


Mariele Bevilaqua1; Ana Claudia Dal-Magro1; Laura Luzzatto1; Renan Rangel Bonamigo1,2,3; Ana Paula Dornelles Manzoni1
Financial support: None.
Conflicts of interest: None.
Submitted on: 17/01/2024
Approved on: 05/04/2024
How to cite this article: Bevilaqua M, Dal-Magro AC, Luzzatto L, Bonamigo RR, Manzoni APD. The unpredictability of silicone fillers: "facies leonina-simile" reaction. Surg Cosmet Dermatol. 2024;16:e20240344.
A 76-year-old woman presented with facial edema and nodules in the front glabellar region and nasal dorsum that clinically resembled leonine facies. A facial ultrasound showed deposits of permanent facial filler with a "snowstorm" aspect characteristic of silicone oil, and an anatomopathological examination suggested a granulomatous reaction to the exogenous substance. Permanent fillers, such as silicone, behave like foreign bodies and cause a chronic granulomatous reaction. Although dermal fillers have been increasingly used, there is still no consensus on the management of their complications. In the present case, a good response to dapsone was observed.
Keywords: Silicones; Dermal Fillers; Granulomatous Disease, Chronic; Foreign-Body Reaction.
The ideal soft tissue filler is one that is effective, nonimmunogenic, nontoxic, noncancerous, nonmigratory, easy to apply, nonpalpable, and painless. Unfortunately, no such product yet exists, and we are increasingly seeing unforeseen manifestations for injectable products used as esthetic fillers. In the middle of the 20th century, a purified synthetic polymer in the form of injectable silicone began to be used for this purpose. Although it seemed promising, it was banned in the USA by the Food and Drug Administration (FDA) in 1991 due to complications.1 In Brazil, it was suspended in 2006, although new complications secondary to its use have been reported to this day.2
A 76-year-old woman presented with intense facial edema and indurated erythematous nodules located in the frontoglabellar region and dorsum of the nose, which clinically resembled a leonine face (Figure 1). The lesions began 12 months ago after a dental procedure and only improved during oral corticosteroid therapy, with recurrence when attempts to stop it were made. She reported only mild local discomfort and no systemic symptoms. In her previous medical history, she had undergone facial rhytidoplasty with placement of a silicone menton prosthesis approximately 40 years previously, facial filling with an unknown substance 30 years ago, and had controlled hypothyroidism, hypertension, and rhinitis.
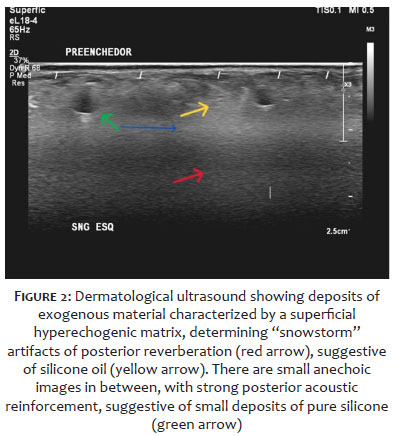
A facial ultrasound was requested and showed permanent facial filling deposits, characterized by areas of increased echogenicity in the dermis and subcutaneous tissue, determining "snowstorm" posterior reverberation artifacts, characteristic of silicone oil filling associated with oval anechoic images, with posterior acoustic reinforcement, superficial and smaller than 0.3cm, consistent with small deposits of pure silicone associated with silicone oil, located in the lower eyelids and infrapalpebral region, and a silicone implant in the chin, in a deep situation, with no signs of extravasation (Figure 2).
