


Caroline Andrade Rocha1; Célia Luiza Petersen Vitello Kalil2,3; Luciane Zagonel1; Patrícia Felipe França4; Valéria Campos1
Submitted on: 18/10/2023
Approved on: 07/01/2024
Financial support: None.
Conflict of interest: Valéria Barreto Campos: Speaker. Patrícia Felipe França: Employee.
How to cite this article: Rocha CA, Kalil CLPV, Zogonel L, França PF, Campos VB. Efficacy of oral omega-3 polyunsaturated fatty acids to prevent post-inflammatory hyperpigmentation in high skin phototypes after non-ablative fractional 1340 nm laser. Surg Cosmet Dermatol. 2024;16:e20240309.
INTRODUCTION: Non-ablative fractional lasers are well-known effective treatments for skin rejuvenation. However, the high incidence of post-inflammatory hyperpigmentation increases the risk of complications, especially in higher skin phototypes. Caviar phospholipid supplementation has been used successfully to reduce the inflammatory process, which may be beneficial to manage post-inflammatory hyperpigmentation after laser.
OBJECTIVE: To compare the incidence of post-inflammatory hyperpigmentation in high phototypes after caviar phospholipid supplementation.
METHODS: 20 patients underwent a non-ablative fractional laser session (Nd:YAP 1340nm, Zye Vydence, Brazil), and 10 of them used 200 mg of caviar phospholipid orally daily for 15 days before treatment and 40 days after. Patient images were evaluated before and after 40 days of laser application. Clinical assessment was based on the presence or absence of post-inflammatory hyperpigmentation. Statistical analysis was performed using the Z test.
RESULTS: We observed no cases of post-inflammatory hyperpigmentation in the experimental group; however, the control group presented 30%.
CONCLUSIONS: Caviar phospholipid may be an option for preventing post-inflammatory hyperpigmentation after non-ablative fractional lasers, aiming to avoid adverse events.
Keywords: Lasers; Skin; Rejuvenation; Fatty Acids; Omega-3.
In dermatology, the term “high skin phototype” encompasses people with darker skin tones and comprises a wide range of racial and ethnic groups, including people of African, Asian, and Pacific Islander descent, Native Americans, Alaskans, Hispanics, Indians, Pakistanis, and of Middle Eastern origin, among others.1 Skin color can be categorized using the Fitzpatrick skin phototype classification, which ranges from type I to type VI, with type VI being the darkest. This skin typing system was developed originally to characterize the skin’s response to sunlight and UV radiation and correlate skin color to burning (in lighter skin types) or tanning (in darker skin types). Most patients with “high phototype” have been classically defined as skin types IV to VI.2
Lasers can be non-ablative fractional or ablative fractional. Ablative lasers use longer wavelengths and can disrupt the skin layers, while non-ablative lasers keep the stratum corneum intact. The non-ablative fractional laser (NAFL) is an innovative technology in aesthetic dermatology that aims to improve the skin appearance, especially regarding facial rejuvenation. Non-ablative lasers emit light within the infrared range (1000–1600 nm) of the electromagnetic spectrum. The most commonly used wavelengths are 1340 nm, 1410 nm, 1440 nm, 1540 nm, and 1550 nm.3
NAFL is indicated for photoaging, rhytides, melasma, sagging, stretch marks, scars, and dyschromia. The results are satisfactory, and recovery occurs within 1 to 5 days, depending on the energy and amount of skin affected by the treatment (thermal microzones). Also, adverse events are minimal, especially in lighter phototypes. However, it is essential to highlight that this procedure requires several sessions, especially when they are less aggressive, making the treatment costly.3
This laser acts by generating microscopic columns of thermal injury with dermal-epidermal coagulation without ablation of the epidermis. By delivering the energy more precisely and maintaining the integrity of the epidermis, it acts more gently, reducing the chances of complications and the recovery period compared to the ablative fractional laser.3 NAFL is a safer treatment for different skin phototypes. However, it can generate local inflammation, culminating in post-inflammatory hyperpigmentation (PIH), especially in higher phototypes.
