


Vitoria Azulay; Beatriz Rocha Strauss; Gabriela Della Ripa; Lucas Madureira; Leonardo Rotolo
Financing: None.
Conflicts of interest: None.
Submitted on: 02/23/2023
Final decision: 05/22/2024
How to cite this article: Azulay V, Strauss BR, Ripa GD, Madureira L, Rotolo L. Forehead reduction: option for reconstructing forehead defects. Surg Cosmet Dermatol. 2025;17:e2025170351.
Three-dimensional facial analysis is the basis for planning appropriate treatment. We evaluated the face in thirds. The distance from the hairline to the glabella, from the glabella to the subnasale and from the subnasale to the menton must be equal. Some conditions such as androgenetic alopecia can cause a greater distance from the hairline to the glabella. We report the case of a 48-year-old patient with androgenetic alopecia and basal cell carcinoma in the right hairline in which forehead reduction surgery was performed in association with tumor excision, simultaneously providing esthetic improvement and resolving the oncological issue.
Keywords: Carcinoma, Basal Cell; Esthetics; Surgical Oncology.
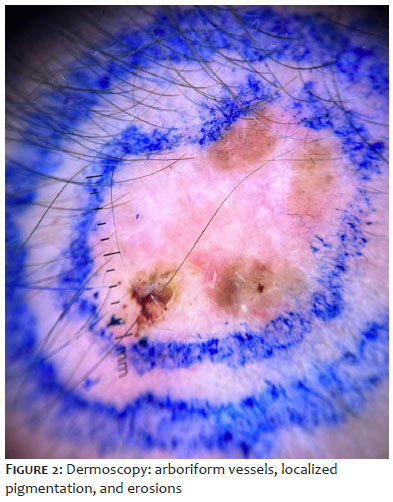
Cosmetic facial surgery is increasingly common in dermatological practice.1 New techniques are being developed to improve facial harmony and, when associated with oncological treatment, they provide a double benefit: esthetic and curative. We report the case of a 48-year-old female patient who sought our service due to the appearance of a plaque with pearly edges, with a slightly erythematous and atrophic center (Figure 1). On dermoscopic examination, an arboriform vascular pattern, localized pigmentation, and erosions were observed (Figure 2), resulting in diagnosis of basal cell carcinoma. Cryosurgical tumor excision was indicated. Considering that the patient had androgenetic alopecia, resulting in a receding hairline and an elongated forehead, it was decided to excise the tumor in association with forehead reduction through a pre-capillary incision (Figure 3).2 In addition, eyebrow ptosis and established rhytides on the forehead were observed, signs of aging that can be improved through forehead reduction.
This study is a case report performed at the Professor Rubem David Azulay Institute of Dermatology, Rio de Janeiro, Brazil. The patient provided written consent to use the images. Cryosurgery was performed to excise the basal cell carcinoma, in association with forehead reduction in a patient with androgenetic alopecia. The surgical technique consisted of marking the hairline with broken lines, anesthesia, incision at the hairline, removing a strip of skin and subcutaneous tissue, skin detachment, and wound closure in layers.
Cryosurgical excision of the tumor and forehead reduction were performed, reducing the forehead size by approximately 3 cm, simultaneously providing esthetic improvement and resolving the oncological issue.
Androgenetic alopecia can significantly affect a patient's psychosocial life, with varying degrees of impairment in overall quality of life.1 This disease has two peaks of incidence: one between the second and third decades of life and another between the fifth and sixth decades.1 As the name suggests, its pathophysiology is related to the interaction between hormonal and genetic factors.1 From a hormonal point of view, it is postulated that androgens promote, in genetically determined follicles, the transformation of terminal follicles into miniaturized follicles.1 The clinical manifestation is hair thinning in the scalp region, diffusely in women and, in men, in the frontoparietal, bitemporal and vertex areas. In advanced cases of androgenetic alopecia, the distance from the hairline to the glabella increases, causing disharmony and aging of the face. Techniques to alleviate this clinical situation range from the use of makeup or tattoos to forehead reduction surgery, which is considered a safe and effective method.3 Indications for this procedure include ptosis of the eyebrows or periorbital tissue, established rhytides on the forehead, and a disproportionately enlarged glabella or forehead. Impulsive decision-making and uncertainty about the procedure are considered contraindications, as is a risk of lagophthalmos, especially if the patient has previously undergone upper blepharoplasty with large tissue removal.4
The surgery consisted of:
Marking: While in the supine position, the patient was instructed to raise her eyebrows to determine the location of the frontalis muscle insertion. The frontalis muscle insertion line and the hair implantation line were marked using zigzag lines. The basal cell carcinoma was also marked according to dermoscopy, with a safety margin of 5 mm.
Anesthesia: Subcutaneous and subgaleal administration of local anesthesia (a solution of lidocaine, adrenaline, and saline solution) was performed.
Incision and removal of skin/subcutaneous tissue: Initially, the neoplasm was excised, with the free margin confirmed by intraoperative freezing. Subsequently, a trichophytic incision was made according to the forehead reduction markings (blade inclined at 20 degrees to preserve the hair follicles) and a 3 cm strip of skin/subcutaneous tissue was removed (Figure 4).
Detachment: Dissection was performed in the subgaleal plane with blunt scissors, and hemostasis was confirmed.
Suture: The surgical wound was sutured in layers, with 4-0 Vicryl internal sutures and 5-0 nylon external sutures (Figure 5).
Forehead reduction with a pre-capillary incision reduces the size of the forehead and raises the eyebrows, improving facial proportions. The procedure has a low complication rate.4 It is highly recommended for patients with an increased distance between the hairline and the glabella, such those with advanced androgenetic alopecia, in addition to eyebrow ptosis. The possibility of associating esthetic surgical techniques with curative surgery, such as basal cell carcinoma excision, increases patient satisfaction rates (Figure 6). The success achieved with this approach allows us to confidently recommend it to selected patients.
Vitoria Azulay
ORCID: 0000-0001-6534-1832
Conceptualization; writing and original draft; writing and review & editing.
Beatriz Rocha Strauss
ORCID: 0009-0004-5072-5242
Conceptualization; writing and original draft; writing and review & editing.
Gabriela Della Ripa
ORCID: 0000-0001-5236-2554
Intellectual participation in the propaedeutic and/or therapeutic conduct of the studied cases.
Lucas Madureira
ORCID: 0000-0001-9412-1900
Intellectual participation in the propaedeutic and/or therapeutic conduct of the studied cases.
Leonardo Rotolo
ORCID: 0000-0003-0481-8224
Writing and review & editing.
1. Azulay RD, Azulay DR, Azulay LA. Dermatologia. 8th ed. Rio de Janeiro: Guanabara Koogan; 2022.
2. Berenguer B, García T, Lorca-García C, San-Basilio M. Aesthetic forehead reduction in female patients: surgical details and analysis of outcome. J Plast Reconstr Aesthet Surg. 2022;75(1):407-414.
3. Kabaker SS, Champagne JP. Hairline lowering. Facial Plast Surg Clin North Am. 2013;21(3):479-86.
4. Niamtu, Joe. Cosmetic facial surgery. 2nd ed. Elsevier; 2017.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}