


Melissa de Almeida Corrêa Alfredo; Ingrid Rocha Meireles Holanda; Ivanka Miranda Castro; Gabriela Roncada Haddad
Financial support: None.
Conflicts of interest: None.
Submitted on: 09/05/2023
Approved on: 10/04/2023
How to cite this article: Alfredo MAC, Holanda IRM, Castro IM, Haddad GR. Piebaldism – portraits of hereditary character: a series of cases. Surg Cosmet Dermatol. 2023;15:e20230297.
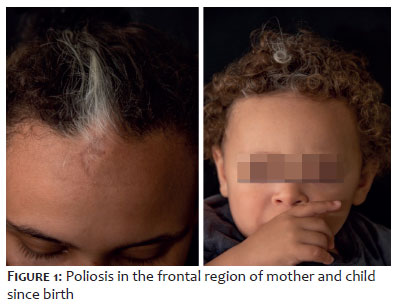
Piebaldism is a rare, autosomal dominant dyschromia characterized by circumscribed poliosis and triangular achromia in the frontal region in 90% of affected individuals, with no other systemic involvement. The incidence of dyschromia in this Dermatology Department, in a short space of time, and with plenty of images, motivated the presentation of this series of cases. We show two families with piebaldism, treated at the same Dermatology Department in 2021: the first family, with a mother and son presenting achromic macules on the trunk and poliosis in the frontal region since birth; the second family, with a grandmother, aunt, mother, and son showing the same characteristics described.
Keywords: Piebaldism; Pigmentation Disorders; Skin Diseases; Genetic
Piebaldism is a rare dyschromia characterized by circumscribed poliosis and triangular achromia in the frontal region in 90% of affected individuals. The incidence of dyschromia in the same Dermatology Department, within a short period of time and with plenty of images, motivated the presentation of this series of cases. We show two families with piebaldism, from different cities near the region, treated in the same department during 2021 (Figures 1 and 2).
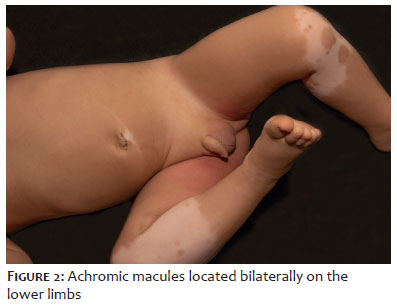
Case 1: One-year-old, male child. Referred from the BHU due to achromic macules on the body and poliosis in the frontal region since birth.
Mother with the same characteristics.
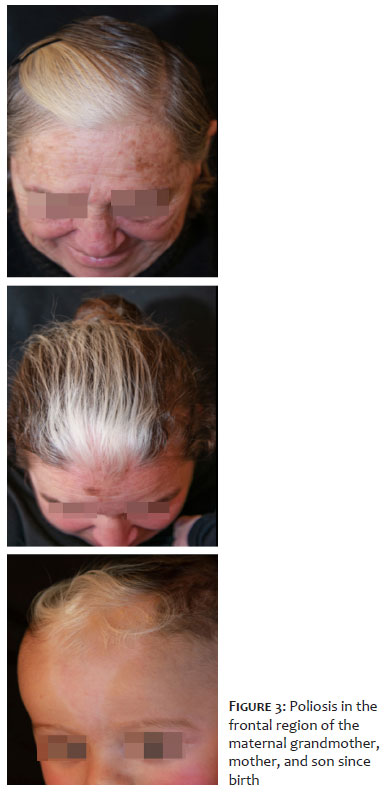
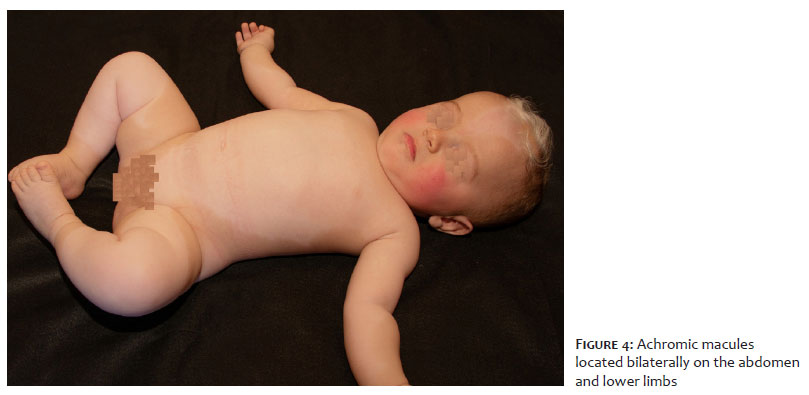
Case 2: Eight-month-old, male child. Referred from the Pediatrics Department due to achromic macules on the body and poliosis in the frontal region since birth (Figures 3 and 4).