The risk of PIH following dermatological procedures is well known. It can affect any individual, regardless of age and sex, being more evident in higher skin phototypes and appearing as hyperpigmented spots on the skin.4-6 Previous history of PIH, presence of PIH, and high skin phototype (Fitzpatrick IV-VI) are considered risk factors. PIH is a pigmentary disorder in which the skin develops reactive hypermelanosis due to different exogenous or endogenous factors induced by excess melanin in the epidermis and aberrant distribution of melanin pigment. Inflammatory and infectious conditions, such as lesions of different etiologies such as dermatophytosis, viral exanthema, allergic reactions, erythematous-scaly dermatoses, and cosmetic procedures, such as chemical peels, laser, and dermabrasion, can trigger PIH. The degree and depth of inflammation and skin color likely influence the severity of PIH. The condition has a chronic course with irregularly shaped lesions ranging from light brown to bluish-gray.7 Prevention and treatment of underlying inflammatory diseases are crucial in PIH management. Topical depigmenting creams, including arbutin, hydroquinone, kojic acid, and azelaic acid, have also been tried with limited success.7
Overproduction or aberrant release of melanin in response to inflammatory stimuli and circumstances causes PIH. The oxidation of arachidonic acid produces eicosanoids, which are involved in cell signaling.8 During the inflammatory response, prostaglandins, leukotrienes, cytokines, nitrogen, and reactive oxygen species stimulate melanocyte proliferation and increase melanogenesis.8 In vitro studies have demonstrated that thromboxane B2, leukotriene C4, histamine, prostaglandin E2, and leukotriene D4 can activate melanocytes. Higher levels of immunoreactive tyrosinases are linked to the upregulation of these metabolites, resulting in greater melanin production and transfer of melanosomes to keratinocytes.8
Caviar phospholipids (CF) consist of a mixture of high levels of fatty acids, including polyunsaturated fatty acids (PUFAs), docosahexaenoic acid (DHA), eicosapentaenoic acid (EPA), astaxanthin, and alpha-tocopherol which are beneficial for skin health.9,10 Although some caviar-based cosmetic products have appeared on the market with the function of anti-aging the skin, the effects of caviar on the skin are still unclear.
PUFAs play a regulatory role, modulating the inflammatory response by producing eicosanoids, including series 3 prostaglandins, thromboxanes, and leukotrienes. Studies suggest that PUFAs play an essential role in skin homeostasis, modulating barrier function and inflammatory/immune reactions involved in various skin diseases.11,12 PUFAs reduce skin inflammation by competing with arachidonic acid and stimulating the production of eicosanoids.11,12 This study aimed to assess the influence of oral supplementation of 200 mg of CF on the incidence of PIH in black skin after a non-ablative laser.
It is a prospective, randomized study conducted in two private and independent dermatological clinics (Clinics A and B). We selected 20 Caucasian volunteers aged 30 to 60 years with Fitzpatrick skin phototypes IV-VI. Exclusion criteria were phototypes below IV, pregnant women, lactating women, patients with unrealistic expectations regarding possible results, and patients using depigmenting agents or topical corticosteroids. All participants enrolled in this study signed an informed consent form.
Research Randomizer at https://www.randomizer.org generates the randomization. Patients in the experimental group (Group I) received 55 capsules, each containing 200 mg of CF orally, and were instructed to take one capsule a day at home after dinner. Individuals allocated to the control group (Group II) did not use the medication.
The dynamics of the study were as follows: each patient visited Clinic A three times (at T0, T15, and T55): at the beginning, an investigator1 distributed the treatment to patients allocated to the experimental group,2 classified the skin phototypes according to the Fitzpatrick scale and3 captured standardized images of the patients using the equipment Visia Canfield Imaging Systems Inc. Fifteen days later (T15), the patients returned to Clinic A and underwent a non-ablative fractional laser session (Nd: YAP 1340 nm, Zye Vydence, Brazil), with 2-3 passes over the entire face, except upper eyelids, following the parameters of 110 MJ, 10 ms, 100 MZT. Forty days after laser application (D55), patients returned to recapture facial images.
Patients were instructed to use a broad-spectrum sunscreen with SPF 50 and the capsules provided daily. In Clinic B, a dermatologist reviewed and evaluated each participant’s paired images taken at baseline (T0) and day 55 (T55). Clinical assessment was based on post-inflammatory hyperpigmentation and was classified as 1: no or 2: yes. Statistical analysis was performed using the Z test to compare proportions with the R software.
