


Juliana Senna Figueiredo Barbi1; Marina Vieira Rodrigues Queiroz2; Karoline Kalinca Rabelo Santana3; Gustavo Carneiro Nogueira4
Funding support: None.
Conflicts of interest: None.
Submitted on: 20/06/2024
Approved on: 21/11/2024
How to cite this article: Barbil JSF, Queiroz MVR, Santana KKR, Nogueira GC. Upper and lower blepharoplasty combined with phenol-croton oil peel for facial rejuvenation: a clinical case report. Surg Cosmet Dermatol. 2025;17:e20250381.
Blepharoplasty is often the first facial aesthetic surgery sought by patients. However, in cases of more advanced aging, blepharoplasty alone may not achieve the desired aesthetic result, requiring the combination of additional rejuvenation techniques. Phenol-croton oil peeling is an excellent adjunct to eyelid surgery, as it effectively addresses deep rhytides. This case report describes a patient treated with combined upper and lower blepharoplasty and full-face phenol-croton oil peel, resulting in a highly satisfactory facial rejuvenation outcome.
Keywords: Blepharoplasty; Phenol; Croton Oil; Rejuvenation.
Blepharoplasty is a surgical procedure aimed at rejuvenating the upper and/or lower eyelids. It is often one of the first aesthetic interventions sought by patients pursuing facial rejuvenation. Technically delicate, blepharoplasty requires careful planning and meticulous execution to achieve optimal results and minimize complications.1 Upper eyelid blepharoplasty is typically performed for both aesthetic and functional reasons, whereas lower eyelid blepharoplasty is more commonly indicated for cosmetic purposes.2
However, improving the periocular region alone may be insufficient for full facial rejuvenation, and adjuvant aesthetic treatments are often necessary. In this context, phenol-croton oil peel is an effective option for treating deep facial rhytides.3 This technique involves a deep chemical peel whose level of skin penetration depends on factors such as the volume applied and the concentration of phenol and croton oil in the formulation. When appropriately indicated and correctly performed, this procedure yields marked improvements in skin quality and wrinkle reduction compared to other methods.3
Because it reaches the reticular dermis, phenol-croton oil peel promotes the formation of a dense dermal neocollagenesis zone, where newly organized elastic fibers replace elastosis and melanin granules are reduced.4 Histologic studies of skin treated with phenol-croton oil peel have shown increased collagen density in the papillary and reticular dermis, due to the stimulation of type I and III collagen.5 As such, phenol-croton oil peels are effective in softening or eliminating deep wrinkles and may serve as valuable adjuncts to facial rejuvenation surgery.6
This report presents a clinical case of a patient with significant facial aging who was treated with combined upper and lower blepharoplasty and full-face phenol-croton oil peel, resulting in substantial aesthetic improvement. This study was reviewed and approved by the Human Research Ethics Committee (CEP) under approval number 5.608.414.
N.P.D., a 67-year-old White female from Belo Horizonte, MG, was evaluated at the oculoplastic surgery outpatient clinic of the Hilton Rocha Eye Hospital with complaints of excess skin on the upper and lower eyelids of both eyes, as well as facial wrinkles. She had a history of hypertension, type 2 diabetes, and dyslipidemia, and was taking losartan 100 mg/day, metformin 850 mg/day, and simvastatin 20 mg/day.
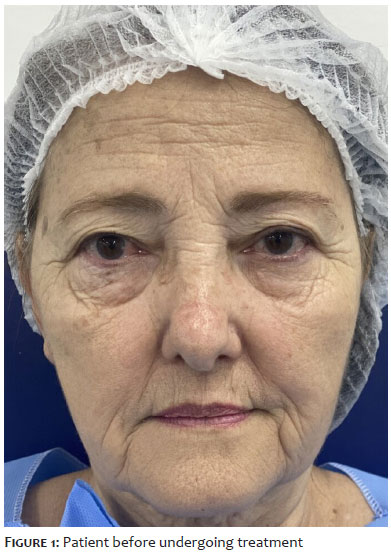
Dermatologic assessment revealed a pattern of aging characterized predominantly by extrinsic factors, with significant photoaging. The patient exhibited minimal facial deflation and well-defined mandibular contour (Figure 1). Oculoplastic examination showed upper and lower eyelid dermatochalasis, with prolapse of the medial fat pads in the upper eyelids and medial, central, and lateral fat pads in the lower eyelids, as demonstrated in Figure 1. Snap-back and distraction tests indicated horizontal laxity of the lower eyelids.
On January 25, 2022, upper and lower blepharoplasty was performed using radiofrequency (Wavetronic 5000 – 110 volts) in "cut" mode for skin incisions (80% cut, 20% coagulation) and "blend" mode for dissection (50% cut, 50% coagulation). After asepsis, local anesthesia was administered with lidocaine and bupivacaine combined with a vasoconstrictor at 2%.
