


Decio Luis Portella; Hamilton Aleardo Gonella; Luciana Canabarro; Karine Helena Bocoli
Funding: None
Conflict of interest: None
Submitted on: 03/06/2025
Final decision: 08/26/2025
How to cite this article: Portella DL, Gonella HA, Canabarro L, Bocoli KH. Use of large-volume facial fat grafting in the treatment of Barraquer-Simons syndrome: A case report. Surg Cosm Dermatol. 2025;17:e20250448.
Barraquer-Simons syndrome is characterized by progressive atrophy of the subcutaneous cellular tissue limited to the upper part of the body. The condition manifests during childhood or adolescence. Usually, there is no previous family history and the etiology remains obscure. Fat grafting has been shown to be an effective, simple, safe and low-cost therapeutic approach in the treatment of this syndrome, but longer follow-up times are necessary to enable conclusions about long-term tissue preservation. Fat grafting allows wide diffusion of the method because it provides a less invasive treatment and good aesthetic results.
Keywords: Lipodystrophy, Familial Partial; Transplants; Face
Barraquer-Simons syndrome (BSS), also known as progressive partial lipodystrophy, is a rare condition characterized by the gradual and symmetric loss of subcutaneous fat in a cranio-caudal direction, affecting the face, neck, chest, and upper limbs.1-3
First described by Mitchell (1886) and later by Barraquer (1906) and Simons (1911), BSS usually manifests in childhood or adolescence, without a family history. It has been associated with viral infections, and genetic analyses point to a mutation in the LMNB2 gene, suggesting a genetic component linked to nuclear instability and the pathogenesis of the clinical presentation.4
BSS affects mostly women, who often present fat accumulation in the buttocks and lower limbs. In men, lipoatrophy predominates. Facial changes are the primary complaint, but 20% to 30% of patients present autoimmune diseases (such as lupus and glomerulonephritis) or neurological or metabolic manifestations (such as type 2 diabetes, dyslipidemia, and insulin resistance).5,6
BSS is classified into three subtypes: subtype I, associated with panniculitis; subtype II, associated with systemic diseases, mainly hypothyroidism, dermatomyositis, dermatitis herpetiformis, systemic lupus erythematosus, leukocytoclastic vasculitis, and mesangiocapillary glomerulonephritis; and subtype III (or idiopathic), which represents more than 50% of cases and is not associated with systemic diseases.7
There is no definitive cure for BSS.8 Treatment focuses on managing renal and autoimmune complications, as well as aesthetic interventions such as fat grafting, muscle flaps, and heterologous fat fillers.
Autologous fat grafting has proven to be an effective option, accessible in both private practice and public healthcare settings such as the Brazilian Unified Health System (SUS), as it is associated with low morbidity and improves facial contour and patient quality of life.9
To evaluate the effectiveness of autologous fat grafting for volumetric restoration and facial harmonization in a patient with Barraquer-Simons syndrome.
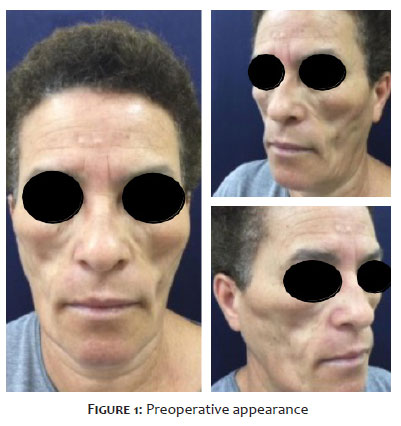
A 54-year-old female patient was admitted to the “Professor Linneu Mattos da Silveira” Plastic Surgery Service in Sorocaba, São Paulo, for evaluation and specialized treatment. She reported progressive adipose tissue atrophy since childhood. The process began in the middle third of the face and later extended to the temporal and bilateral orbital regions, eventually progressing to the upper thorax. She denied comorbidities, similar family history, alcohol consumption, smoking, drug use, or other systemic complaints.10 Physical examination revealed major lipoatrophy (loss of adipose tissue) involving multiple body areas, more pronounced bilaterally in the middle third of the face, producing localized depressions. In addition to the face, physical examination also found the cervical region (neck) and upper thorax were also affected.
Treatment consisted of two fat-grafting sessions, spaced 4 months apart, following the structural Coleman technique.10 Using a 3-mm cannula attached to a 20-mL Luer Lock syringe, 100 mL of abdominal fat were harvested and processed by decantation for 15 minutes. After antisepsis with chlorhexidine and placement of surgical drapes, local anesthetic infiltration was performed with lidocaine 0.4%, bupivacaine 0.0005%, and epinephrine 1:200,000, in accordance with maximum doses of lidocaine (7 mg/kg) and bupivacaine (2 mg/kg) in the facial recipient areas. Grafting was performed with a 1.2-mm microcannula attached to a 5-mL syringe, injecting small amounts of fat into multiple tunnels to maximize contact with the recipient tissue. In the first session, approximately 80 mL of fat was grafted into various facial regions; in the second session, 90 mL was grafted following the same protocol. After each procedure, micropore dressings and compression were applied to the liposuctioned area for 7 days. The patient remained under observation for 3 hours and was discharged in the absence of complications in the donor and recipient areas.