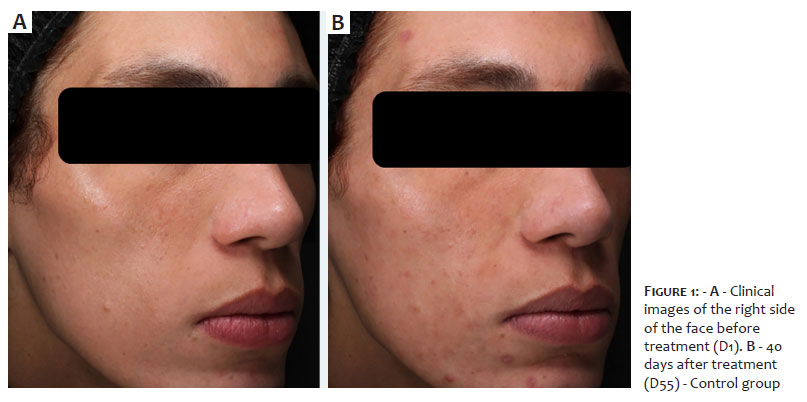
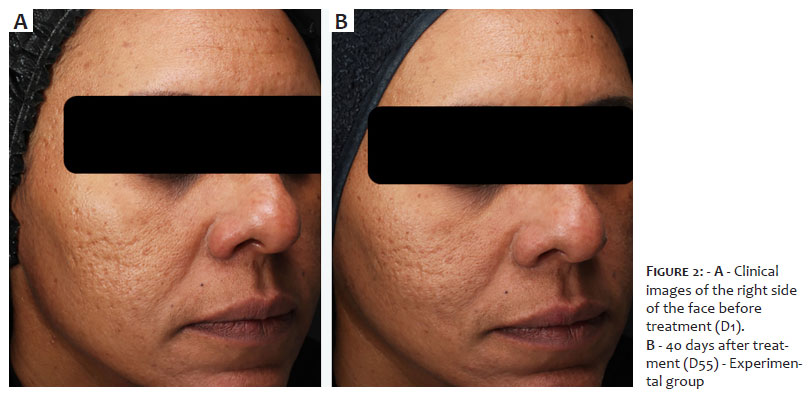
No adverse events related to the supplement were reported. The main adverse event was PIH in 30% of the control group (Figure 1), with no cases observed in the experimental group (Figure 2). The Z test to compare proportions observed that the difference was statistically significant; therefore, we rejected the null hypothesis that the proportions of cases with PIH are statistically equal (p=0.027).
Changes related to skin hyperpigmentation, such as lentigo, melisma, and PIH, are frequent complaints in dermatological offices and impact significantly the patients’ quality of life. Despite being very common, the literature lacks preventive treatments that could be indicated before risk situations, such as laser on skin with higher phototypes. Despite several treatments available, many can lead to a process irritative with subsequent worsening or even development of PIH. It is more evident in these phototypes, which makes treatment even more challenging for patients with phototypes between III-VI.5,6,13 The risk of PIH can be a limiting factor in the choice of dermatological treatment in the skin with higher phototypes, sometimes restricting therapeutic options, as hyperpigmentation is one of the most common post-laser complications.
Resurfacing using an ablative fractional laser is considered the gold standard for skin rejuvenation, especially in the skin with intense photoaging, presenting surprising results. However, the prolonged recovery time and discomfort are limiting factors.14 Furthermore, the risk of adverse events is greater in patients with higher phototypes.
The non-ablative fractional laser aims to generate thermal damage to the dermis through coagulation columns in the skin that stimulate collagen remodeling with minimal effects on the epidermis. It allows rapid tissue repair with few adverse events while keeping the skin intact without ablation. This laser works for skin rejuvenation in moderately aging skin, with excellent results, less discomfort, and a lower risk of complications.3
Although the non-ablative fractional laser is a therapy with excellent results in skin rejuvenation and is safer for patients with higher phototypes, as it is a procedure that generates irritation and consequently an inflammatory process, it can cause PIH in predisposed skin.15 Early treatment and even preventive care are essential to reduce long-term sequelae, such as hyperpigmentation and scars, which can be very difficult to treat or also reduce treatment adherence, as most treatments include several sessions. However, there are no studies on the use of a 1340 nm Nd: YAP (Neodymium: Yttrium Aluminum Perovskite) laser in higher skin phototypes and association with active ingredients in an attempt to minimize adverse events of hyperchromia. It is recommended to use refrigeration during treatment and photoprotectors, topical corticosteroids, and products with depigmenting action to reduce the risk of PIH. However, to date, little has been described about systemic prophylaxis for the occurrence of PIH after procedures.
