


Simone Ramos Neri1; Marcia Regina Franzolin2; Célia Luiza Petersen Vitello Kalil3; Vaniky Duarte Marques4; Ronaldo Maciel Marques2; Marta Oliveira Domingos2
Fonte de financiamento: None
Conflito de interesses: Nenhum.
Data de Submissão: 20/04/2023
Decisão final: 20/06/2023
How to cite this article: Neri SR, Franzolin MR, Kalil CLPV, Marques VD, Marques RM, Domingos MO. Therapeutic effect of botulinum toxin A on dissecting cellulitis of the scalp. Surg Cosmet Dermatol. 2024;16:e20240252.
A patient with folliculitis dissecans who did not respond to antibiotic therapy received four monthly sessions of intradermal administration of 100 IU of botulinum toxin A. Four months after the treatment, a complete recovery of the affected area of the patient's scalp was observed. A biopsy taken from the lesional area showed the presence of Staphylococcus lugdunensis and Staphylococcus aureus, both of which were found to be resistant to erythromycin. It was observed that the toxin had no effect on the viability or biofilm production of the Staphylococcus strains. This indicates that the healing effect of the toxin was associated with the host response alone.
Keywords: Botulinum Toxin A, Folliculitis Dissecans, Staphylococcus aureus, Staphylococcus lugdunensis
Folliculitis dissecans is a rare scarring alopecia characterized by neutrophilic inflammation, hair loss, perifollicular pustules, nodules, and abscesses.1 Despite the fact that the abscesses of folliculitis dissecans are sterile, they are frequently associated with secondary bacterial infection, mainly by Staphylococcus aureus.2 Accordingly, the conventional treatment for this disorder involves the use of topical and oral antibiotics, which may not be very effective in severe cases where surgical removal of the affected area needs to be considered.3 Therefore, there is an urgent need to find new treatments to control the development of this disorder. Taking into consideration that several studies have demonstrated that botulinum toxin A can be used as an alternative treatment for androgenetic alopecia, a non-scarring folliculitis disorder which is not associated with infection, the present work, investigates the healing effect of botulinum toxin A in folliculitis dissecans.4,5 The results obtained were very promising, suggesting that botulinum toxin A has the potential to be used as an alternative treatment for patients with folliculitis dissecans who do not respond to the conventional antibiotic treatments.
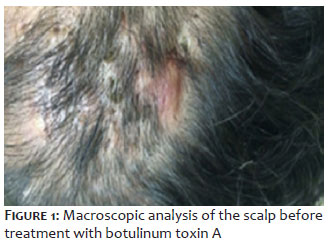
A 37-year-old male patient with clinical picture of folliculitis dissecans was admitted to our clinic. The patient did not have associated comorbidities such as high blood pressure, diabetes or obesity. Upon clinical examination the presence of nodules, abscesses and a patch of alopecia was observed. (Figure 1)
At admission, the patient was treated with tetracycline-type antibiotic (100mg/24 h for 12 weeks) and intralesional administration of corticosteroids and antibiotics. However, the patient did not respond to these treatments. Therefore, botulinum toxin A was considered as an alternative treatment option. The patient was then treated with intradermal administration of 100 IU of botulinum toxin A (Allergan) at days 0, 30, 60, and 90. A diagram of the scalp area to be treated was previously defined by outlining the infection sites. Each injection site received a dose of 2.5 IU/100 µL of botulinum toxin A in sterile saline 0.9%. The patient did not receive any other type of treatment during this period. After the treatment, the patient reported elimination of pain within the first two weeks of treatment. In addition, after a period of four months from the initial treatment, the abscesses and the bumps receded, and a significant increase in hair density was observed. (Figure 2)
In order to carry out a microbiological analysis of the affected area, a punch biopsy of approximately 3 mm in size, was taken from the patient's scalp lesional area before the treatment with botulinum toxin A. 6,7,8 The results showed the presence of Staphylococcus aureus and Stapylococcus lugdunensis, which were resistant to erythromycin, associated with the biopsy (Table 1)
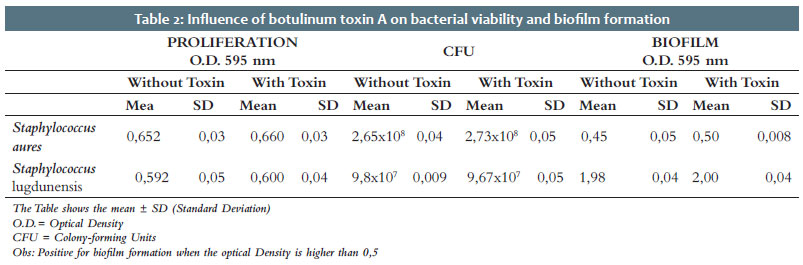
The influence of botulinum toxin A on the Staphylococcus strains derived from the patient was also investigated. For that, the effect of botulinum toxin A on the growth (bacteriostatic effect) and killing (bactericidal effect) of Staphylococcus aureus and Staphylococcus lugdunensis was determined by measuring the optical density of the bacterial culture and counting the number of colony-forming units respectively. 9,10,11 The effect of botulinum toxin A on the ability of the bacterial strains to produce biofilm was also determined by colorimetric assay as described by Sheikl et al (2001).12
The results showed that botulinum toxin A had no effect on the viability of the Staphylococcus strains and did not influence their ability to form biofilm (Table 2).
