


Bruna Mendes Almeida; Ana Claudia Rolim Branco; Célia Antônia Xavier de Moraes Alves; Nayara Pelizaro Di-Rito; Gabriela Fagan Belini
Financial support: None.
Conflicts of interest: None.
Submitted on: 07/24/2023
Approved on: 08/16/20
How to cite this article: Almeida BM, Branco ACR, Alves CAXM et al. Treatment of a rare case of nodular cutaneous amyloidosis in the nose: a case report. Surg Cosmet Dermatol. 2023;15:0281.
Although primary cutaneous amyloidosis (PCA) is prevalent worldwide, it is underdiagnosed. Among the subtypes, nodular amyloidosis (NA) is the rarest. There is no consensus in the literature; treatment is challenging, and no therapy has been proven effective. The authors report the case of a patient with a nodule in the nose, whose anatomopathological examination was compatible with amyloidosis, with no evidence of systemic disease. It was then classified as nodular PCA. The lesion was excised satisfactorily. It was concluded that surgical removal is an effective therapy for the treatment of NA.
Keywords: Amyloidosis; Amyloid; Congo Red
Amyloidosis is a heterogeneous group of conditions characterized by extracellular deposition of amyloid material.1 In the primary cutaneous form, deposition is restricted to the skin, with no systemic repercussions.2 Nodular primary cutaneous amyloidosis (PCA) or nodular amyloidosis (NA) is the rarest form, with few cases reported in recent years; it has particular characteristics, as up to 7% of cases can progress to systemic amyloidosis.1 There is still no effective treatment for removing amyloid deposits, but there is a wide range of therapies to improve aesthetics. Not all treatments, however, are effective.1
A 32-year-old male patient referred to the Dermatology Department complaining of an eight-month-old single lesion on his nose, initially a papule, which grew slowly and progressively. He denied any local symptoms and reported only aesthetic discomfort.
He reported sporadic smoking and alcohol consumption, tension headaches, and was taking sertraline 50mg/day. No family history was reported.
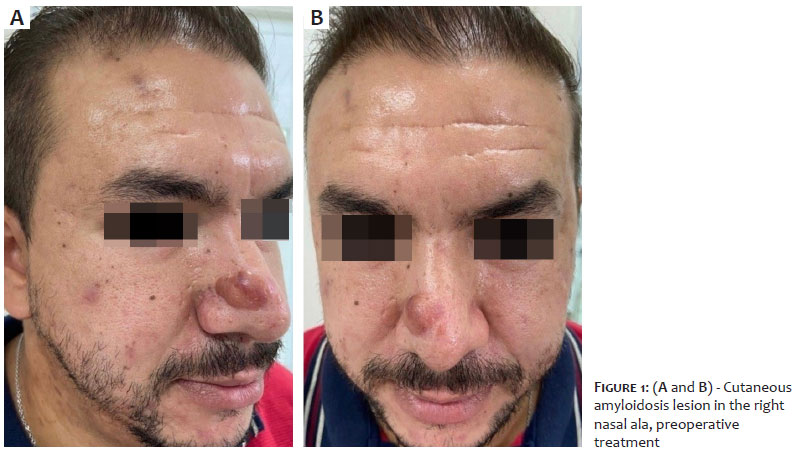
Dermatological examination revealed an erythematous nodule measuring approximately 3 × 2cm, with a fibroelastic consistency, in the transition between the dorsum of the nose and the right nasal wall (Figure 1).
Diagnostic hypotheses of cutaneous lymphocytoma, dermatofibrosarcoma protuberans, nodular cutaneous amyloidosis, and facial granuloma were initially considered. A biopsy of the lesion was requested for anatomopathological analysis.
