


Giovana Junqueira Gerbasi; Panny Rushaster Cordeiro de Albuquerque; Dayane de Assis Pereira Hansen Cavalheiro; Ana Carolina Silva Chuery; Neila Maria de Góis Speck
Submitted on: 06/23/2023
Accepted on: 10/04/2023
Funding source: None
Conflict of interest: None
How to cite this article: Gerbasi GJ, Albuquerque PRC, Cavalheiro DAPH, Chuery ACS, Speck NMG. CO2 laser treatment for vulvar syringoma: a case report. Surg Cosmet Dermatol. 2024;16:e20240269.
Syringoma is a rare benign adnexal tumor of the intraepidermal eccrine duct of unknown etiology. It is typically characterized by multiple, bilateral, yellow-brownish or skin-colored papules measuring 1-5 mm. Syringomas predominantly affect the face but can also be found in gluteal, pubic, vulvar, or thoracic regions. In this article, we report two cases of vulvar papules with a confirmed diagnosis of syringoma by histopathological analysis, which were successfully treated with carbon dioxide (CO2) laser therapy. The selected treatment approach was easy to implement and resulted in a favorable clinical response, including improvement of itching after the first session.
Keywords: Syringoma; Vulvar Diseases; Pruritus Vulvae; Adenoma; Sweat Gland; Lasers
Syringoma is a rare benign adnexal tumor of the intraepidermal eccrine duct (adenoma). It is characterized by multiple yellow, brown, or skin-toned papules measuring from 1 to 5 mm. The lesions are typically bilateral and symmetrical, but sometimes may be isolated. Syringomas are usually asymptomatic but may be associated with itching.1-4 Although they are more likely to affect white-skinned women during puberty and tend to occur sporadically,5,6 there are familial forms with autosomal dominant inheritance affecting both sexes equally and which seem to represent a form of mosaicism.7-9
The most commonly affected area is the face, particularly the eyelids and periorbital region, but the chest, neck, buttocks, pubic region, and vulva can also be affected. Vulvar syringoma should be included in the differential diagnosis of vulvar itching.1,2,10
Clinical diagnosis is challenging, as syringomas can be mistaken for different dermatitis or allergies. Thus, a definitive diagnosis should be obtained by histopathological analysis.13 Hematoxylin and eosin-stained sections show multiple small channels and epithelial cords consisting of a double layer of flat cuboidal cells within a fibrous stroma, usually without atypia.12
Several therapeutic techniques have been described, such as excision,13,14 electrocautery and electrodesiccation,15,16 oral isotretinoin, topical retinoic acid,13 laser application,4,17-19 and techniques combining trichloroacetic acid and carbon dioxide (CO2) laser.20,21 However, none of these treatments eliminate the risk of syringoma recurrence, often making treatment frustrating.20
Lasers have been used to treat several types of skin tumors, such as warts, sebaceous adenomas, and superficial basal cell carcinomas.15 The energy generated is absorbed by water, resulting in minimal heat conduction and thermal damage to adjacent tissue, allowing for more precision with minimal damage to healthy tissue and little scar formation.20
In this context, we report two rare cases of vulvar syringoma treated with CO2 laser, a method that, due to its advantages, should be more widely disseminated and used.
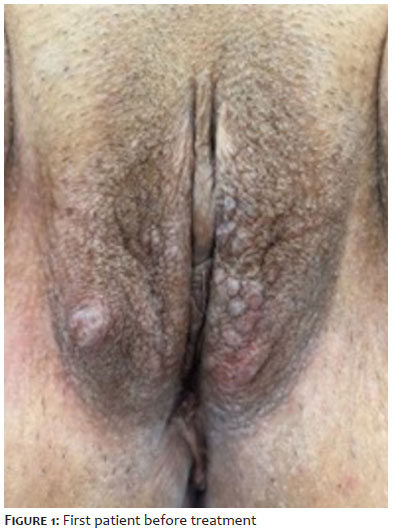
A 56-year-old woman who had undergone menopause 3 years earlier complained of intense vulvar itching, especially after showering, with no improvement after treatment with dexamethasone. Recent pap smear and mammography results were normal. Physical examination revealed multiple yellow-brown periocular papules, a hypochromic and scaly plaque on the upper portion of the right inner thigh suggestive of fungal infection, and multiple bilateral yellow-brown papules measuring 1 mm on the labia majora suggestive of syringoma. There was also a clean-based ulcer on the right labium majus measuring approximately 0.5 cm (Figure 1).
The fungal infection was treated with oral ketoconazole. Pathological examination of a biopsy of a papule on the left labium majus confirmed the diagnosis of syringoma. Treatment with CO2 laser vaporization was performed. The Smartxide device (Deka, Florence, Italy) was used in continuous mode, at a power of 12 W.
