


Rafael Rezende Rocha de Oliveira; Jade Noleto Viana; Kaique Arriel; Rafael Rubinho; Fernanda Rytenband
Financial support: None.
Conflicts of interest: None.
Submitted on: 15/03/2024
Approved on: 05/04/2024
How to cite this article: Oliveira RRR, Viana JN, Arriel K, Rubinho R, Rytenband F. Combined surgical techniques in the treatment of hypopigmented scars in discoid lupus erythematosus. Surg Cosmet Dermatol. 2025;17e20250359.
Discoid lupus erythematosus (DLE) causes chronic lesions that can heal with dyschromic patches. We report a clinical case showing success in the treatment of achromic lesions using a combination of surgical techniques, including excision, punch grafting, and full-thickness skin grafting.
Keywords: Lupus Erythematosus, Discoid; Cicatrix; Surgical Procedures, Operative.
Chronic cutaneous lupus erythematosus (CLE) is an autoimmune connective-tissue disease that predominantly affects women in the fourth decade of life. The most common clinical variant of chronic CLE is discoid lupus erythematosus (DLE), characterized by erythematous plaques covered with adherent scaling. Cutaneous lesions in DLE are chronic, persistent, and may regress, leaving hypopigmentation, scarring, telangiectasia, and cicatricial alopecia. These lesions, due to their unsightly nature, can be stigmatizing, causing a negative impact on quality of life.1
Here, we report a successful case in the treatment of achromic lesions in DLE using a combination of surgical techniques, including excision, punch grafting, and full-thickness skin grafting in a patient with multiple comorbidities.
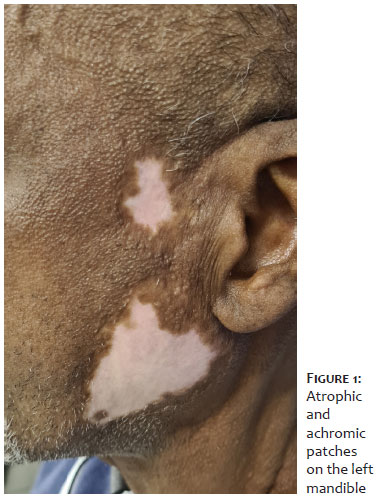
A 58-year-old male patient with hypertension and chronic kidney disease on dialysis, diagnosed with DLE 13 years ago, with stable disease for 9 years, and on hydroxychloroquine presented with significant aesthetic discomfort due to lesions on the face and scalp. On dermatological examination, he exhibited achromic and atrophic lesions on the left mandibular and preauricular regions (Figure 1), as well as in the occipital, temporal, and parietal scalp.
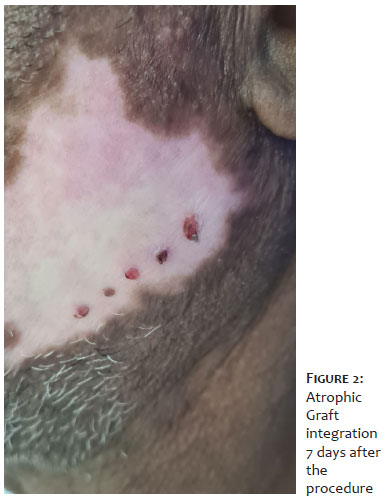
Due to the patient's comorbidities and high surgical risk, we initially decided to perform punch grafting in the achromic plaque of the left mandible. The left retroauricular region was chosen as the donor site. Local anesthesia was administered, and the grafts were harvested with a 3-mm punch. Five fragments were removed and placed on sterile gauze moistened with saline solution. The donor area was not sutured, and only compressive dressing was applied. The recipient area was incised at 5 linear points, spaced 1 cm apart, using a 2-mm punch. The grafts were placed on the recipient area and covered with sterile surgical tape, which was removed after 7 days (Figure 2).
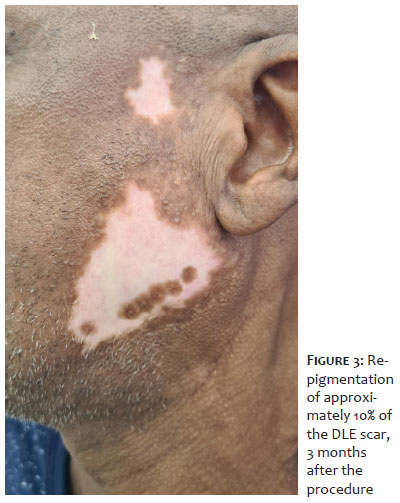
The patient returned 1 month after the procedure, showing small halos of repigmentation around the implants. After 3 months, he exhibited pigmented halos of approximately 1 cm around all the implanted grafts, with repigmentation of about 10% of the DLE lesion (Figure 3), without complications and satisfied with the treatment.