Oral tranexamic acid has already been used for this purpose; however, without significant results.16 Furthermore, it is a medication that can have significant adverse events. Tranexamic acid started soon after the procedure would affect melanogenesis, blocking the interaction between melanocytes and keratinocytes and reducing inflammatory cytokines that stimulate melanocytes.16 Several mechanisms are described. Nevertheless, the exact action of tranexamic acid on melanogenesis is still uncertain.
Previous studies have demonstrated the biological activities of marine fish oil. CF supplementation probably has the potential to reduce inflammatory processes, which may be beneficial to manage PIH. CF exerts a regulatory function by modulating physiological and pathological conditions on multiple mechanisms, such as the inflammatory response through the production of eicosanoids, which are inflammatory mediators of lipid origin, synthesized from omega-6 fatty acids, such as arachidonic acid (AA) or omega-3 fatty acids, such as eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), including prostaglandins, thromboxanes, and leukotrienes. The literature corroborates the findings of this study by demonstrating the reduction of hyperpigmentation in the skin with the use of polyunsaturated fatty acids from fish oil.17,18 It is worth highlighting that although CF apparently reduces the risk of PIH, combining sunscreen and established topical treatments is essential.
Fish oil can inhibit radiation-induced inflammation and hyperpigmentation (UVR) and improve skin barrier function. It also promotes skin protection against dry skin stimulation and accelerates the recovery of skin physiology. Omega 3 appears to have a photoprotective role in sun-exposed skin,19 which may also be related to protection against PIH, as observed in this study.
Most studies that assess polyunsaturated fatty acid supplementation did not observe critical adverse events. The only adverse event described is mild gastrointestinal discomfort in a small number of patients,20, 21 that was not reported in our study. The safety of this supplement, combined with its anti-inflammatory and photoprotective properties, reinforces the promising characteristics for use in high phototypes who undergo procedures that generate irritation.
The study demonstrated that daily oral administration of 200 mg of CF can be an effective and well-tolerated treatment option for preventing PIH in the skin with a higher phototype after a non-ablative laser. The results of this study need to be confirmed in randomized, controlled studies with a larger sample size. l
Caroline Andrade Rocha
ORCID: 0000-0002-0116-8548
Approval of the final version of the manuscript; preparation and writing of the manuscript; collecting, analyzing and interpreting data; critical literature review; critical review of the manuscript.
Célia Luiza Petersen Vitello Kalil
ORCID: 0000-0002-1294-547X
Approval of the final version of the manuscript; conception and planning of the study; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the manuscript.
Luciane Zagonel
ORCID: 0000-0002-7687-6557
Approval of the final version of the manuscript; collecting, analyzing, and interpreting data; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Patrícia Felipe França
ORCID: 0000-0002-2047-4161
Approval of the final version of the manuscript; study design conception and planning.
Valéria Barreto Campos
ORCID: 0000-0002-3350-8586
Approval of the final version of the manuscript; study design and planning; collecting, analyzing, and interpreting data; effective participation in research guidance; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the manuscript.
1. Desai M, Gill J, Luke J. Cosmetic procedures in patients with skin of color: clinical pearls and pitfalls. J Clin Aesthet Dermatol. 2023;16(3):37-40.
2. Sachdeva S. Fitzpatrick skin typing: applications in dermatology. Indian J Dermatol Venereol Leprol. 2009;75(1):93-96.
3. Favaro J, Loureiro VB. Fractional Non-ablative Laser and Drug Delivery. In: Kalil CLPV, Campos V. Drug Delivery in Dermatology. Springer, 2021.
4. Davis EC, Callender VD. Postinflammatory hyperpigmentation: a review of the epidemiology, clinical features, and treatment options in skin of color. J Clin Aesthet Dermatol. 2010;3(7):20-31.
5. Elbuluk N, Grimes P, Chien A, Hamzavi I, Alexis A, Taylor S, et al. The pathogenesis and management of Acne-induced Post-inflammatory Hyperpigmentation. Am J Clin Dermatol. 2021;22(6):829-836.