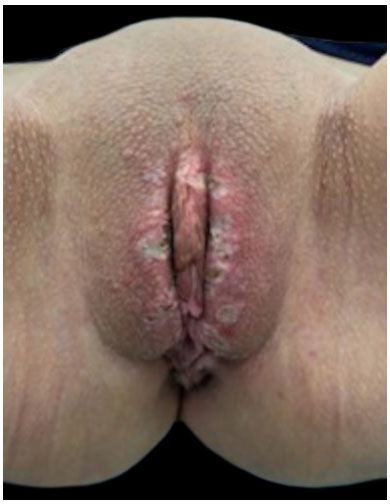
In the first laser session, surgical excision of the ulcer and vaporization of the lesions on the left labium majus were performed (Figure 2). At 15-day follow-up, the patient reported significant improvement in general itching but still complained of symptoms on the right labium majus. A second laser session was performed to treat the remaining lesions. Fifteen days after the second session (Figure 3, first patient 30 days after the first session), the patient reported localized hypopigmentation and mild itching but significant overall improvement. The patient was discharged and instructed to continue treatment for facial lesions on the Dermatology department.
A 46-year-old hypertensive woman, living with HIV since 1998, presented with vulvar itching since September 2020. She was clinically diagnosed with lichen sclerosus, and histopathology confirmed the diagnosis of vulvar syringoma (the biopsy was performed in December 2019). Initially, topical treatment with 0.1% mometasone furoate ointment and clinical monitoring were prescribed. The patient returned 30 days after the start of treatment with worsening itching. Physical examination revealed a hypochromic plaque on the labia majora and a small hypochromic area in the left perianal region, forming an “8” shape. Multiple syringomas were identified (Figure 4). Treatment with CO2 laser was performed.
Local anesthetic infiltration with 2% lidocaine with adrenaline was administered, followed by vaporization of the papules using the same device parameters as in the other case. At 30-day follow-up (Figure 5), the patient reported postoperative burning during urination and persistent itching. A second laser session was conducted to treat the remaining lesions at the same visit (Figure 6). There were no complications. The patient returned without complaints, with improved itching.
Syringomas are adenomas of sweat glands that affect several locations, most commonly the face. Lesions in the vulvar region are rare.1-3,17 They are typically asymptomatic and identified during routine examination.17,22,23 In the cases described in this report, both patients had vulvar lesions, and one also presented facial lesions. Intense itching was the main complaint that made them seek medical care. Treatment is usually indicated for aesthetic reasons, especially in visible areas, as these are benign, nonprogressive, and usually asymptomatic lesions.19,20,24
Although these lesions typically develop during puberty,5,6 our patients were diagnosed in adulthood, and one of them was already post-menopausal.
Syringomas pose a diagnostic challenge for gynecologists and dermatologists and should be considered in the differential diagnosis of vulvar papular lesions, itching, and vulvar pain; histopathological diagnosis is essential.16,22 Syringomas can be associated with other causes of vulvar itching, such as lichen.
Medical treatment is little effective, often requiring some form of surgical intervention.22,25 Surgery is commonly associated with hyperpigmentation, scar formation, and recurrence17,19; however, lasers provide better aesthetic results,20 as seen in these cases, with only slight hypopigmentation in one patient.
Lasers are a more costly method compared with others15 and are unavailable in many public services in Brazil. However, laser therapy has the advantage of being performed in an outpatient setting, with only local anesthesia, and requiring a few sessions. The availability of the equipment at our service allowed and facilitated early treatment.
There are several treatments for syringoma, including topical medications, surgery, and lasers, but few studies report the use of lasers on the vulva and postoperative follow-up results. In this study, CO2 laser vaporization was a good treatment option due to its ease of execution in an outpatient setting, patient satisfaction regarding aesthetic results, itching improvement, and no need for multiple sessions. Patients had good pain tolerance even though the procedure was performed only with local anesthesia, and there were no severe complications resulting from the treatment.
Giovana Junqueira Gerbasi
ORCID: 0009-0005-7887-1919
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; critical review of the literature; critical review of the manuscript.
Panny Rushaster Cordeiro de Albuquerque
ORCID: 0009-0008-8631-2019
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; critical review of the literature; critical review of the manuscript.
Dayane de Assis Pereira Hansen Cavalheiro
ORCID: 0009-0008-8164-1964
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; effective participation in research guidance; critical review of the literature; critical review of the manuscript.
Ana Carolina Silva Chuery
ORCID: 0000-0002-6645-0392
Approval of the final version of the manuscript; study design and planning; effective participation in research guidance; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the literature; critical review of the manuscript.