Figure 1 shows major facial lipoatrophy, most apparent in the middle third of the face, with signs of facial aging and masculinization.
The patient presented with lipoatrophy of the cervical region, upper third of the thorax, and proximal upper limbs, without involvement of the abdominal region, as shown in figure 2.
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki. Although a formal informed consent form was not used, all participants were previously informed about the objectives, procedures, and possible implications of the research. Verbal authorization was obtained and documented in the medical record through a medical reliability statement, ensuring that clinical data and any images used would be kept confidential and employed exclusively for scientific purposes. The study was approved by the medical team in charge and follows the criteria of confidentiality, anonymity, and non-exposure of participants.
The patient was diagnosed with BSS, subtype III.
Fat grafting provided a considerable improvement in facial contour, with the near-complete disappearance of depressions and irregularities. There was an initial resorption of 40% of the grafted fat, but the results were maintained after the second session, with a 5-month follow-up.
Areas such as the malar and orbital regions showed remarkable harmonization, reducing the appearance of hollow eyes and facial masculinization (Figures 3 and 4). At the 7-day postoperative mark, there was substantial improvement in facial symmetry and harmony between the facial thirds, with adequate malar filling.
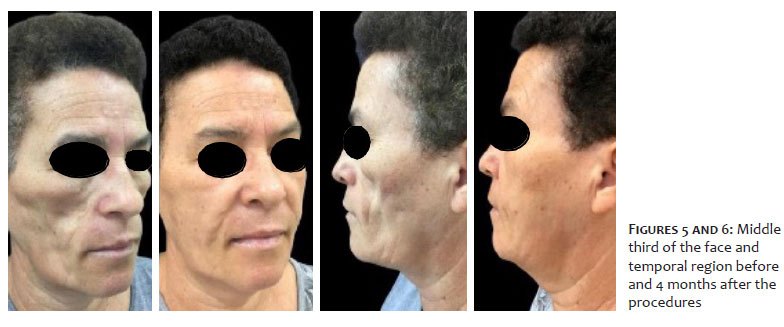
In figures 5 and 6, corresponding to the 4-month postoperative mark, a loss of filling in the middle third of the face and temporal region can be observed, with partial loss of the grafted volume. However, the facial lines and depressions are clearly smaller compared with the preoperative images.
Restoring facial contour in cases of lipodystrophy can be performed using different techniques, each with specific advantages and limitations. Among the available options are the use of alloplastic materials and fillers such as polymethyl methacrylate (PMMA), which are regulated and authorized for use under specific conditions and indications, such as in reconstructive plastic surgery, in addition to autologous tissues, whether devascularized or vascularized. Selection of the optimal treatment must take into account the individual needs of the patient, the severity of the lipodystrophy, and the surgeon’s preferences.11
Lipofilling, or autologous fat grafting, is widely used due to its effectiveness, safety, and relatively low cost. It consists of harvesting fat from donor areas, such as the abdomen or thighs, which is then processed and injected into the areas affected by lipodystrophy.8 One of its main advantages is that using the patient’s own tissue eliminates the risk of rejection. However, part of the grafted fat may undergo resorption, requiring multiple sessions to achieve satisfactory results.8
Patients with progressive lipodystrophy often seek treatment at advanced stages of the disease, when they present marked facial characteristics such as volume loss in the temporal, infra-malar, and periorbital regions. These losses accentuate concavities, producing an appearance of premature aging due to fat loss.12
Therapeutic options for correcting facial lipoatrophy include facial reconstruction techniques such as fat grafting and filling with substances like poly-L-lactic acid or PMMA. In more severe cases, particularly those involving metabolic alterations, pedicled or free flaps may be used. In addition, recombinant leptin has been used to assist in regulating glucose metabolism and adipocyte storage.2
Fat grafting involves transferring fat from one area of the body to another, using low negative pressure for aspiration and injecting small amounts of fat through multiple tunnels. This favors integration with the recipient tissue and minimizes risks and complications.2
During filler procedures or adipose tissue grafting, specific technical precautions are essential to minimize the risk of aesthetic complications such as overcorrection, irregularities, asymmetries, and nodules, since adequate preservation of viable adipocytes is crucial for success. This is especially true in autologous fat grafting techniques, in which adipocyte preservation is favored by several technical measures, such as: Gentle fat aspiration with cannulas of appropriate diameter, avoiding excessive negative pressure; Delicate processing of adipose tissue, without vigorous centrifugation or prolonged exposure to air; Avoiding mechanical trauma during injection by using blunt cannulas and retrograde injection in multiple planes; Implanting small volumes per tunnel, ensuring greater surface contact with the recipient bed and, therefore, better integration and revascularization.2,3
During the 5-month follow-up period, two fat-grafting sessions were performed, with preservation of grafted volume after an initial loss estimated at 40%. No intercurrences or complications were reported, demonstrating the effectiveness and safety of the treatment. The simplicity of the procedure and the absence of a need for special materials significantly reduce cost, which favors its wide adoption.9
Alternatives such as the use of free or microsurgical flaps, including the rectus abdominis muscle flap, deep inferior epigastric artery perforator (DIEP) flap, and anterolateral thigh flap, may also be considered. However, these techniques may result in donor-site scarring, ptosis, hernias, and local reactions, in addition to generally presenting high cost, which limits their use in many centers.10,12,13
Autologous fat grafting stands out as a valuable treatment option for reducing the stigma associated with facial lipodystrophy, providing aesthetic benefits and improving patient quality of life. Early diagnosis and continuous treatment are essential to prevent the disease from progressing to advanced stages, in which physical and psychological changes become more difficult to manage.10,12,13
Fat grafting proved to be an effective and low-cost therapeutic approach for treating BSS, promoting aesthetic and psychological improvements. Although long-term studies are needed to assess the durability of results, the method stands out for its simplicity and safety, making it widely applicable in both public and private health care settings. The technique offers a less invasive and more accessible alternative for patients with this rare condition.
