


Juliana Reis de Sousa Zacarias1; Roberpaulo Anacleto Neves1; Yara Alves Caetano2
Financial support: None.
Conflict of interest: None
Submitted on: 20/11/2022
Approved on: 03/07/2023
How to cite this article: Zacarias JRS, Neves RA, Caetano YA. Mohs surgery for melanoma treatment: a systematic literature review. Surg Cosmet Dermatol. 2023;15:e20230201.
Mohs micrographic surgery, created in 1930 by Frederich Mohs, is a world-renowned technique to treat skin cancers. Currently, it is used to treat basal cell and squamous cell carcinomas, ensuring excellent cure rates for patients. However, regarding the treatment of cutaneous melanoma, the use of Mohs surgery is not a consensus among specialists. This article aims to elucidate whether Mohs surgery is a safe and effective treatment for melanoma skin cancer.
Keywords: Melanoma; Mohs Surgery; Skin neoplasms; Treatment Outcome; Prognosis.
Mohs micrographic surgery (MMS) was first described in the 1930s by the American physician Friedrich Mohs. In 1933, Mohs created the concept of micrographic chemosurgery, and after three years of the discovery, he began to treat his patients using this technique.1 After several successful surgeries, associating high cure rates and good secondary intention healing, Mohs surgery impressed mainly dermatologists, and it was accepted as an innovative and high-impact technique for skin tumors.2 The current Mohs surgery differs from the technique initially created in 1930 and may also vary between surgeons and institutions.3
Basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) are the two tumors most treated by Mohs surgery.4 The excellent cure and low recurrence rates obtained with MMS show that the Mohs technique is already very well established for both carcinomas. However, as melanoma has a strong tendency to invade vascular walls and metastasize, chemosurgery for this type of neoplasm differs and is a matter of debate regarding its effectiveness and benefit.5
Primary cutaneous melanoma is a neoplasm that affects melanocytes, the cell responsible for melanin production. This cell, present in the basal layer, can infiltrate deeper layers when a mutation occurs, thus denominating invasive melanoma (IM); or remain only in the most superficial layer, being characterized as melanoma in situ (MIS).6 This tumor tends to invade adjacent tissues in a clinically invisible way. Therefore, it must have a rigid and careful evaluation of its margins.7
The current challenge is to find effective therapies that present a low surgical risk for the patient, with the possibility of preserving as much tissue as possible, combined with negative histological margins that reduce the chance of recurrence. One of the reasons to discuss the use of MMS in melanomas is that this type of cancer presents non-contiguous growth, a fact that was refuted by Friedrich Mohs in one of his articles where he reports that melanoma spreads contiguously before spreading systemically.8 Another critical point for this discussion is the difficulty in distinguishing melanoma atypical melanocytes from photodamaged skin atypical melanocytes. However, the experience of the surgeon and the biochemical technician can minimize this difficulty with the combined use of staining and immunohistochemistry.
MMS is a technique based on maximum tissue preservation with serial frozen sections, combined or not with staining and immunohistochemistry. The surgery aims to preserve as much tissue as possible, combining a good aesthetic and functional result, especially in noble and exposed areas such as the head and neck, areas where the preservation of the aesthetic function is of great importance to the patient. MMS, however, requires a well-trained team, as a qualified professional must know how to interpret the histological sections, thus ensuring that the margins are free of tumor tissue.
Currently, the standard treatment for melanoma is global excision (GE). This technique is based only on excision with wide margins and does not perform perioperative microscopic analysis of the removed margins.9 In GE, as there is no analysis of the excised margins, it is necessary to make a safety margin greater than usual to guarantee negative margins, impairing the patient's aesthetics. Even with a larger margin, conventional surgery may not remove the entire tumor area, allowing tumor recurrence in a more severe form.