Neila Maria de Góis Speck
ORCID: 0000-0002-3713-5393
Approval of the final version of the manuscript; study design and planning; effective participation in research guidance; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the literature; critical review of the manuscript.
1. Mackie RM, Calonje E. Tumors of the skin appendages. In: Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook’s Textbook of Dermatology. 7th ed. London: Blackwell Publishing; 2004. p.1-34.
2. Patrizi A, Neri I, Marzaduri S, Varotti E, Passarini B. Syringoma: a review of twenty- nine cases. Acta Derm Venereol. 1998;78(6):460-2.
3. Gómez MI, Pérez B, Azaña JM, Nunez M, Ledo A. Eruptive syringoma: treatment with topical tretinoin. Dermatology. 1994;189(1):105-6.
4. Pérez-Bustillo A, Ruiz-González I, Delgado S, Alonso T, Ingelmo J. Vulvar syringoma: a rare case of vulvar pruritus. Actas Dermosifiliogr. 2008;99:580-1.
5. Bhat L, Goldberg LH, Rosen T. Basal cell carcinoma in a black woman with syringomas. J Am Acad Dermatol. 1998;39(6):1033-4.
6. Nuñez-Troconi J, Alvarado MEV. Syringoma of the vulva: an unusual presentation. Clinical, morphological and immunohistochemical aspects. Invest Clin. 2015;56(1):60-5.
7. Metze D, Wigbels B, Hildebrand A. Familial syringoma: a rare clinical variant. Hautarzt. 2001;52(11):1045-8.
8. Smith KJ, Skelton HG. Familial syringomas: an example of gonadal mosaicism. Cutis. 2001;68(4):293-5.
9. Belgaumkar VA, Chavan RB, Deshmukh NS, Kachare SA. Syringoma of the vulva. Dermatol Rev/Przegl Dermatol. 2021;108:299-304.
10. Garib G, Lullo JJ, Andea AA. Vulvar syringoma. Cutis. 2020;105(5):E7-E10.
11. Chandler WM, Bosenberg MW. Autoimmune acrosyringitis with ductal cysts: reclassification of case of eruptive syringoma. J Cutan Pathol. 2009;36(12):1312-5.
12. Soler-Carrillo J; Estrach T; Mascar JM. Eruptive syringoma: 27 new cases and review of the literature. J Eur Acad Dermatol Venereol. 2001;15(3):242-6.
13. Zitelli JA. Wound healing by secondary intention. A cosmetic appraisal. J Am Acad Dermatol. 1983;9(3):407-15.
14. Eedy DJ. Treatment of xanthlasma by excision with secondary intention healing. Clin Exp Dermatol. 1996;21(4):273-5.
15. Langtry JAA, Carruthers A. True electrocautery in the treatment of syringomas and other benign cutaneous lesions. J Cutan Med Surg. 1977;2(1):60-3.
16. Shalabi MMK, Homen K, Bicknell L. Vulvar syringomas. Proc (Bayl Univ Med Cent). 2021;35(1):113-4.
17. Wheeland RG, Bailin PL, Reynolds OD, Ratz JL. Carbon dioxide (CO2) LASER vaporization of multiple facial syringomas. J Dermatol Surg Oncol. 1986;12(3):225-8.
18. Riedel F, Windberger J, Stein E, Hormann K. Treatment of periocular skin lesions with the erbium: YAG LASER. Ophthalmologe. 1998;95(11):771-5.
19. Mendoza AMM, Vega JLM. Vulvar syringomas: case report. Rev Peru Ginecol Obstet. 2021;67(4):1-3.
20. Kang WH, Kim NS, Kim YB, Shim WC. A new treatment for syringoma. Combination of carbon dioxide LASER and trichloroacetic acid. Dermatol Surg. 1998;24(12):1370- 4.
21. Frazier CC, Camacho AP, Cockerell CJ. The treatment of eruptive syringoma in an african american patient with a combination of trichloroacetic acid and CO2 LASER destruction. Dermatol Surg. 2001;27(5):489-2.
22. Algeri P, Rodella R, Manfredini C, Algeri M. An unusual case of genital lesion: a vulvar syringoma. J Fam Reprod Health. 2021;15(1):70-3.
23. Sarac GA, Onder M. An alternative for the treatment of vulvar syringoma: 577nm pro- yellow laser. J Cosmet Dermatol. 2021;20(12):3931-3.
24. Young AW, Herman EW, Tovell HM. Syringoma of the vulva: incidence, diagnosis. and cause of pruritus. Obstet. Gynecol. 55(4):515-518, 1980.
25. Baker GM, Selim MA, Hoang MP. Vulvar adnexal lesions: a 32-year, single institution review from Massachusetts General Hospital. Arch Pathol Lab Med. 2013;137:1237-46.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}