Decio Luis Portella
ORCID: 0000-0002-7375-4407
Statistical analysis, Approval of the final version of the manuscript, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical revision of the manuscript
Hamilton Aleardo Gonella
ORCID: 0000-0001-9302-2919
Approval of the final version of the manuscript, Conception and design of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature
Luciana Canabarro
ORCID: 0000-0003-1461-3695
Statistical analysis, Preparation and writing of the manuscript, Effective participation in the conduct of the study, Critical review of the literature, Critical revision of the manuscript
Karine Helena Bocoli
ORCID: 0009-0001-1476-4904
Acquisition, analysis and interpretation of data
1. Santos M, Rabelo R, Vilasboas V, Talhari S. Do you know this syndrome? An Bras Dermatol. 2011;86:391.
2. Franco FF, Spencer LB, Mendes FD, Lopes RG, Braga EVB, Pinheiro AF, et al. Tratamento cirúrgico do paciente com síndrome de Barraquer-Simon: revisão bibliográfica e relato de caso. Rev Soc Bras Cir Craniomaxilofac. 2007;10:152-5.
3. Mansouri HN, Lahmiti S, Aimadeddine S. Barraquer Simons syndrome. Rev Stomatol Chir Maxillofac. 2011;112:172-3.
4. Hegele RA, Cao H, Liu DM, Costain GA, Charlton-Menys V, Rodger NW, et al. Sequencing of the reannotated Lmnb2 gene reveals novel mutations in patients with acquired partial lipodystrophy. Am J Hum Genet. 2006;79(2):383-9.
5. Ferrarini A, Milani A, Bottigelli M. Two new cases of Barraquer-Simons syndrome. Am J Med Genet A. 2004;126:427-9.
6. Misra A, Peethambaram A, Garg A. Características clínicas e desequilíbrios metabólicos e autoimunes na lipodistrofia parcial adquirida: relato de 35 casos e revisão da literatura. Medicina (Baltimore). 2004;83:18–34.
7. Requena Caballero C, Angel Navarro Mira M, Bosch IF, Bauxauli JM, Aliaga Boniche A. Barraquer-Simons lipodystrophy associated with antiphospholipid syndrome. J Am Acad Dermatol. 2003;49:768-9.
8. Cedrola JPV, Castro CC, Aboudib JH, Turini T, Castro M, Serra F. Análise do tratamento da síndrome de Parry-Romberg por lipoenxertia estruturada no Hospital Universitário Pedro Ernesto HUPE-UERJ. Rev Bras Cir Plást. 2011;26(Suppl):1-102.
9. Ducours JL, Poizac P, Ardanza B, Modschiedler T, Caix P. Barraquer- Simons syndrome and facial lipo-filling. apropos of a case. Rev Stomatol Chir Maxillofac. 1991;92(2):105-11.
10. Coleman SR. Structural fat grafting. In: Bartlett SP, Beasley RW, Aston SJ, Gurtner GC, Scott L, Spear SL, ed. Grabb and Smith’s plastic surgery. 6th ed. Philadelphia: Lippincott Williams & Wilkins/Wolters Kluwer; 2006. p. 480- 5.
11. Spranger S, Spranger M, Tasman AJ, Reith W, Voigtländer T, Voigtländer V. Barraquer-Simons syndrome (with sensorineural deafness): a contribution to the differential diagnosis of lipodystrophy syndromes. Am J Med Genet. 1997;71(4):397-400.
12. Panse I, Vasseur E, Raffin-Sanson Ml, Staroz F, Rouveix E, Saiag P. Lipodystrophy associated with protease inhibitors. Br J Dermatol. 2000;142:496-500.
13. Dornelas MT, Corrêa MPD, Netto GM, Barra FML, Alves SGS, Dornelas MC, et al. Bioplastia na lipodistrofia de pacientes com Hiv/Aids. Rev Bras Cir Plást. 2012;27(3):387-91.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}