In Brazil, despite being a recognized surgery for more than 30 years, Mohs surgery has only recently become evident. One of the reasons is the lack of qualified professionals to perform the surgery and the scarcity of training centers since the success of the technique depends on the high skill of the laboratory technician and the surgeon's experience. The lack of public policies that include Mohs micrographic surgery in the list of surgeries against skin cancer also hinders the dissemination of this technique.6
Several therapies have been proposed to treat Cutaneous Melanoma (CM), including non-surgical therapies such as cryotherapy, imiquimod, laser, radiotherapy, and curettage.10 However, according to the American Academy of Dermatology guidelines, the primary therapy against this cancer is surgical excision, and the primary objective of this excision is to achieve free histological margins to prevent recurrences and increase survival.11
In the 1970s, Alexander Breslow created a concept of histological staging for melanoma based on tumor thickness.9,12 From this, the prognosis of melanoma can be evaluated more reliably, using mainly the invasion stage and its thickness.12 Also, the location of the tumor and the patient's characteristics help evaluate the prognosis and therapeutic choice. In addition, the body areas affected by the tumor also contribute enormously to assessing whether or not using MMS is suitable for melanoma.
Although MMS is an increasingly advocated technique for melanoma, GE is still the most widely used technique. This review aims to elucidate the benefits and importance of using Mohs micrographic surgery to treat melanoma, emphasizing data such as cost, recurrence, overall survival and disease-free survival, minimum margins to extinguish the tumor, and use of staining and/or immunohistochemistry.
It is a systematic review aiming to answer "Is Mohs Surgery an effective and safe therapy to treat melanoma?". We searched the electronic databases MEDLINE/Pubmed between 06/25/2022 and 07/26/2022, following the recommendations of the PRISMA guideline. In the first stage, we selected the keywords melanoma, skin neoplasm, Mohs surgery, treatment outcome, and prognosis, which were later crossed with the Boolean operator AND, generating a total of 127 results. The filters used were "last 10 years", "human", and "full text". The selected languages were English and Portuguese. After all the steps, we obtained 67 results. Articles were initially selected by title and abstract to verify eligibility for this study. Subsequently, we extracted data regarding the general characteristics of the sample, recurrence, overall survival, disease-free survival, margins, and use of immunomarkers and staining. The inclusion criteria were prospective cohort, retrospective, and cross-sectional articles, papers correlating melanoma and Mohs surgery, contemplating melanoma and its subtypes and treatment therapies, presenting Mohs surgery as a treatment for melanoma, and published between 2012 and 2022. Exclusion criteria were articles that showed therapies for skin cancer other than Mohs, focusing on non-melanoma skin cancer, articles emphasizing melanoma, and areas of medicine other than dermatology. We also excluded reviews, articles unavailable for reading, and letters to the editor. In the end, we selected 12 articles to compose this article.
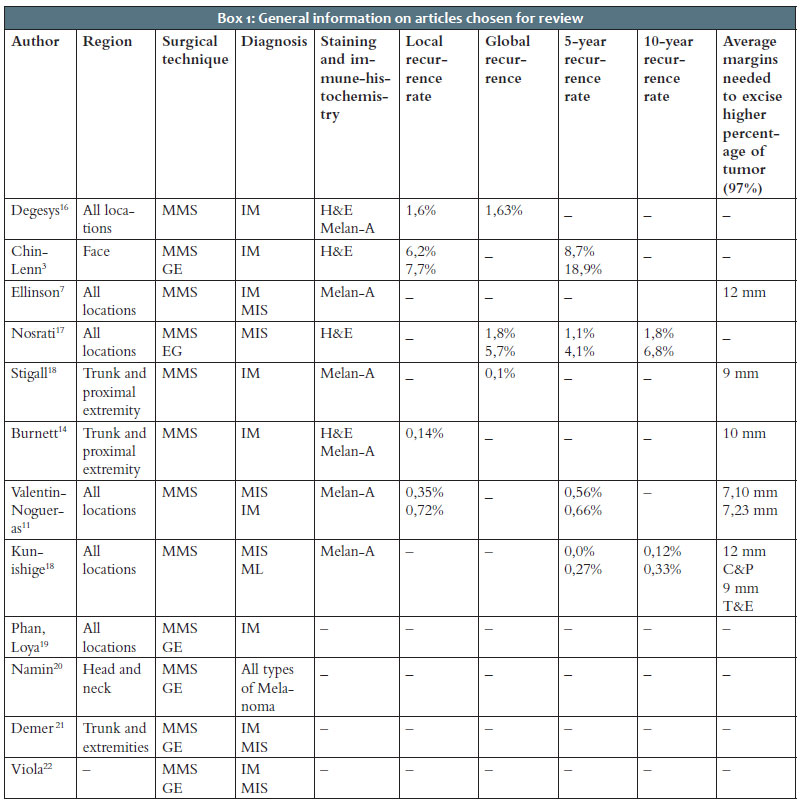
The mean follow-up time for patients in each study was 2.88 years. The average age of the total sample was 63.65 years. Most of the lesions in this study were in the extremities (44.3%), followed by the trunk (32.4%) and head and neck (20.8%). Regarding immunohistochemistry and staining, most authors used melan-A (melanoma antigen recognized by T1 cells), and the prevalent immunostaining was hematoxylin and eosin (H&E). Table 1 shows the general characteristics of the articles chosen to compose the present study.
