


Soraya Neves Marques Barbosa dos Santos; Sílvia Iovine Kobata; Isabela Boechat Morato; Natália de Paiva Sobreira
Funding: None.
Conflict of interest: None.
Submitted on: 09/18/2024
Final decision: 02/27/2025
How to cite this article: Santos SNMB, Kobata SI, Morato IB, Sobreira NP. Onychomatricoma: always a diagnostic challenge. Surg Cosmet Dermatol. 2025;17:e20250408.
Onychomatricomas are rare and benign tumors of the nail apparatus. Clinical findings, dermoscopic features and possibly imaging and histopathology exams confirm the diagnosis. We report the case of a 15-year-old male patient who had undergone multiple previous treatments for other diagnoses with no response. The transverse hypercurvature and digitiform projections on the nail plate, complemented by histopathological analysis, confirmed the hypothesis of onychomatricoma. The relevance of proper diagnosis and therapeutic management in these cases spares the patient and optimizes the use of public resources that would otherwise be spent on countless consultations and the long period until diagnosis.
Keywords: Neoplasms, Adnexal and Skin Appendage; Nails; Onychomycosis; Nails, Malformed.
An onychomatricoma (OM) is a rare and benign tumor of the nail apparatus, of unknown origin, found primarily in the nail matrix of the fingers. The classical clinical presentation includes a thick yellow band on the nail plate, tending toward transverse hypercurvature, often accompanied by findings of splinter hemorrhage and cavitations in the distal portion of the nail plate.1-3 Generally asymptomatic and rarely associated with chronic paronychia, OMs may cause severe pain and impair quality of life.2 In the literature, we find several reports of patients with long care pathways before proper diagnosis and treatment.4,5 This article reports on a clinical case referred to the dermatology department, treated for years as onychomycosis but with a clinical and histopathological diagnosis matching OM. Clinical and complementary criteria for an earlier and more assertive diagnosis are discussed below.
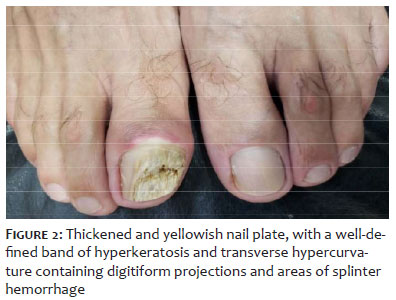
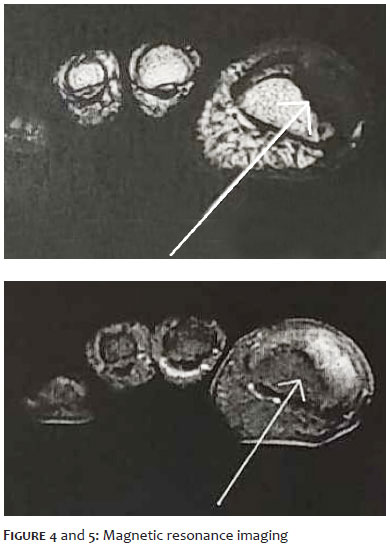
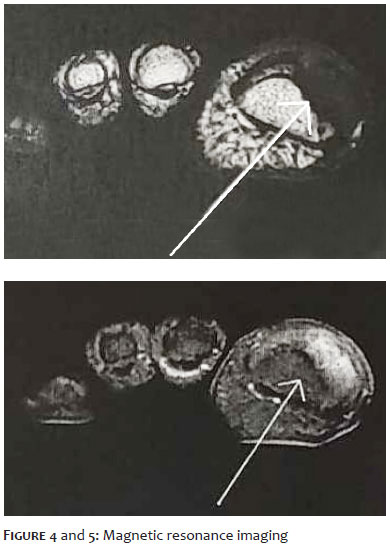
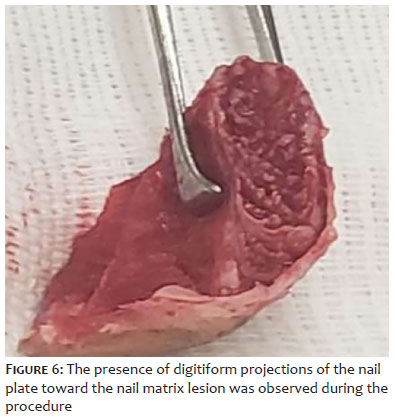
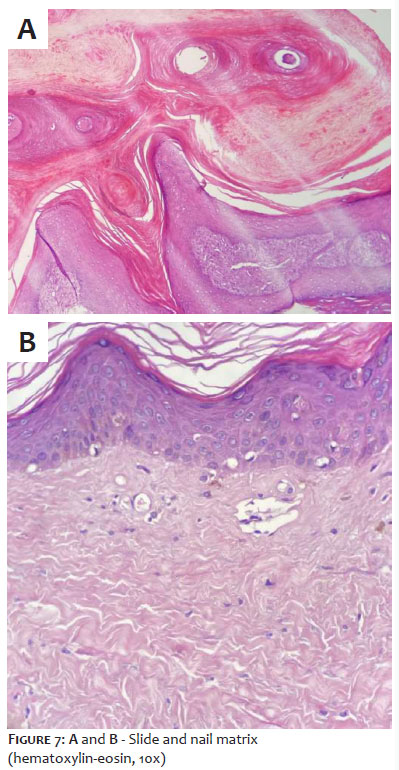
A patient, Caucasian, male, 48 years old, employed as an information technology assistant, visited the dermatology department complaining of an alteration in the thickness and coloring of the nail on the right hallux. The alteration began approximately 15 years earlier, and had been accompanied by intense pain for 1 year, with progressive worsening and impaired walking. The patient had undergone several earlier treatments for onychomycosis, such as oral terbinafine and topical antifungal medications, without improvement. He reported episodes of acute pain with drainage of purulent periungual secretion requiring systemic antibiotic therapy on several occasional, as well as frequent use of nonsteroidal anti-inflammatory drugs for pain relief. Upon dermatological examination, the right hallux was found to have a thickened and yellowish nail plate, with a well-defined band of hyperkeratosis and transverse hypercurvature containing digitiform projections and areas of splinter hemorrhage, more clearly seen in dermoscopy. There was also edema and warmth of the proximal nail fold (Figures 1 and 2). Direct mycological examination of the nail bed was negative, but a culture found growth of Trichophyton mentagrophytes. In an X-ray of the right hallux (Figure 3), there was doubt regarding the presence of a punched-out lesion of the distal phalanx in the area underlying the nail injury. Magnetic resonance imaging of the right hallux was requested (Figures 4 and 5), showing an oval injury to the nail matrix, hypointense on T1 and with heterogeneous signal on T2, with poorly-defined limits and no soft tissue infiltration, but also found remodeling of the bone contour. A surgical approach with excisional