Additional punch grafting procedures were performed, and 1 year after the start of treatment, the patient demonstrated complete repigmentation of the patches, with multiple halos forming a homogeneous repigmentation macule. During this period, the preauricular lesion was excised with an elliptical incision of approximately 3 cm in height by 1 cm in width, followed by primary closure. After 9 months, the initial lesions had improved by approximately 90%.
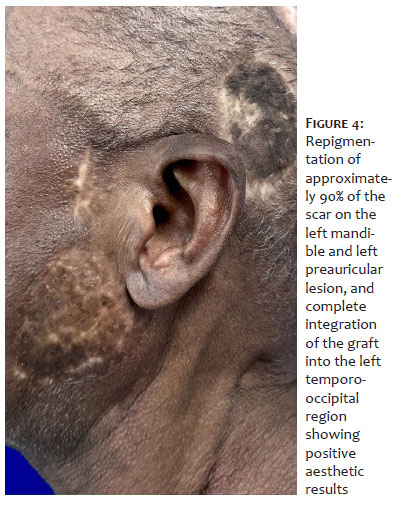
Considering the successfulness of the treatment, we decided to perform full-thickness skin grafting on the left temporo-occipital cicatricial lesion. The medial right thigh was chosen as the donor site. In the recipient area, the entire hypochromic cicatricial lesion was excised using an elliptical incision with a cold blade, and the cutaneous fragment was discarded. The healthy fragment was then placed on the recipient area, sutured, and covered with sterile dressing. The patient returned after 8 weeks with complete graft integration into the recipient site, promoting repigmentation of the region (Figure 4).
Punch grafting with melanocyte transplantation aims to provide a reservoir of melanocytes and repigment refractory lesions. However, in a meta-analysis evaluating treatment response of different surgical techniques, the highest repigmentation rate was achieved with skin grafting. Both techniques are simple to execute and low-cost; however, studies reporting the application of punch grafting in DLE lesions are scarce.2 Surgical excision of lesioned skin patches is a treatment option for certain dermatological conditions. Some cases of cicatricial alopecia may be corrected by surgical excision of small lesions followed by primary closure. For larger defects, tissue expanders or extensors may be used to allow for tension-free closure. Their use for burns and for cutaneous lupus itself has also been reported.2,3
In this case, the technique of punch grafting for melanocyte transplantation in the left mandibular region, full-thickness skin grafting in the left temporal region, and excision with primary closure in the left preauricular region was reported in the treatment of an adult patient with an achromic cicatricial lesions on the face due to DLE. Moreover, because the lesions were on the face, the patient already experienced considerable aesthetic discomfort, which impacted his quality of life.4 Possible adverse effects of this technique include static graft (without spread of pigmentation), cobblestone appearance, post-inflammatory hyperpigmentation, graft failure, and scar formation.5 Our patient did not experience any adverse effects.
In conclusion, punch grafting and full-thickness skin grafting may be promising options for the treatment of stable DLE lesions, which significantly impact quality of life. Further research is necessary to evaluate outcomes in a larger number of patients, considering that there are only a few reports in the literature.
Rafael Rezende Rocha de Oliveira
ORCID: 0000-0002-4261-185x
Preparation and writing of the manuscript; critical review of the literature; critical review of the manuscript.
Jade Noleto Viana
ORCID: 0009-0009-3089-9743
Preparation and writing of the manuscript.
Kaique Arriel
ORCID: 0000-0002-3984-2964
Study design and planning; preparation and writing of the manuscript; critical review of the literature.
Rafael Rubinho
ORCID: 0000-0002-4913-2560
Preparation and writing of the manuscript; critical review of the literature.
Fernanda Rytenband
ORCID: 0000-0002-2882-1658
Approval of the final version of the manuscript; preparation and writing of the manuscript; effective participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied case; critical review of the literature; critical review of the manuscript.
1. McDaniel B, Sukumaran S, Koritala T, Tanner LS. Discoid lupus erythematosus. Treasure Island (FL): StatPearls Publishing; 2024 .
2. Ju HJ, Bae JM, Lee RW, Kim SH, Parsad D, Pourang A, et al. Surgical interventions for patients with vitiligo: a systematic review and meta-analysis. JAMA Dermatol. 2021;157(3):307-316.
3. Unger W, Unger R, Wesley C. The surgical treatment of cicatricial alopecia. Dermatol Ther. 2008;21(4):295-311.
4. Lewandowicz E, Zielinski T, Iljin A, Fijalkowska M, Trojan-Kasielska A, Antoszewski B. Surgical treatment of skin lesions in lupus erythematosus. Postepy Dermatol Alergol.2014;31(6):405-409.
5. Romagnolli LE, Reis LM, Douat FB, Delfes MFZ, Battaglin ER, Torre DS. Tratamento de lesões cicatriciais acrômicas de lúpus discoide com técnica de enxertia por punch: relato de caso. Surg Cosmet Dermatol.2014;6(2):191-193.
6. Dellatorre G, Cafrune FE. Tratamento cirúrgico do vitiligo. Surg Cosmet Dermatol.2016;8(4):289-293.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}