The recurrence rate is a controversial aspect that is difficult to agree on. Thus, it was arbitrarily considered, as authors defined the recurrence rate in their way. Given this arbitrariness, the recurrence rate is not the best parameter to assess MMS effectiveness. Concerning surgical margins, most articles considered 10 mm as ideal to achieve free margins.
Regarding overall survival, many articles compared MMS and GE, creating a parallel mainly with the percentage of overall survival. Only five authors assessed this data, and the overall survival rate for MMS was 93.78%. For the authors who compared it with GE, the overall survival rate for this group was 90.27%. Overall survival rates showed good results for MMS. Studies using MMS showed an overall survival rate of 92.90%. The disease-free survival rate for melanoma was a variable that presented excellent results. The average for the MMS was 95.9%, while for the GE was 88%. The Breslow thickness is the primary prognostic marker for melanoma. Most studies presented the Breslow thickness as the main recurrence and mortality predictor of invasive melanoma and some evaluated the average Breslow thickness. Most of the patients studied had a Breslow depth of <1 mm.
The results of this review corroborate the hypothesis of efficacy and adequacy of MMS for invasive and in situ melanoma. This assessment is paramount since melanoma is the most prevalent cancer in Brazil, accounting for 30% of malignant tumors in the country. Therefore, devising strategies for its treatment and prevention impact public health significantly. However, Brazil needs more studies on this topic, given that most of the studies analyzed in this article were conducted in the United States.
The low recurrence and survival rates compared with GE show that it is an effective technique to treat and cure melanoma. Nevertheless, more studies must be performed to corroborate these results. The NCCN (National Comprehensive Cancer Network) and the AAD (American Academy of Dermatology) guidelines recommend MMS only for melanoma in situ and lentigo maligna subtype 1.13,14 Although some studies have shown that MMS is effective for invasive melanoma, its use for this type of tumor remains restricted.
The average age of the samples reveals a characteristic of this type of cancer: it mostly affects elderly people aged around 60 years. One of the reasons would be the longer exposure time to the sun, and a prevention program based on this environmental factor may be essential to reduce this neoplasm rate. A significant advantage of the MMS is the perioperative evaluation and absence of general anesthesia for the procedure. Moreover, high cost due to the use of sophisticated materials and equipment remains a barrier to the use of the MMS.
Recurrences, whether arising from a contiguous tumor or not, present a significant inconvenience in melanoma treatment, as a new surgical approach is required, resulting in greater tissue loss and costs for the patient. Also, the recurrence tissue may present a more aggressive tumor characteristic than the primary tumor, with a deeper Breslow thickness and the development of metastases.3 Therefore, preventing recurrence is a key point to define the success of the therapy used to treat melanoma.
