


Micaelly Samara Meneses Santos; José Roberto Pegas; Raissa Piagentini de Andrade; Leonardo Silva Grassi; Vanessa Cristina Coimbra; Bianca Sousa de Almeida Neves
Funding support: None.
Conflicts of interest: None.
Submitted on: 24/06/2024
Approved on: 15/08/2024
How to cite this article: Santos MSM, Pegas JR, Andrade RP, Grassi LS, Coimbra VC, Neves BSA. Case report: the importance of nail transillumination in the diagnosis and topographic assessment of subungual glomus tumor. Surg Cosmet Dermatol. 2025;17:e20250382.
Glomus tumor is a rare, benign neoplasm typically found in areas with a high concentration of glomus bodies. It presents with a characteristic clinical triad: paroxysmal pain, cold sensitivity, and localized tenderness. We report the case of a patient with clinical suspicion of a glomus tumor, in which transillumination played a crucial role in diagnosis, surgical planning, and rapid pain relief. This case highlights the importance of maintaining a high index of clinical suspicion and the utility of transillumination for both diagnosis and therapeutic planning – particularly in settings where high-frequency ultrasound or magnetic resonance imaging is not readily available.
Keywords: Glomus Tumor; Transillumination; Nail Diseases; Surgical Procedures, Operative.
Glomus tumor was first described by William Wood in 1812. It is a rare, benign, slow-growing tumor derived from structures known as glomus bodies. These are neuromyoarterial structures composed of arteriovenous anastomoses responsible for thermoregulation by controlling blood flow to the skin. They are found in the dermis throughout the body, but are most concentrated in the digital pulp, particularly in the subungual nail beds.1,5
Glomus tumors are considered tumors of young individuals, with a higher prevalence among females and an average age at diagnosis of around 40 years. Studies show that the time from symptom onset to diagnosis typically ranges from 3.3 to 5 years. Clinically, these tumors are characterized by hyperesthesia and well-localized pain, which intensifies with exposure to cold temperatures. The classic triad suggestive of diagnosis includes paroxysmal lancinating pain, cold sensitivity, and precise localization of tenderness on palpation. Nail dystrophy and/or mild discoloration of the nail plate (bluish or pinkish hue) may also be observed.2,3
Definitive diagnosis is made through histopathological examination. Auxiliary methods for preoperative identification include transillumination, onychoscopy, high-frequency ultrasound, and magnetic resonance imaging (the gold standard).3,4
This study aims to report the case of a young patient with clinical suspicion of a glomus tumor, in which transillumination — a method considered highly specific — was instrumental for diagnostic support, prompt tumor excision, and effective pain control.
Information was obtained through medical record review and photographic documentation, with the patient's consent.
A 22-year-old male patient reported pain in the left fifth digit for 6 years, with progressive worsening. Initially, the pain occurred only during movement but later evolved to occur even at rest. On physical examination, he presented with intense pain upon palpation of the nail plate of the left fifth digit, which prevented precise tumor localization during the preoperative assessment.
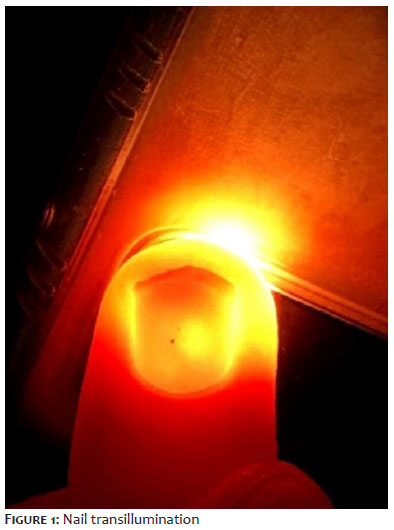
In the operating room, transillumination using a mobile phone flashlight revealed a translucent, spherical structure measuring approximately 4 mm in diameter (Figure 1). Based on clinical history and physical examination, a glomus tumor was suspected. Nail transillumination proved essential for preoperative localization, eliminating the need for additional imaging tests.
The patient underwent surgical exploration of the area guided by the light-assisted technique. A pinkish, rounded lesion with a smooth and regular surface — consistent with a glomus tumor — was identified (Figures 2 and 3). The lesion was excised, and the specimen was sent for histopathological analysis to confirm the diagnosis.