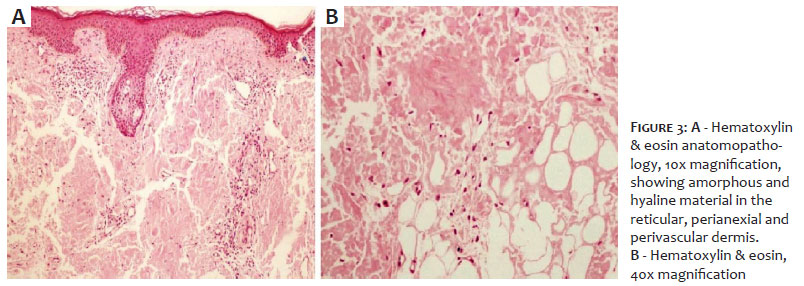
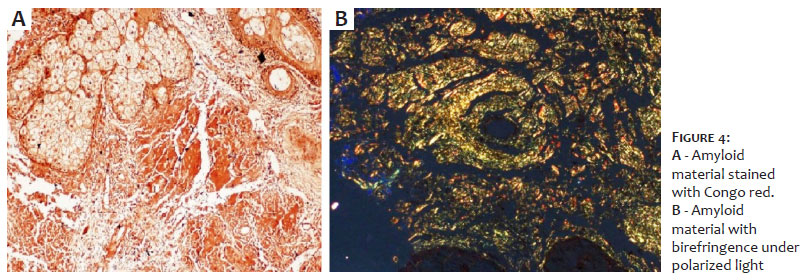
Histopathology revealed a deposit of amorphous and hyaline material in the reticular, perivascular, and perianexial dermis, which turned reddish when stained with Congo red and greenish under polarized light, thus characterizing amyloid material (Figures 2 and 3).
Screening for systemic disease with imaging tests (computed tomography of the skull, chest, and abdomen) and laboratory tests (blood count, complement system, serum, and urine protein electrophoresis) were performed, with no alterations, and the diagnosis of nodular PCA was confirmed.
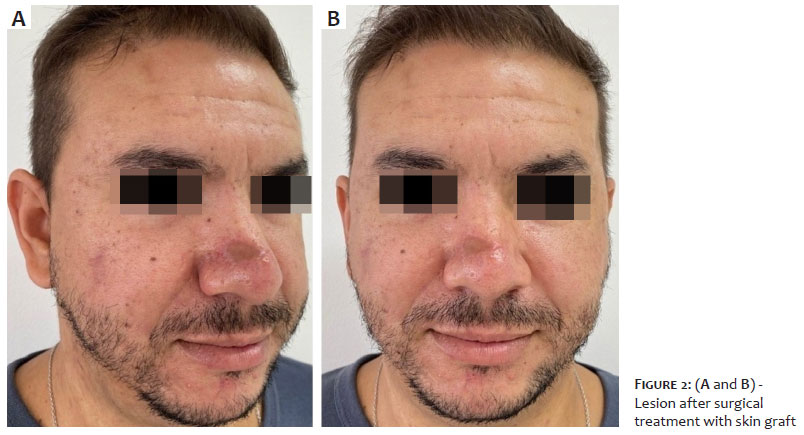
The patient's wishes were met with an explanation of the available and possible therapeutic options. We decided to perform surgical excision of the lesion, with subsequent skin grafting, using a graft from the suprascapular region. A satisfactory aesthetic result was achieved and the patient has had no signs of recurrence for a year (Figure 4).