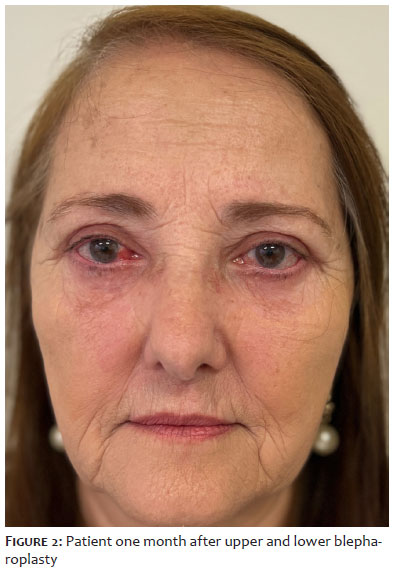
For the upper eyelids, skin incisions were made along premarked lines, preserving the orbicularis muscle, followed by resection of the medial fat pad. For the lower eyelids, a subciliary incision was made to excise a myocutaneous flap (excess skin and a band of preseptal orbicularis muscle). The medial, central, and lateral fat pads were resected. Canthopexy was performed using 5-0 polypropylene sutures, and skin closure was completed with 6-0 nylon sutures. The procedure lasted one hour and was uneventful. Sutures were removed on postoperative day 10. The result 30 days after surgery is shown in Figure 2.
After 105 days, the patient underwent full-face phenol-croton oil peel. The procedure was performed in an operating room under appropriate cardiorespiratory monitoring, intravenous hydration with Ringer's lactate, and conscious sedation using a combination of midazolam, fentanyl, and ketamine, under the supervision of an anesthesiologist.
The phenol-croton oil solution used was Hetter's 1.6% formula, consisting of 2.75 mL distilled water, 0.25 mL Novisol, and 2 mL of stock solution (0.08 mL croton oil and 1.92 mL of 88% phenol solution), yielding a total of 5 mL for facial application.
The technique began with facial degreasing using pure acetone, followed by demarcation of treatment zones using a white pencil or surgical marker. The face was divided into five zones: forehead, nose, perioral region, malar area, and periocular region, with careful delineation of the mandibular line.
A handmade applicator, which was a wooden stick wrapped with cotton at one end, was dipped into the solution. Then, the excess was removed, and the applicator was applied to the face. The solution was spread generously to keep the area moist, and the applicator was gently rubbed across the skin while the other hand stabilized the area. In regions with deep rhytides, more vigorous rubbing was performed to enhance penetration. Each facial zone was treated sequentially with a 15- to 20-minute interval between applications, resulting in a total procedure time of at least one hour, which helps minimize systemic phenol toxicity.
Immediately after application, a solid white frost appeared on the skin, followed by a light gray hue. A thick layer of petroleum jelly was applied to the entire face intraoperatively. The patient was instructed to reapply petroleum jelly frequently until complete reepithelialization.
Prophylactic antiviral therapy (for herpes simplex) was initiated the day before the procedure and continued for 10 days. The peak period of discomfort typically occurs 1 to 4 hours after the procedure and may last up to 8 hours.4 For relief, the use of cool, moist compresses and fans was recommended. Reepithelialization occurred approximately 1 week after the procedure.
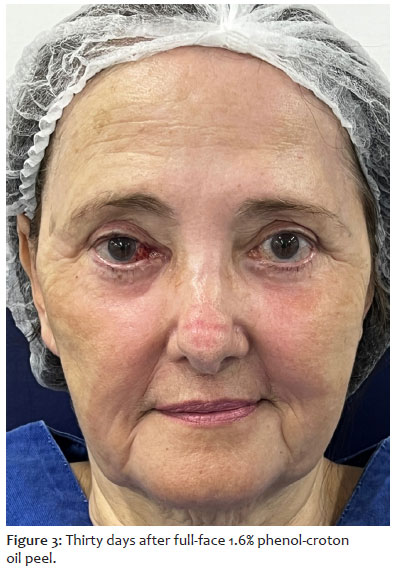
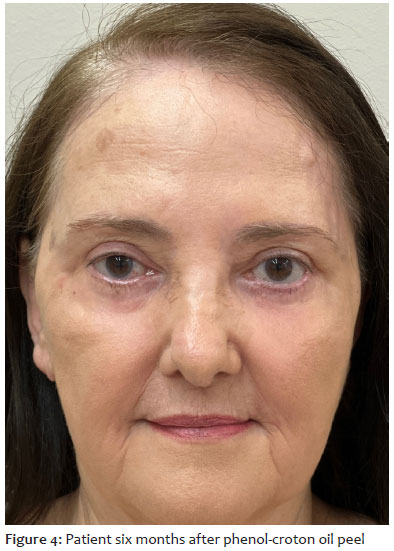
It is common for residual erythema to persist for 3 to 6 months following treatment, as shown in Figure 3.4 6 months after completing treatment, the patient exhibited a highly satisfactory outcome (Figure 4).