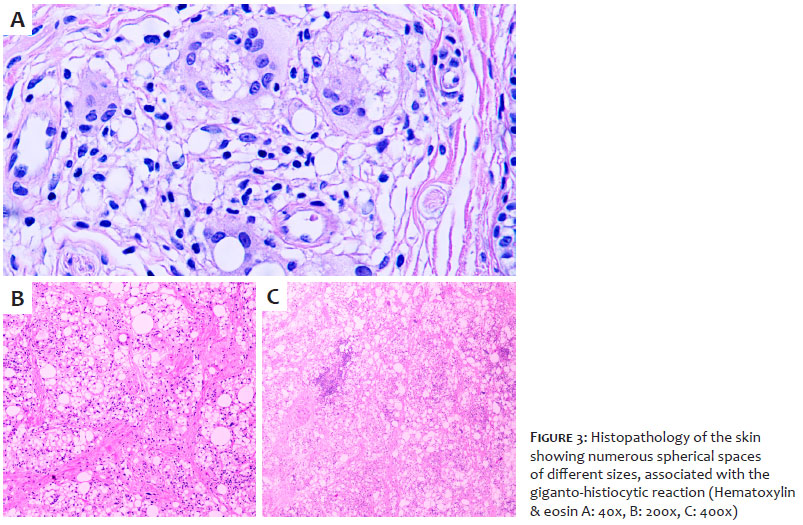
No areas of abscesses or liquid collections were evident. Histopathological examination of the skin identified numerous spherical spaces of different sizes, associated with a giganto-histiocytic reaction and negative tests for acid-fast bacilli (AFB) and fungi using the Ziehl-Neelsen, Grocott, and periodic acid-Schiff (PAS) stains. The morphological findings suggested a granulomatous reaction to the exogenous substance (Figures 3A, 3B, 3C).
Bacteriological, mycobacteriological, and mycological cultures were negative. General laboratory tests, including serology for viral infections such as SARS-CoV-2 and autoimmunity markers (antinuclear factor - ANF - and rheumatoid factor - RF), and glucose-6-phosphate dehydrogenase (G6PD) were unremarkable. The initial treatment recommended was prednisone 40mg (0.5mg/kg/day), moxifloxacin 400mg/day, and clarithromycin 500mg every 12 hours for 30 days (until the definitive results of the cultures) with total remission of the lesions. After 30 days, the corticosteroid therapy was gradually reduced and dapsone 50mg/day was introduced, with an increase in the second month to 75mg/day, with laboratory control (blood count, transaminases), reaching 100mg/day; however, with this dose, the patient showed a drop of one point in hemoglobin (g/dL), so the dose of 75mg/day was resumed to avoid recurrence of the lesions. The patient used dapsone for 10 months and, at the time of completing this report, there had been no worsening (Figure 4).
Injectable liquid silicone, or fluid polydimethylsiloxane, was a product used for tissue filling, considered unstable, with a high risk of migration and triggering local and systemic immune responses.2,3 Its most common late complication is the appearance of a single, nodular-granulomatous lesion, also known as "late siliconoma," and when the affected area is small, it can be treated with intralesional corticosteroids or antimitotic agents such as 5-fluorouracil; however, in extensive cases, the use of systemic corticosteroid therapy is necessary.4
In the present case, the exuberance of the manifestation is noteworthy, with the presence of around 20 nodules, widening of the nasal base, and an infiltrated appearance in the supraciliary region, which led to the analogy with the "leonine facies" (a condition that can be observed in lepromatous leprosy and cutaneous lymphomas, for example).5 It is also noteworthy that the first clinical manifestation occurred 30 years after the procedure, and the probable trigger was the dental procedure. Beleznay et al. described that 39% of patients with late complications after filling with hyaluronic acid have a respiratory tract infection or previous dental procedure as a trigger.6 Lloret et al. reported two cases of granulomatous reaction after silicone skin filling, in which the patients had positive antinuclear antibodies.7
In view of the constant recurrences of facial granulomas when systemic corticosteroid therapy was reduced, dapsone was added to the therapeutic regimen in this case. The choice of this antineutrophilic drug was based on its lower long-term morbidity and experience in treating other facial granulomatous diseases.7,8 There is still a need for scientifically relevant publications on the best treatment regimen for granulomas secondary to fillers and, for the time being, the options described range from surgical excision, intralesional corticosteroids, tetracyclines, tacrolimus, imiquimod, methotrexate, mycophenolate mofetil, alupurinol, cyclosporine, and azathioprine to etanercept.9-12 Some authors have had good experience with the use of isotretinoin, similar to how it is used in granulomatous rosacea.7 However, there is still no data defining whether any of these drugs are superior among the treatment options.