Glomus tumor is an uncommon neoplasm with benign behavior. It is a neurovascular mass derived from glomus bodies located in the reticular dermis. These bodies are arteriovenous anastomoses found throughout the body and are involved in thermoregulation.8 Although they may also be found in the central nervous system, gastrointestinal tract, and genital organs, glomus bodies are most commonly located in the digital pulp — especially within the subungual nail beds of the hands. Approximately 65% of glomus tumors are found in this region.2
The typical presentation is a solitary lesion in the subungual or periungual region. Clinically, it is defined by the classic triad of paroxysmal lancinating pain, localized tenderness, and hypersensitivity to cold. Except for subtle changes in nail color, the lesion usually has a normal macroscopic appearance. The pathophysiological mechanism of pain is not yet fully understood; however, it may involve myofilament contraction in response to temperature changes as well as the involvement of nerve fibers, mast cells, and cyclooxygenase-2. Indeed, the tumor's pathogenesis remains poorly understood.9,10
Diagnosis is essentially clinical and may be supported by complementary tests such as X-ray, magnetic resonance imaging (MRI), arteriography, ultrasound, and transillumination. The clinical signs and symptoms are typically sufficient to raise suspicion and justify surgical intervention.11 In a case series (2007–2009) involving 21 patients who underwent surgical excision, a variety of tests were used, including the “pin test” (pain upon percussion of the tumor area), thermal sensitivity test, and nail transillumination. In the latter, 85.7% of cases presented a bluish-violet or pink nodule in the subungual bed.2
The transillumination technique involves the use of a bright light source placed beneath the nail in a completely dark room. The tumor area appears as a distinct image, helping to estimate its size.4,8 In the present case, this method enabled visualization of a well-defined, rounded, lighter-colored image compared to the surrounding nail bed, indicating the probable tumor location without the need for further imaging. Intraoperatively, the lesion was found precisely in the area identified through transillumination, demonstrating the practicality, low cost, and effectiveness of this method.
Despite its advantages, transillumination is less effective in detecting multiple overlapping lesions and cannot differentiate the etiology of lesions, unlike imaging techniques such as ultrasound or MRI.15,16 There are reports of patients undergoing surgery only after MRI evaluation, and in one-third of these cases, the imaging failed to identify the tumor, resulting in false-negative outcomes. This reinforces the importance of clinical evaluation over reliance on imaging in cases of suspected glomus tumor.12
Differential diagnoses include hemangiopericytoma, neuroma, schwannoma, gout, osteoarthritis, subungual melanoma, and chronic paronychia. The treatment is primarily surgical. Two main techniques are described in literature: transungual and periungual approaches. Both are performed under local and regional anesthesia. The periungual approach, used in this case, is indicated for lesions located in the nail pulp or superficially in the subungual bed.
Possible surgical complications include nail deformity and tumor recurrence.14 In this case, the procedure was preceded by digital block anesthesia with 2% lidocaine at the base of the finger, along with distal wing block. A subtotal nail detachment was performed, preserving adherence on the contralateral nail fold. After trimming the nail at the level of the distal matrix (lunula), the nail bed became visible. A semilunar incision was made at the hyponychium, followed by dissection of the bed toward the lunula, where a single, well-circumscribed, rounded lesion was identified. It was carefully separated from the surrounding tissue.
Simple sutures were used to close the nail bed and to reposition and secure the detached nail fragment (Figure 4). The excised lesion was sent for histopathological examination, which later confirmed the diagnosis of glomus tumor.
Glomus tumor is a rare, benign neoplasm typically found in areas with a high concentration of glomus bodies, such as the subungual region and digital pulp. It presents with the classic clinical triad of paroxysmal pain, cold sensitivity, and localized tenderness. Nail dystrophy and/or slight discoloration (ranging from pink to violet) may also be observed.
Diagnosis is based on clinical suspicion and must be confirmed by histopathological examination. This tumor type often causes significant discomfort, requiring prompt management. As demonstrated in our case, the transillumination test — a practical, quick, and low-cost tool — can be highly valuable for supporting diagnosis and guiding early therapeutic planning in patients with clinical suspicion. It is especially useful in settings where advanced imaging techniques such as high-frequency ultrasound or magnetic resonance imaging (the gold standard) are not readily available.
Micaelly Samara Meneses Santos
ORCID: 0009-0001-0314-9033
Final approval of the manuscript; study conception and design; manuscript drafting and writing; data collection, analysis, and interpretation; intellectual contribution to diagnostic and/or therapeutic management of the case; critical review of the literature; critical review of the manuscript.
José Roberto Pegas
ORCID: 0000-0002-2541-6008
Final approval of the manuscript; study conception and design; manuscript drafting and writing; data collection, analysis, and interpretation; active research supervision; intellectual contribution to diagnostic and/or therapeutic management of the case; critical review of the literature; critical review of the manuscript.
Raissa Piagentini de Andrade
ORCID: 0009-0003-9250-9065
Final approval of the manuscript; study conception and design; manuscript drafting and writing; data collection, analysis, and interpretation; intellectual contribution to diagnostic and/or therapeutic management of the case; critical review of the literature; critical review of the manuscript.