Degesys studied MMS in invasive melanoma, and although their study used a Breslow thickness of <1 mm, it used the MMS well, resulting in a low recurrence rate (1.6%) and absence of metastases, thus showing good control of the primary tumor.16 In the Chin-Leen study, no patient submitted to MMS presented recurrence.3 Also, Valentin-Nogueras demonstrated the effectiveness of MMS combined with Melan-A, resulting in low local recurrence rates.11
The disease-free survival rate showed excellent results for MMS compared to GE. Few authors showed this data; however, it impacts significantly the comparison of which surgical technique has the best outcome and greater efficiency, as well as the recurrence rates. This review evidences the high success rates in melanoma treatment using MMS. However, Demer observed that the survival rate varies with the location of the melanoma, and therefore the therapy must be individualized.21
Many studies used immunostaining in their research. Frozen immunostaining is a technique that increases surgical costs, as it is a complex and time-consuming process that requires a qualified and experienced team. However, MMS combined with immunostaining and immunohistochemistry increased the accuracy of margin assessment, and the most used technique in immunohistochemistry was Melan-A. Melan-A combined with H&E help in MMS accuracy in differentiating between atypical melanocytes and photodamaged skin.3
The Valentin-Nogueras study notes that Melan-A potentiated good results in MMS, reaching lower recurrence rates and higher survival rates than GE techniques.11 However, Nosrati did not use immunohistochemistry and states that this technique can result in errors, which can cause unnecessary extension of the margins for excision, mistaking sun-damaged skin for tumor cells.17 Therefore, the specialist discretion should decide the use of this technique.
In most studies, a margin of 12 mm was adequate for a melanoma clearance of 97%. Degesys showed that a margin of 5 mm would be necessary to remove 62.6% of melanomas, and additional margins were needed to increase this percentage. The NCCN recommends margins of 0.5 cm to 1.0 cm for melanoma in situ and margins of 1 cm to 2 cm for invasive melanoma, based on a Breslow depth of 4.5 mm.
One of the ways to reduce MMS costs in Brazil is to include it in the list of surgeries for skin tumors in the Public Healthcare System (Sistema Único de Saúde - SUS). Another essential issue is the implementation of preventive measures and early cancer diagnosis. Mohs, in one of his studies, states that an important criterion is that MMS is more successful when performed in melanomas diagnosed in the early stages.15 Even conventional surgery would not be able to achieve high chances of cure in melanomas diagnosed in late stages.
Furthermore, the MMS needs a well-trained team for the serial evaluation of histological sections to ensure that the excision is complete and free of tumor margins. The creation of Mohs surgery centers can train surgeons and laboratory technicians capable of interpreting the slides.
A fundamental aspect of MMS in melanoma is its ability to spare healthy tissue in exposed areas, such as the face, and preserve noble structures, such as the eyeball and facial nerve. As GE does not perform perioperative analysis of the margins, this type of surgery can compromise important structures to extirpate the entire tumor by increasing the size of the margins, thus creating a choice between preserving a noble structure or reaching negative margins.
The main limitations of this study were the divergences in the samples. Some studies were conducted with samples above N=400,000, while others with N=123, which is an inconvenience when defining parameters. Also, not all studies analyzed the same data, thus making it more difficult to compare the information extracted from each author.
Recurrence prevention and increased overall disease-free survival is the Mohs surgery's ultimate goal. Although MMS is a well-established and effective surgical technique for MIS and lentigo maligna, according to existing articles, this technique is not used routinely as a treatment option for these tumors. Regarding invasive melanoma, further studies can be conducted since the articles evaluated in this review leave this hypothesis open, demonstrating that invasive melanoma is a tumor difficult to treat, regardless of the therapy used. Immunohistochemistry and staining proved to be great allies in the success of MMS. Given all the aspects analyzed here, MMS is an effective and efficient surgical technique to treat melanoma. Planning regarding early diagnosis and melanoma prevention can contribute to reducing the rates of this cancer in Brazil, as well as increasing training centers for Mohs surgeons.
Juliana Reis de Sousa Zacarias
ORCID:
ORCID: 0009-0007-6707-9605
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation.
Roberpaulo Anacleto Neves
ORCID:
ORCID: 0000-0003-1181-2373
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; critical literature review; critical revision of the manuscript.
Yara Alves Caetano
ORCID:
ORCID: 0000-0001-8483-8617
Approval of the final version of the manuscript; active participation in research orientation; critical literature review.
1. Trost LB, Bailin PL. History of Mohs surgery. Dermatol Clin. 2011;29(2):135-9.
2. Brodland DG, Amonette R, Hanke CW, Robins P. The history and evolution of Mohs micrographic surgery. Dermatol Surg. 2000;26(4):303-7.
3. Chin-Lenn L, Murynka T, McKinnon JG, Arlette JP. Comparison of outcomes for malignant melanoma of the face treated using Mohs micrographic surgery and wide local excision. Dermatol Surg. 2013;39(11):1637-45.