6. Kaufman BP, Aman T, Alexis AF. Postinflammatory Hyperpigmentation: epidemiology, clinical presentation, pathogenesis and treatment. Am J Clin Dermatol. 2018;19(4):489-503.
7. Naik P. Getting to the core of contemporary therapies for Post-inflammatory Hyperpigmentation. J Drugs Dermatol. 2022;21(3):276-283.
8. Medrano EE, Farooqui JZ, Boissy RE, Boissy YL, Akadiri B, Nordlund JJ. Chronic growth stimulation of human adult melanocytes by inflammatory mediators in vitro: implications for nevus formation and initial steps in melanocyte oncogenesis. Proc Natl Acad Sci USA. 1993;90(5):1790-1794.
9. Kendall AC, Kiezel-Tsugunova M, Brownbridge LC, Harwood JL, Nicolaou
10. A. Lipid functions in skin: differential effects of n-3 polyunsaturated fatty acids on cutaneous ceramides, in a human skin organ culture model. Biochim Biophys Acta Biomembr. 2017;1859(9 Pt B):1679-1689.
11. Yoshida S, Yasutomo K, Watanabe T. Treatment with DHA/EPA ameliorates atopic dermatitis-like skin disease by blocking LTB4 production. J Med Invest. 2016;63(3-4):187-191.
12. Barcelos RC, Segat HJ, Benvegnú DM, Trevizol F, Roversi K, Dolci GS, et al. Trans fat supplementation increases UV-radiation-induced oxidative damage on skin of mice. Lipids. 2013;48(10):977-987.
13. McCusker MM, Grant-Kels JM. Healing fats of the skin: the structural and immunologic roles of the omega-6 and omega-3 fatty acids. Clin Dermatol. 2010;28(4):440-451.
14. Markiewicz E, Karaman-Jurukovska N, Mammone T, Idowu OC. Post- Inflammatory Hyperpigmentation in dark skin: molecular mechanism and skincare implications. Clin Cosmet Investig Dermatol. 2022;15:2555-2565.
15. Campos V, Merheb J, Romero J, Kalil CL. Estudo comparativo do laser fracionado não ablativo 1340nm para rejuvenescimento facial: alta energia com passagem única versus energia média e passagem tripla. Surg Cosmet Dermatol. 2017;9(3):229-236.
16. Oh SM, Lee YE, Ko MJ, Baek JH, Shin MK. Proposal of facial pigmentary unit and facial hyperpigmentation type for Fitzpatrick skin types II-IV. Skin Res Technol. 2023;29(1):e13251.
17. Lindgren AL, Austin AH, Welsh KM. The use of Tranexamic Acid to prevent and treat Post-Inflammatory Hyperpigmentation. J Drugs Dermatol. 2021;20(3):344-345.
18. Ando H, Funasaka Y, Oka M, Ohashi A, Furumura M, Matsunaga J, et al. Possible involvement of proteolytic degradation of tyrosinase in the regulatory effect of fatty acids on melanogenesis. J Lipid Res. 1999;40(7):1312-1316.
19. Ando H, Ryu A, Hashimoto A, Oka M, Ichihashi M. Linoleic acid and alpha- linolenic acid lightens ultraviolet-induced hyperpigmentation of the skin. Arch Dermatol Res. 1998;290(7):375-381.
20. Latreille J, Kesse-Guyot E, Malvy D, Andreeva V, Galan P, Tschachler E, et al. Association between dietary intake of n-3 polyunsaturated fatty acids and severity of skin photoaging in a middle-aged Caucasian population. J Dermatol Sci. 2013;72(3):233-239.
21. Jung JY, Kwon HH, Hong JS, Yoon JY, Park MS, Jang MY, et al. Effect of dietary supplementation with omega-3 fatty acid and gamma-linolenic acid on acne vulgaris: a randomised, double-blind, controlled trial. Acta Derm Venereol. 2014;94(5):521-525.
22. Kristensen S, Schmidt EB, Schlemmer A, Rasmussen C, Johansen MB, Christensen JH. Beneficial effect of n-3 polyunsaturated fatty acids on inflammation and analgesic use in psoriatic arthritis: a randomized, double blind, placebo-controlled trial. Scand J Rheumatol. 2018;47(1):27-36.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}