Complications from facial fillers are becoming increasingly common. Permanent fillers, which were widely used decades ago, are particularly challenging due to their unpredictability in terms of the onset time of their complications (from days to decades) and clinical variations. Scientifically relevant publications are needed to guide the best treatment regimen, as it is believed that the number of cases will increase exponentially given the wide range of aesthetic procedures available today.
Mariele Bevilaqua
ORCID:-0001-5689-1162
Approval of the final version of the manuscript; study design and planning; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of the cases studied; critical review of the manuscript.
Ana Claudia Dal-Magro
ORCID:-0001-5472-4539
Approval of the final version of the manuscript; data collection, analysis, and interpretation.
Laura Luzzatto
ORCID:-0002-4193-6943
Approval of the final version of the manuscript; data collection, analysis, and interpretation.
Renan Rangel Bonamigo
ORCID:-0003-4792-8466
Approval of the final version of the manuscript; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of the cases studied; critical literature review.
Ana Paula Dornelles Manzoni
ORCID:-0001-6184-4440
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; active participation in research orientation; critical review of the manuscript.
1. Attenello NH, Corey SM. Injectable fillers: review of material and properties. Facial Plast Surg. 2015;31(1):29-34.
2. Marinelli E, Vergallo GM, Reale G, Di Luca A, Catarinozzi I, Napoletano S, et al. The role of fillers in aesthetic medicine: medico-legal aspects. Eur Rev Med Pharmacol Sci. 2016;20(22):4628-4634.
3. Vargas AF, Amorim NG, Pintaguy I. Complicações tardias dos preenchimentos permanentes. Rev Bras Cir Plást. 2009;24(1):71-81.
4. Broder KW, Cohen SR. An overview of permanent and semipermanent fillers. Plast Reconstr Surg. 2006;118(3 Suppl):7S-14S.
5. Souza CS. Hanseniase: formas clínicas e diagnostico diferencial. Medicina (Ribeirão Preto). 1997;30:325-34.
6. Beleznay K, Carruthers JDA, Carruthers A, Mummert ME, Humphrey S. Delayed-onset nodules secondary to a smooth cohesive 20 mg/mL hyaluronic acid filler: cause and management. Dermatol Surg. 2015;41(8):929-39.
7. Lloret P, España A, Leache A, Bauzá A, Fernández-Galar M, Idoate MA, et al. Successful treatment of granulomatous reactions secondary to injection of esthetic implants. Dermatol Surg. 2005;31(4):486-90.
8. Cavallieri FA, Balassiano LKA, Bastos JT, Fontoura GHM, Almeida AT. Edema tardio intermitente e persistente ETIP: reação adversa tardia ao preenchedor de ácido hialurônico. Surg Cosmet Dermatol. 2017;9(3):218-222.
9. Lindhaus C, Elsner P. Granuloma faciale treatment: a systematic review. Acta Derm Venereol. 2018;98(1):14-18.
10. Alijotas-Reig J, Fernández-Figueras MT, Puig L. Inflammatory, immune-mediated adverse reactions related to soft tissue dermal fillers. Semin Arthritis Rheum. 2013;43(2):241-58.
11. Desai AM, Browning J, Rosen T. Etanercept therapy for silicone granuloma. J Drugs Dermatol. 2006;5(9):894-6.
12. Requena L, Requena C, Christensen L, Zimmermann US, Kutzner H, Cerroni L. Adverse reactions to injectable soft tissue fillers. J Am Acad Dermatol. 2011;64(1):1-34; quiz 35-6.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}