


Ahmed Fathy State1; Shaymaa ElMongy ElMongy-Mohammed1; Ghada Elsayed Mohamed2
Financial support: none
Conflict of interest: none
How to cite this article: State AF, Mohammed SEE, Mohamed GE. Predictive factors in the treatment of pseudo-acanthosis nigricans by fractional carbon dioxide laser and glycolic acid peel. Surg Cosmet Dermatol. 2023;15:e20230168.
BACKGROUND: Acanthosis nigricans is a common dermatological disorder characterized by hyperpigmented and hyperkeratotic velvety skin lesions. It can be a manifestation of systemic disease.
OBJECTIVE: This study aims to evaluate the clinical and laboratory predictive factors in the treatment of pseudo-acanthosis nigricans.
PATIENTS AND METHODS: This study included 20 patients with pseudo-acanthosis nigricans from the
outpatient clinic. All cases were subjected to fractional CO2 laser on the right side of the neck and glycolic acid peel 70% on the left side of the neck. Each patient was followed up for three and half months.
RESULTS: There was an overall improvement in area index, severity, and texture in the neck of cases with pseudo-acanthosis nigricans treated with fractional CO2 laser or Glycolic acid peel.
CONCLUSION: There was no statistical significance when comparing the effect of laser or peeling on different age groups and obese or overweight cases.
Keywords: Laser therapy; BMI-Age; Skin diseases
Acanthosis nigricans (AN) is described as a dermatological disorder of multiple etiologies, characterized by symmetric, dark, coarse, thickened, velvety appearing plaques commonly distributed on the neck, axillae, antecubital and popliteal fossae, inframammary, and groin areas.1 AN can be a manifestation of systemic disease that is associated with insulin resistance, diabetes mellitus, obesity, internal malignancy, endocrine disorders, and drug reactions.2
It can be classified into four types: benign, malignant, drug-induced, and pseudo-acanthosis nigricans.3
Pseudo-acanthosis nigricans is the most common variant. The term pseudo-acanthosis nigricans was referred to obese individuals who have AN with no underlying endocrinopathies. In these cases, the etiology was attributed to obesity, excessive local friction, and sweat.4
The pathophysiology of AN is a multifactorial stimulation of the proliferation of epidermal keratinocytes and dermal fibroblasts.1
Multiple treatment options are available for the condition. General measures include weight loss and treating underlying diseases, while topical treatments include retinoids, calcipotriol, keratolytics, lasers, chemical peel using trichloroacetic acid, and systemic therapies include retinoids like isotretinoin and insulin sensitizers like metformin.5
Fractional laser can be used in AN due to the mechanism of elimination of thermally damaged keratinocytes and melanin pigment (called microscopic epidermal necrotic debris – MENDs) that leads to new epidermal formation resulting in both decrease in epidermis thickness and melanin pigment in AN.6
GA facilitates corneodesmosome degradation, causing desquamation. GA acidifies the horny cell layer to accelerate the activity of an exfoliative enzyme, cathepsin D, which resides in the granular and horny cell layers and has an optimum pH value of 2–5. GA also enhances long-term de novo synthesis of cathepsin D. These effects promote exfoliation of the corneocytes and decrease the stratum corneum thickness.7
No available studies reported data about predictive factors during AN treatment. However, several studies have identified an association between increased BMI (Body Mass Index) and AN.8 AN patients have a higher risk of developing metabolic syndrome and type 2 diabetes mellitus. Also, a significant correlation is seen between AN and hyperinsulinemia, hyperglycemia, and HOMA-IR.1 Homeostasis model assessment-insulin resistance (HOMA-IR) is a good tool to assess acanthosis nigricans associated with insulin resistance.4
This study aimed to evaluate the clinical and laboratory predictive factors in the treatment of pseudo-acanthosis nigricans through assessing changes in the degree of area index, severity, and texture of lesion after glycolic acid peel 70% and fractional CO2 laser.
The study included 20 patients with pseudo-acanthosis nigricans chosen from the outpatient clinic.
The patients signed the informed consent before inclusion in the study. Every care was taken to protect the data’s privacy. The work has been conducted following The Code of Ethics of the World Medical Association (Declaration of Helsinki) for studies involving humans.
The patients were selected based on the following criteria for inclusion and exclusion:
Inclusion criteria: Patients who have pseudo-acanthosis nigricans of the neck with no underlying endocrinopathies.
Exclusion criteria: Other causes of acanthosis nigricans. Higher susceptibility to post-peel and post-laser risks such as hyperpigmentation or hypopigmentation, scarring, and keloids (known by full history and examination); pregnancy and lactation; systemic diseases as connective tissue disease; diabetes mellitus; and infectious diseases or any other condition that could affect the wound-healing process; systemic retinoids use within six months of study initiation, and/or use of immunosuppressive drugs; patients treated for acanthosis nigricans in the previous three months or less.
