et al. ‘Treating aging changes of facial anatomical layers with hyaluronic acid fillers’. Clin Cosmet Investig Dermatol. 2021;14:1105-18.
44. O'Toole JP, Song A, Rubin JP. ‘The history of body contouring surgery’. Semin Plast Surg. 2006;20(1):5-8.
45. Lee W, Jung YC, Yang EJ. ‘Gluteal soft-tissue repositioning using polydioxane threads’. Dermatol Surg. 2021;47(7):e195-9.
46. De Masi EC, De Masi FD, De Masi RD. ‘Suspension Threads’. Facial Plast Surg. 2016;32(6):662-3.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}