In patients with deep periocular and facial rhytides, isolated upper and lower blepharoplasty may not provide the desired level of facial rejuvenation. Therefore, combining eyelid surgery with other aesthetic procedures is often necessary to enhance overall outcomes. Full-face phenol-croton oil peel is an excellent adjunctive treatment option; however, it should be reserved for patients with lower Fitzpatrick phototypes (I, II, or III) and fixed deep rhytides that no longer respond to conventional therapies such as botulinum toxin injections.
Importantly, phenol is cardiotoxic. It can prolong the QT interval (>450 ms or an increase of 20-30 ms from baseline) and may trigger minor arrhythmic events (e.g., isolated atrial extrasystoles) as well as more significant ventricular arrhythmias such as ventricular bigeminy and nonsustained ventricular tachycardia.7 The risk of cardiotoxicity increases when phenol is applied to an area greater than one cosmetic unit, or more than 0.5% of total body surface area. Although phenol-croton oil peel has been associated with transient intraoperative QT prolongation, no clinically significant arrhythmias were observed. Nevertheless, due to the potential interaction of phenol with various medications – including analgesics, antibiotics, diuretics, antifungals, antipsychotics, and antidepressants – further investigation is warranted to establish clear safety parameters.7 In such cases, it is recommended that the procedure be performed in an operating room under continuous electrocardiographic monitoring and with appropriate air ventilation or exhaust systems. Substantial intravenous hydration during the procedure is also advised.4
Full-face phenol-croton oil peel may be safely performed in conjunction with blepharoplasty as long as transcutaneous lower eyelid surgery is not performed. This precaution is due to the risk of postoperative eyelid retraction resulting from the combined effect of surgical skin excision and anterior lamella contraction induced by the peel. Thus, phenol-croton oil peeling is best combined with either isolated upper blepharoplasty or with lower blepharoplasty performed via a transconjunctival approach, where only the prolapsed fat pads are excised, and skin treatment is exclusively managed by the peel.
Additionally, for patients with prominent periocular rhytides who do not wish to undergo full-face peeling, a phenol-croton oil peel can be applied to the periocular region in a localized fashion. Because the area involved is smaller, this localized approach can be safely performed in an outpatient setting.
Full facial rejuvenation is an increasingly common demand in dermatology, plastic surgery, and oculoplastic practice. To achieve more effective outcomes, a combination of treatments is often required to address skin laxity, improve skin quality, and, in some cases, restore volume in areas affected by the aging process. Thus, the present case demonstrated the effectiveness of combining blepharoplasty with phenol-croton oil peel for achieving significant facial rejuvenation in the patient described.
Juliana Senna Figueiredo Barbi
ORCID: 0000-0001-6888-0495
Final approval of the manuscript, study conception and design, active participation in research supervision, critical revision of the manuscript.
Marina Vieira Rodrigues Queiroz
ORCID: 0000-0001-5544-458X
Final approval of the manuscript, study conception and design, manuscript drafting and writing, intellectual contribution to the diagnostic and/or therapeutic approach, critical literature review, critical revision of the manuscript.
Karoline Kalinca Rabelo Santana
ORCID: 0000-0002-6744-8112
Final approval of the manuscript, manuscript drafting and writing, data acquisition, analysis, and interpretation, critical literature review.
Gustavo Carneiro Nogueira
ORCID: 0000-0002-0602-3241
Final approval of the manuscript, data acquisition, analysis, and interpretation, intellectual contribution to the diagnostic and/or therapeutic approach.
1. Alghoul M. Blepharoplasty: anatomy, planning, techniques, and safety. Aesth Surg J. 2019;39(1):10–28.
2. Bhattacharjee K, Misra DK, Deori N. Updates on upper eyelid lepharoplasty. Indian J Ophthalmol. 2017;65(7):551–8.
3. Cortez EA, Fedok FG, Mangat DS. Chemical peels: panel discussion. Facial Plast Surg Clin North Am. 2014;22(1):1–23.
4. Wambier CG, Lee KC, Soon SL, Sterling JB, Rullan PP, Landau M, et al. Advanced chemical peels: phenol- croton oil peel. J Am Acad Dermatol. 2019;81(2): 327–36.
5. Cardoso F, Moura RD, Pilar E, Moura I, Miot HA, Costa A. Phenol-croton oil peel enhances type-1 and type-3 collagen amounts by stimulating SIRT-6 and SIRT-7. Int J Dermatol. 2022;61(2):e71– 4.
6. Ozturk CN, Huettner F, Ozturk C, Bartz-Kurycki MA, Zins JE. (2013). Outcomes assessment of combination face lift and perioral phenol-croton oil peel. Plast Reconstr Surg. 2013;132(5):743e–53e.
7. Wambier CG, Wambier SPF, Pilatti LEP, Grabicoski JA, Wambier LF, Schmidt A. Prolongation of rate-corrected QT interval during phenol-croton oil peels. J Am Acad Dermatol. 2018;78(4):810-2.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}