biopsy of the lesion to confirm the diagnosis was chosen. The procedure consisted of a distal anesthetic block, detachment of the nail plate, and exeresis of an exophytic lesion measuring 1.5 cm by 0.5 cm in the nail matrix. The presence of digitiform projections of the nail plate toward the nail matrix lesion was observed during the procedure (Figure 6). Histopathological analysis using hematoxylin and eosin staining found nail plate cavitations filled with plasma and fibroepithelial tumor with digitiform projections of the matrix epithelium and interspersed mastocytes, compatible with the diagnosis of OM (Figures 7 A, B).
OMs are rare and benign fibroepithelial tumors of the nail matrix and still represent a diagnostic challenge. Originally described by Baran and Kint in 1992,6 OM shows peculiar CD34 expression in the connective tissue portion.2,7 The incidence is higher in Caucasians, with more reports among women, though some authors claim they are not more frequent in either sex. It occurs mainly around the fifth decade of life, but there are case reports in children.7,8 The fingernail matrix is affected more often (63%), with the index finger accounting for two-thirds of cases; toes are affected in 36% of cases. Multiple fingers and toes may be affected simultaneously, but that is unusual.2
Clinical features consist of a well-demarcated portion of the nail plate with evident thickening, presence of splinter hemorrhage, transverse hypercurvature, and xanthonychia, the latter the most frequent sign, found in a little over 50% of all cases.2 Other characteristics include: erythema and edema of the proximal nail fold, prominent longitudinal groove, onychodystrophy, and dorsal pterygium.2,9 Pain may or may not be associated with the condition. Digitiform projections after surgical avulsion of the nail plate are highly suggestive.5 The primary differential diagnoses are fibrokeratoma and periungual fibroma, but also include squamous cell carcinoma, Bowen's disease, subungual verruca vulgaris, keratoacanthoma, osteochondroma, and fungal and bacterial infections. It may also present with associated longitudinal melanonychia, with the differential diagnosis including disorders of proliferation and activation of nail matrix melanocytes.2 OM and onychomycosis frequently coexist, since cavitations make the nail plate more susceptible to secondary fungal infections. OM cases are frequently treated as onychomycosis, leading to delayed diagnosis and unnecessary use of ineffective medications.10,11 Therefore, the finding of septate hyaline hyphae upon direct mycological examination and fungal growth in culture media do not rule out OM, and the absence of response to standard therapy should suggest the hypothesis of other differential diagnoses.4 Dermoscopy evidences thickening of the nail plate with multiple honeycombed cavitations (70%), hemorrhagic striae (72%), and white longitudinal grooves corresponding to nail plate channels (71%). Honeycombed cavitations may be filled by yellowish or red-black pigmentation material. While the patterns of plaque thickening and splinter hemorrhage do not have high specificity and may be present in isolated cases of onychomycosis, the presence of parallel longitudinal white grooves associated with lateral demarcation of the lesion and honeycombed cavitations have high specificity.2,4,5,7,12 Complementary tests may be requested to rule out skeletal involvement and explore the presence of OM, but they are not required for diagnostic confirmation. Ultrasonography has higher predictive value when performed by an experienced professional and may find hypoechoic areas on the nail matrix with adjacent hyperechoic linear areas corresponding to digitiform projections.5,11 Radiography of the affected finger or toe is easily available and may rule out skeletal involvement, but it does not show typical signs for a conclusive diagnosis. Magnetic resonance imaging, although not routinely necessary, shows