Leonardo Silva Grassi
ORCID: 0000-0003-1629-9476
Final approval of the manuscript; study conception and design; manuscript drafting and writing; data collection, analysis, and interpretation; intellectual contribution to diagnostic and/or therapeutic management of the case; critical review of the literature; critical review of the manuscript.
Vanessa Cristina Coimbra
ORCID: 0009-0009-2583-0178
Final approval of the manuscript; study conception and design; manuscript drafting and writing; data collection, analysis, and interpretation; intellectual contribution to diagnostic and/or therapeutic management of the case; critical review of the literature; critical review of the manuscript.
Bianca Sousa de Almeida Neves
ORCID: 0000-0002-2921-6281
Final approval of the manuscript; study conception and design; manuscript drafting and writing; data collection, analysis, and interpretation; intellectual contribution to diagnostic and/or therapeutic management of the case; critical review of the literature; critical review of the manuscript.
1. Kim SW, Jung SN. Glomus tumour within digital nerve: a case report. J Plas Reconstr Aesthet Surg. 2011; 64(7):958-60.
2. Puentes Buendia GP, Jimenez Uribe WA, Facciolli D, Rodriguez Florez JM, Gervais J. Tumor glômico: um diagnóstico fácil ou difícil? Rev Bras Cir Plast. 2010;25(3):439- 42.
3. Grover C, Jayasree P, Kaliyadan F. Clinical and onychoscopic characteristics of subungual glomus tumor: a cross‐sectional study. Int J Dermatol.2021;60(6):693-702.
4. Tang CY, Tipoe T, Fung B. Where is the lesion? Glomus Tumours of the hand. Arch Plast Surg. 2013;40(5):492-5.
5. McDermott E, Weiss A. Review Glomus Tumors. J Hand Surg. 2006;31(8):1397-1400.
6. Lin YC, Hsiao PF, WuYH, Sun FJ, Scher RK. Recurrent digital glomus tumor: analysis of 75 cases. Dermatol Surg. 2010;36(9):1396-1400.
7. Lin S, Dumanian G. Benign hand tumors. Medscape; 2011.
8. Honsawek S, Kitidumrongsook P, Luangjarmekorn P, Pataradool K, Thanakit V, Patradul A. Glomus tumors of the fingers: expression of vascular endothelial growth factor. World J Orthop. 2016;7(12):843–6.
9. Samaniego E, Crespo A, Sanz A. Key diagnostic features and treatment of subungual glomus tumor. Actas Dermosifiliogr. 2009;100(10):875-82.
10. Sun Y, Ruiqun QI, Wu Z, Zhang X, Niu J. The clinicopathologic and immunohistochemical features of 60 cutaneous glomus tumor: a retrospective case series study. An Bras Dermatol. 2024;99(2):238-24.
11. Cigna E, Carlesimo B, Bistoni G, Conte F, Palumbo F, Scuderi N. The value of clinical diagnosis of digital glomus tumors. Acta Chir Plast. 2008;50(2):55-8.
12. Trehan SK, Athanasian EA, DiCarlo EF, Mintz DN, Daluiski A. Characteristics of Glomus Tumors in the hand not diagnosed on magnetic resonance imaging. J Hand Surg. 2015;40(3):542-5.
13. Suhett RP, Gervais Filho J, Souza MMC, Buttner AA, Janin B, Santos EA. Tumor Glômico: o que é e como tratar? Rev Bras Cir Plast. 2012;27(3 SUPPL.1):96.
14. Abidin MA, Kitta MI, Nong I, Rahmansyah N, Johan MP. Diagnosis and surgical approach in treating glomus tumor distal phalanx left middle finger: a case report. Int J Surg Case Reports. 2023:108:108426.
15. Quinto-González KL, Espinosa-Gutiérrez A, Hernández-Méndez-Villamil E, Borjón-Cisneros AE. [Glomus Tumor of subungual presentation in the thumb and use of ultrasound in its diagnosis. Case report and literature review]. Acta Ortop Mex. 2023;37(6):368-71. Spanish.
16. Tsiogka A, Belyayeva, Sianos S, Rigopoulos D. Transillumination: a diagnostic tool to assess Subungual Glomus Tumors. Skin Appen Dis.2021;7(3):231-3.
17. Chen L, Gao YH, Chen J, Yao YJ, Wang R, Yu Q, et al. Diagnosis of Subungual Glomus Tumors with 18MHz ultrasound and CDFI. Sci Rep. 2020;10(1):17848.
18. Saaiq M. Presentation and management outcome of Glomus Tumors of the hand. Arch Bone Joint Surg. 2021;9(3): 312.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}