Amyloidosis can be divided into primary and secondary, systemic or localized, based on historical classification.7 Although cutaneous amyloidosis is prevalent worldwide, it is still underdiagnosed. It is not associated with systemic diseases. It occurs due to abnormal extracellular protein deposition in the dermis by aggregation, polymerization, and formation of fibrils. These are deposited, becoming insoluble and resistant to proteolysis.5 The pathogenesis is still unknown, but it is attributed to the death of keratinocytes as a result of a preexisting dermatosis.5
PCA is subdivided into macular, lichen amyloid, nodular, and biphasic. The nodular form is the rarest and its pathology differs from the others in that the amyloid material stems from the deposition of light chain immunoglobulin produced locally by monoclonal plasma cells, and not from degenerated keratinocytes.4,5 These deposits are not restricted to the dermis, but also include vessels and appendages.8 Histopathology shows deposits of amorphous and eosinophilic material in the superficial dermis and around vessels and appendages, stained with Congo red. Under polarized light, these deposits show a birefringent green color.2
Clinically, NA presents as single or multiple nodules, predominantly on the face, extremities, and scalp.7 It grows insidiously and is sometimes asymptomatic, which can lead to late diagnosis or underdiagnosis. However, regular follow-up is extremely important given the 7% risk of progression to systemic amyloidosis.5,7,8 Furthermore, the possible association with systemic sclerosis and Sjogren's syndrome is well established in the literature.8
Various therapeutic options have been described in the literature, but none have proven to be effective in completely removing the amyloid material or preventing the progression of the deposits, which leads to a common local recurrence.1,9,3 Some therapies have been responsible for accelerating or deepening these deposits.3 Well-established options include the use of occlusive or intralesional topical corticosteroids, although some studies have associated these drugs with the acceleration of deposits, dermabrasion, surgical excision, and technologies such as the CO2 laser.3,7,9
This report aimed to portray a case of NA effectively treated with surgical excision, corroborating it as a good option for treatment, both in terms of aesthetic appearance and easy accessibility. However, more studies with robust evidence are needed to establish therapies and protocols.
Given that it can present as an insidious and asymptomatic lesion, the diagnosis of NA can be delayed or even missed, thus leading to underdiagnoses. However, due to the importance of its association with systemic diseases and the possibility of progression to systemic amyloidosis, NA should be part of the dermatologist's diagnostic scope for nodular lesions. Once the diagnosis has been established, the patient should be followed up regularly. Treatment will depend on the patient's complaint or request, always in agreement with their doctor about accessible and available therapies, considering possible recurrence.
Bruna Mendes Almeida
ORCID: 0000-0002-0804-5401
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical review of the manuscript.
Ana Claudia Rolim Branco
ORCID: 0009-0006-9564-1813
Author's contribution: Approval of the final version of the manuscript; preparation and writing of the manuscript; critical review of the manuscript.
Célia Antônia Xavier de Moraes Alves
ORCID: 0000-0002-8421-8837
Author's contribution: Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of the cases studied.
Nayara Pelizaro Di-Rito
ORCID: 0009-0002-1972-6453
Author's contribution: Approval of the final version of the manuscript; critical review of the manuscript.
Gabriela Fagan Belini
ORCID: 0000-0003-4492-2392
Author's contribution: Approval of the final version of the manuscript; critical review of the manuscript.
1. Schipper CR., Cornelissen AJM, Welters CFM, et al. Treatment of rare nodular amyloidosis on the nose: a case report. JPRAS Open. 2015;6:25–30.
2. Summers EM, Kendrick CG. Primary localized cutaneous nodular amyloidosis and CREST syndrome: a case report and review of literature. Cutis. 2008;82:55-59.
3. Raymond J, Choi J. Nodular cutaneous amyloidosis effectively treated with intralesional methotrexate. JAAD. 2016;2:373-376.
4. Alexanian C, Chen YC, Le S, et al. Nodular amyloidosis of the lips as a presenting feature of systemic amyloidosis associated with multiple myeloma. JAAD Case Reports. 2019;5(11):963–965.
5. Kalajian AH, Waldman M, Knable AL. Nodular primary localized cutaneous amyloidosis after trauma: a case report and discussion of the rate
6. of progression to systemic amyloidosis. JAAD. 2007;57(2):S26–S29.
7. Junior WB, Chiacchio ND, Criado PR. Tratado de dermatologia. 2nd ed. São Paulo: Atheneu; 2014.
8. Azulay RD. Dermatologia. 8th ed. Rio de Janeiro: Guanabara Koogan; 2022.
9. Verma SB, Khopkar U. Bilateral recurrent facial primary cutaneous nodular amyloidosis (PCNA). JAAD Case Reports. 2016;2(1):31–33.
10. Woollons A, Black MM. Nodular localized primary cutaneous amyloidosis: a long-term follow-up study. Br J Dermatol. 2001;145(1):105–109.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}