low signal uptake in the lesion and in the nail matrix and high uptake of adjacent signal corresponding to tumor projections.3,5 In this case report, the radiograph showed an equivocal image of the distal phalanx of the right hallux, which might correspond to skeletal involvement (punched-out lesion), so a second imaging examination was requested before the surgical procedure to enable better planning. In terms of histology, OM are fibroepithelial tumors comprising two distinct parts. The proximal zone is characterized by having deep epithelial invaginations occupied by overlapping nail protrusions. The distal zone corresponds to epithelial digitations originating from the matrix epithelium, which proliferate and cause perforations in the nail plate.2,13,14 Immunohistochemistry is of great diagnostic aid, with OM positive for CD34, whereas CD99 markers, S-100 protein, epithelial membrane antigen, actin, and desmin are negative.1 Clinical suspicion combined with complementary examinations, such as radiography, ultrasonography, magnetic resonance imaging, and dermoscopy, are valuable, but diagnosis can only be confirmed by histopathological analysis.5,7 Treatment consists of full surgical excision of the tumor, including the normal nail matrix proximal to the lesion to prevent local relapse. Though a benign tumor, long-term follow-up is recommended due to the risk of relapse. Permanent nail dystrophy is not an infrequent complication.2,15 Despite classical clinical and intraoperative characteristics, the lack of knowledge about the condition and its tendency to be asymptomatic contribute to late diagnosis. Given what appears to be a case of intractable onychomycosis associated with transverse hypercurvature, nail thickening, and splinter hemorrhages, underlying OM should be suspected.
Soraya Neves Marques Barbosa dos Santos
ORCID: 0000-0001-5138-8584
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Sílvia Iovine Kobata
ORCID: 0000-0002-9079-6940
Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Isabela Boechat Morato
ORCID: 0000-0002-2542-4454
Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied.
Natália de Paiva Sobreira
ORCID: 0000-0002-8460-1289
Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied.
1. Figueiredo LA, Ribeiro RS, Melo ALB, Lima AL, Terra BB, Ventim FC. Polypropylene prosthesis for the treatment of fingertip injuries. Description of surgical technique and results. Rev Bras Ortop. 2017;52(6):685-92.
2. Carrai LHM, Rodrigues EF, Lima TFM, Sasseron MGM, Gomes Neto A. Delayed surgical closure (secondary intention) using the Figueiredo Technique: a case series study. Surg Cosmet Dermatol. 2023;15:e20230212.
3. Muniz AAS, Muniz MT, Figueiredo LA, Figueiredo PH, Oliveira BG. Use of the Figueiredo Technique for the treatment of ring avulsion injury: a case report. BioRes Scientia. 2024;2(2):1-4.
4. Figueiredo LA, Ribeiro RS, Figueiredo PH, Lima ALM, Oliveira FM, Oliveira Júnior DS. Comparison between Atasoy-Kleinert V-Y Advancement Flap and Figueiredo Techniques for the treatment of transverse and dorsal oblique fingertip injuries. Rev Bras Ortop. 2022;59(5): e712–e718.
5. Carvalho RSS, Leitão Júnior PSL, Dias Neto VS, Souza IGL, Rosal LCF, Gomes ACS. Use of polypropylene prosthesis using the Figueiredo Technique for treating thumb degloving in the interior of Minas Gerais – case report. Braz J Health Rev. 2024;7(3):1-11.
6. Sin-Soler M, Yébenes M, Gamissans M, Riera-Martí N, Lara A, Sàbat M. The use of bone wax versus dermal regeneration matrix for the reconstruction of scalp defects. Int J Dermatol. 2024;63(9):1236-41.
7. Becker GD, Adams LA, Levin BC. Secondary intention healing of exposed scalp and forehead bone after Mohs surgery. Otolaryngol Head Neck Surg. 1999;121(6):751-4.
8. Wong N, Zloty D. Secondary intention healing over exposed bone on the scalp, forehead, and temple following Mohs micrographic surgery. J Cutan Med Surg. 2022;26(3):274-9.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}