4. Shriner DL, McCoy DK, Goldberg DJ, Wagner RF Jr. Mohs micrographic surgery. J Am Acad Dermatol. 1998;39(1):79-97.
5. Mohs FE. Chemosurgery for melanoma. Arch Dermatol. 1977;113(3):285-91.
6. Sanchez F, Marques H. Cirurgia micrográfica de Mohs: manual prático e atlas. Rio de Janeiro: Di Livros; 2019.
7. Ellison PM, Zitelli JA, Brodland DG. Mohs micrographic surgery for melanoma: a prospective multicenter study. J Am Acad Dermatol. 2019;81(3):767-74.
8. Mohs FE. The width and depth of the spread of malignant melanomas as observed by a chemosurgeon. Am J Dermatopathol. 1984(1);6 Suppl:123-6.
9. Zitelli JA, Mohs FE, Larson P, Snow S. Mohs micrographic surgery for melanoma. Dermatol Clin. 1989;7(4):833-43.
10. Phan K, Loya A. Mohs micrographic surgery versus wide local excision for melanoma in situ: analysis of a nationwide database. Int J Dermatol. 2019;58(6):697-702.
11. Valentín-Nogueras SM, Brodland DG, Zitelli JA, González-Sepúlveda L, Nazario CM. Mohs micrographic surgery using MART-1 immunostain in the treatment of invasive melanoma and melanoma in situ. Dermatol Surg. 2016;42(6):733-44.
12. Breslow A. Thickness, cross-sectional areas and depth of invasion in the prognosis of cutaneous melanoma. Ann Surg. 1970;172(5):902-8.
13. Instituto Nacional de Câncer - INCA. Câncer de pele melanoma [Internet]. Available from: https://www.gov.br/inca/pt-br/assuntos/cancer/tipos/pele-melanoma
14. Burnett ME, Brodland DG, Zitelli JA. Long-term outcomes of Mohs micrographic surgery for invasive melanoma of the trunk and proximal portion of the extremities. J Am Acad Dermatol. 2021;84(3):661-8.
15. Connolly SM, Baker DR, Coldiron BM, Fazio MJ, Storrs PA, Vidimos AT, et al. AAD/ACMS/ASDSA/ASMS 2012 appropriate use criteria for Mohs micrographic surgery: a report of the American Academy of Dermatology, American College of Mohs Surgery, American Society for Dermatologic Surgery Association, and the American Society for Mohs Surgery. J Am Acad Dermatol. 2012;67(4):531-50.
16. Degesys CA, Powell HB, Hsia LB, Merritt BG. Outcomes for invasive melanomas treated with Mohs micrographic surgery: a retrospective cohort study. Dermatol Surg. 2019;45(2):223-8.
17. Nosrati A, Berliner JG, Goel S, McGuire J, Morhenn V, de Souza JR, et al. Outcomes of melanoma in situ treated with Mohs micrographic surgery compared with wide local excision. JAMA Dermatol. 2017;153(5):436-41.
18. Stigall LE, Brodland DG, Zitelli JA. The use of Mohs micrographic surgery (MMS) for melanoma in situ (MIS) of the trunk and proximal extremities. J Am Acad Dermatol. 2016;75(5):1015-21.
19. Kunishige JH, Doan L, Brodland DG, Zitelli JA. Comparison of surgical margins for lentigo maligna versus melanoma in situ. J Am Acad Dermatol. 2019;81(1):204-12.
20. Namin AW, Oudin EM, Tassone PT, Galloway TLI, Dooley LM, Zitsch RP. 3rd. Treatment of cutaneous melanoma of the head and neck with wide local excision versus Mohs. Laryngoscope. 2021;131(11):2490-6.
21. Demer AM, Hanson JL, Maher IA, Liszewski W. Association of Mohs micrographic surgery vs wide local excision with overall survival outcomes for patients with melanoma of the trunk and extremities. JAMA Dermatol. 2021;157(1):84-9.
22. Viola KV, Rezzadeh KS, Gonsalves L, Patel P, Gross CP, Yoo J, et al. National utilization patterns of Mohs micrographic surgery for invasive melanoma and melanoma in situ. J Am Acad Dermatol. 2015;72(6):1060-5.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}