• Full history taking focusing on age, disease duration, possible causes, and previous treatment modalities (such as peeling, vitamin A derivatives, or Laser therapy).
• General dermatological examination for any associated skin diseases, and any signs of systemic diseases and obesity assessment through measuring body mass index. Body mass index (BMI) is the ratio of weight to height, calculated as weight (kg)/height (m2) or weight (lb)/height (in2) multiplied by 703. (Normal weight is a BMI between 18.5 and 24.9; overweight is a BMI between 25.0 and 29.9; obesity is a BMI of 30.0 or higher).
• Local examination: 1) Disease severity and texture were evaluated by the scoring system Acanthosis Nigricans Area and Severity Index.9
Location and score Description
Neck severity
0 Absent: not detectable on close inspection
1 Present: clearly present on close visual inspection, not visible to the casual observer, extent or measurable
2 Mild: limited to the base of the skull, does not extend to the lateral margins of the neck (usually <3 inches in breadth)
3 Moderate: extending to the lateral margins of the neck (posterior border of the sternocleidomastoid) (usually 3-6 inches), should not be visible when the participant is viewed from the front.
4 Severe: extending anteriorly (>6 inches), visible when the participant is viewed from the front
Neck texture
0 Smooth to touch: no differentiation from normal skin to palpation
1 Rough to touch: clearly differentiated from normal skin
2 Coarseness can be observed visually; portions of the skin clearly raised above other areas
3 Extremely coarse: "hills and valleys" observable on visual examination
• The area index was calculated by first finding the total area of the side of the neck by multiplying the length (measured from a point at the junction between the chin and upper neck in full neck extension to a point at the inter-clavicular space) by the width (measured from the point at the junction between the chin and upper neck to a point just below the nape hairline). Then the affected area was calculated by multiplying its largest length by its largest width.
• A percentage was then calculated, and a value was chosen according to the table mentioned for area index score: Acanthosis nigricans area index score for assessment of right and left sides of the neck affection.
AREA (A) INDEX
0 1 2 3 4 5
No involvement <10% 10-29% 30-49% 50-69% 70-100%
Score 0 >> no involvement (no lesion found)
Score 1 >> AN lesion less than 10% of total area of side of neck
Score 2 >> AN lesion is from 10% to 29% of total area of side of neck
Score 3 >> AN lesion is from 30% to 49% of total area of side of neck
Score 4 >> AN lesion is from 50% to 69% of total area of side of neck
Score 5 >> AN lesion is from 70% to 100% of total area of side of neck
• Before treatment, patients were asked about their goals, concerns, and expectations to avoid unrealistic anticipations. Possible adverse events were explained such as pain, erythema, and burning.
• Sunscreen was strictly used throughout the treatment.
• All patients received topical retinoic acid and whitening agents 10-14 days before each session to decrease post-inflammatory hyperpigmentation.
• The follow-up visit was performed two months after the last session.
Fractional CO2 laser: On the right side of the neck (laser side), each patient received three sessions of fractional CO2 laser (SmartXide DOT, fractional handpiece, Deka Co, Italy), with a 2-week interval. The parameters were low power (10 J), low density (500μm), short dwell time (500 μs), and double stacking with a single pass on the affected area. A test was performed first on the region to detect adverse events of treatment. Preoperatively, an anesthetic cream was applied to the treatment area, and the neck was degreased with alcohol. Post-operatively, ice packs for cooling were immediately applied after laser sessions, and the patients were advised to apply a topical antibiotic with steroid ointment and emollient after the session.
Glycolic acid (GA) peel: First, the skin was degreased with acetone. The skin was subjected to chemical peel with GA 70% on the left side of the neck. Each patient underwent three sessions with a 2-week interval. A first coat of the peeling was applied, and the frosting was observed. If no frosting was formed, a second coat was applied.
The collected data was revised, coded, tabulated, and introduced to a PC using Statistical Package for Social Science (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.). Data were presented, and suitable analysis was performed according to the type of data obtained for each parameter. The Shapiro test was conducted to test the normality of data distribution, mean and standard deviation (± SD) for parametric numerical data, while median and range for non-parametric numerical data. The Student T-Test was used to assess the statistical significance of the difference between the two study group means.
Regression analysis: linear regression analysis was used to predict risk factors, using generalized linear models. A p-value is considered significant if <0.05 at a confidence interval of 95%.
We conducted a comparative study with 20 patients with pseudo-acanthosis nigricans. All cases were subjected to fractional CO2 laser on the right side of the neck and glycolic acid peel on the left side of the neck. Fifteen patients received three sessions, while five cases improved after two sessions (Figure 1). The follow-up visit was performed two months after the last session.