Folliculitis dissecans is a rare skin disorder that can cause significant emotional distress due to the appearance of the affected skin, as well as itching, pain, and permanent hair loss. This disease destroys hair follicles by causing deep follicular occlusion, followed by follicular rupture and deep inflammation of the hair follocles's bulb.13 Therefore, folliculitis dissecans is characterized as a cicatricial folliculitis.13
Folliculitis dissecans is frequently associated with Staphylococcus aureus, however, the results obtained in the present work, demonstrated that Staphylococcus lugdunensis could also be associated with folliculitis dissecans. In addition, the results also indicate that the healing effect of the botulinum toxin A, does not seem to be associated with the toxin's direct action on the pathogen, as no effect of the toxin was observed on the viability of the Staphylococcus strains isolated from the patients or their ability to produce biofilm.
In contrast, treatment with botulinum toxin A was very successful, with the patient reporting elimination of pain within the first few days and full recovery after 4 months. Therefore, it seems that the healing effect of the toxin is associated to the host response. However, the mechanism of action of the botulinum toxin A, has yet to be fully understood, as the toxin has the ability to interact with both, neuronal and immune cells.4
Nevertheless, several studies have indicated that under conditions of altered immune response, botulinum toxin A can act locally as an antagonist agent against altered immune suppressive state, induced by the cholinergic anti-inflammatory pathway, and the release of calcitonin gene-related peptide CGRP. 4,14,15,16,17
Therefore, it is possible that the intradermal administration of botulinum toxin A in patients with folliculitis dissecans is able to shift the patient's dysfunctional inflammatory reaction to a competent immune response, and as a consequence, restore the normal functioning of the affected area of the scalp. However, further research is needed to fully understand the mechanisms behind the healing effect of botulinum toxin A and to establish protocols to optimize its utilization as a therapeutic tool for folliculitis dissecans.
In summary, the results of this study suggest that botulinum toxin A may be used as an alternative treatment for folliculitis dissecans in patients who do not respond to the conventional treatment with antibiotics.
Simone Ramos Neri
ORCID: 0009-0004-7380-4795
Approval of the final version of the manuscript; study design and planning; collecting, analyzing, and interpreting data; effective participation in research guidance; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the literature; critical review of the manuscript.
Marcia Regina Franzolin
ORCID: 0000-0003-0654-639X
Approval of the final version of the manuscript; collecting, analyzing, and interpreting data; effective participation in research guidance. Célia Luiza Petersen
Vitello Kalil
ORCID: 0000-0002-1294-547X
Approval of the final version of the manuscript, study design and planning; effective participation in research guidance; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the literature; critical review of the manuscript.
Vaniky Duarte Marques
ORCID: 0009-0005-0307-6283
Approval of the final version of the manuscript; collecting, analyzing, and interpreting data; effective participation in research guidance.
Ronaldo Maciel Marques
ORCID: 0009-0006-8789-5936
Approval of the final version of the manuscript; collecting, analyzing, and interpreting data; critical review of the manuscript.
Marta Oliveira Domingos
ORCID: 0000-0003-4492-0709 Approval of the final version of the manuscript; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; effective participation in research guidance; critical review of the literature; critical review of the manuscript.
1. Egro FM, Coleman SR. Facial fat grafting: the past, present, and future. Clin Plast Surg. 2020;47(1):1-6.
2. Denadai R, Buzzo CL, Raposo-Amaral CA, Raposo-Amaral CE. Facial contour symmetry outcomes after site-specific facial fat compartment augmentation with fat grafting in facial deformities. Plast Reconstr Surg. 2019;143(2):544- 556.
3. Rotunda, AM. Injectable treatments for adipose tissue: terminology, mechanism, and tissue interaction. Lasers Surg Med.2019;41:714-720
4. Matarasso A, Pfeifer TM. Mesotherapy and injection lipolysis. Clin Plast Surg 2009;36:181-192.
5. Thomas MK, D'Silva JA, Borole AJ. Injection lipolysis: a systematic review of literature and our experience with a combination of phosphatidylcholine and deoxycholate over a period of 14 years in 1269 patients of Indian and South East Asian origin. J Cutan Aesthet Surg. 2018;11(4):222-228.
6. Antonio CR, Trídico LA, Esteves ALV. Nova técnica de rejuvenescimento facial com ácido hialurônico: delta V lifting. Surg Cosmet Dermatol. 2019;11(3):211-215.
7. Lu SM, Bartlett SP. On facial asymmetry and self-perception. Plast Reconstr Surg. 2014;133:873e-881e
8. Mulliken JB. The molders of this plastic surgeon and his quest for symmetry. J Craniofac Surg. 2004;15:898-908.
9. Cheong YW, Lo LJ. Facial asymmetry: etiology, evaluation, and management. Chang Gung Med J. 2011;34:341-351
10. Neuber GA. Fettransplantation. Chir Kongr Verhandl Dsch Gesellch fur Chir. 1893:22:66.
11. Saha S. Enxerto de gordura composta para correção de distrofia facial em caso de esclerodermia localizada. Surg Cosmet Dermatol. 2023;15:e20230181.
12. Matarasso A, Pfeifer TM. Mesotherapy and injection lipolysis. Clin Plast Surg 2009;36:181-192.
13. Duncan D, Rubin JP, Golitz L, Badylak S, Kesel L, Freund J, et al. Refinement of technique in injection lipolysis based on scientific studies and clinical evaluation. Clin Plast Surg 2009;36:195-209.
14. Kutlubay Z. Evaluation of mesotherapeutic injections of three different combinations of lipolytic agents for body contouring. J Cosmet Laser Ther. 2011;13(4):142-53.
15. Antonio CR, Trídico LA. Drug injcetion to reduce facial fat. J Clin Dermatol Ther. 2021;7:082.
16. Rittes PG. The use of phosphatidylcholine for correction of localized fat deposits. Aesthetic Plast Surg. 2003;27:315-8.
17. Talathi A, Talathi P. Fat busters: lipolysis for face and neck. J Cutan Aesthet Surg. 2018;11(2):67-72.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}