Mother with the same characteristics. Maternal grandmother and aunt had the same phenotypic characteristics.
Piebaldism is a rare dermatosis that affects around 1:20.000 individuals, regardless of sex or ethnicity. In 90% of cases, poliosis and areas of achromic skin are present, unrelated to systemic alterations.1 This dyschromia has been described since Egyptian reports2 and occurs due to mutations in the C-KIT 4q12 proto-oncogene, an autosomal dominant disorder, with abnormal migration of melanoblasts in the neural crest, resulting in body areas without melanocytic activity.3
Poliosis is typical of the disease, characterized by an area with no pigment in the frontal region of the scalp, which extends in a triangular shape to the forehead, converging towards the midline of the face. Achromic and hypochromic macules that affect the body are characteristically of a central pattern, located predominantly on the abdomen, the middle third of the upper and lower limbs, sparing the involvement of the hands, feet, and back.1 The central pattern of dyschromia is explained because the mutation affects the neural crest. Affected individuals may present with hyperchromic macules and axillary ephelides.3
The diagnosis of piebaldism is clinical and, if it is suspected, a thorough clinical, ophthalmological, neurological, and gastrointestinal investigation is necessary, even in the neonatal period, to rule out differential diagnoses with possible systemic and deleterious symptoms, such as Waardenburg syndrome, which not only has achromic macules, but also iris heterochromia and sensorineural deafness.1,3 Other differential diagnoses are vitiligo, Ito hypomelanosis, Wolf syndrome, and achromic nevus.4
As this is a benign condition, no treatment is required, but photoprotection guidelines are essential. Melanocyte transplants have been reported to reduce areas of achromia in patients with aesthetic complaints.5
Isolated piebaldism has no known systemic complications. As an autosomal dominant genodermatosis, it is necessary to question the family pattern when the diagnosis is suspected.
Melissa de Almeida Corrêa Alfredo
ORCID: 0000-0001-7423-4190
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in the propaedeutic and/or therapeutic conduct of the studied cases; critical literature review; critical review of the manuscript.
Ingrid Rocha Meireles Holanda
ORCID: 0000-0002-2629-5244
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in the propaedeutic and/or therapeutic conduct of the studied cases; critical literature review; critical review of the manuscript.
Ivanka Miranda Castro
ORCID: 0000-0002-3146-1892
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in the propaedeutic and/or therapeutic conduct of the studied cases; critical literature review; critical review of the manuscript.
Gabriela Roncada Haddad
ORCID: 0000-0002-7516-9586
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis and interpretation; active participation in research orientation; intellectual participation in the propaedeutic and/or therapeutic conduct of the studied cases; critical literature review; critical review of the manuscript.
1. Shah M, Patton E, Zedek D. Piebaldism. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK544238/
2. Huang A, Glick SA. Piebaldism in History—"The Zebra People." JAMA Dermatology. 2016; 152(11):1261.
3. Saleem MD. Biology of human melanocyte development, piebaldism, and waardenburg syndrome. Pediatr Dermatol. 2019;36(1):72-84.
4. Grob A, Grekin S. Piebaldism in children. Cutis. 2016 ;97(2):90-2.
5. Neves DR, Régis Júnior JR, Oliveira PJ, Zac RI, Silveira Kde S. Melanocyte transplant in piebaldism: case report. An Bras Dermatol. 2010;85(3):384-388.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}