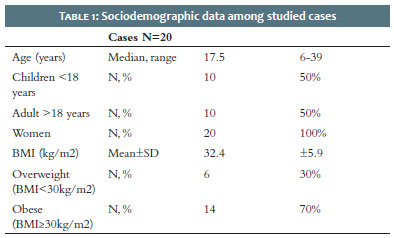
All cases were women with a mean age of 17.5 (ranging from 6 to 39 years), and a mean BMI of 32.4 (70% obese and 30% overweight). The median HOMA-IR was 1, ranging from 0.5 to 3. Median TSH was 2, ranging from 0.8 to 4.9. Median disease duration was 1 year, ranging from 2 months to 4 years.
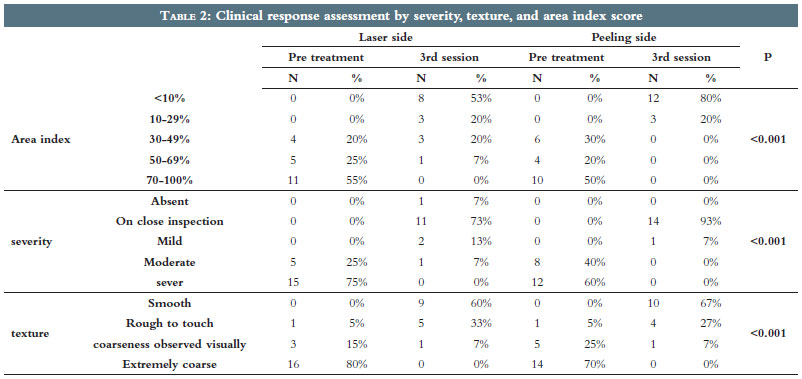
The baseline clinical data were similar but not identical when comparing the right and left sides of the neck (p>0.05 for area index, severity, and texture) (Tables 1 and 2).
There was an overall improvement in area index, severity, and texture across time in individuals subjected to CO2 laser or GA peel (p<0.001).
Note that five cases improved after two sessions and did not require a third one (Table 3).
There was an overall improvement in area index, severity, and texture across time in individuals subjected to CO2 laser or GA peel (p<0.001).
Note that five cases improved after two sessions and did not require a third one.
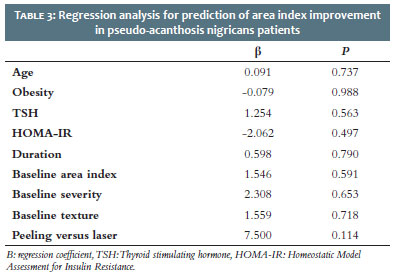
We conducted a linear regression to predict area index improvement using age, obesity, TSH, HOMA-IR, duration of AN, baseline area index, severity, texture, and compared treatment types as confounders. None of these parameters affected the improvement of the area index. Although comparing peeling and laser treatments had no statistically significant impact on area index improvement (p>0.05), peeling had a better effect (β had a positive charge) (Table 4).
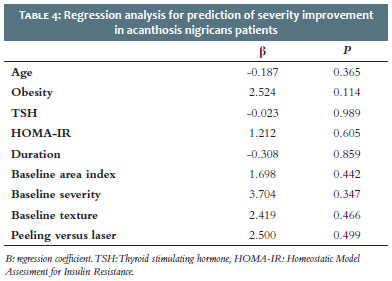
We conducted a linear regression to predict severity improvement using age, obesity, TSH, HOMA-IR, duration of AN, baseline area index, severity, texture, and compared treatment types as confounders. None of these parameters affected the improvement of the severity. Although comparing peeling and laser treatment had no significant impact on severity improvement (p>0.05), peeling had a better effect (β had a positive charge) (Table 5).
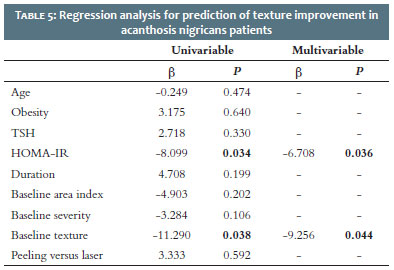
We conducted a linear regression to predict texture improvement using age, obesity, TSH, HOMA-IR, duration of AN, baseline area index, severity, texture, and compared treatment types as confounders. Better baseline texture and lower HOMA-IR were considered a favorable predictor of better texture improvement after laser or peeling treatment in uni- and multivariable analyses.
Although comparing peeling and laser treatment had no statistically significant impact on texture improvement (p>0.05), peeling had a better effect (β had a positive charge) (Table 6).
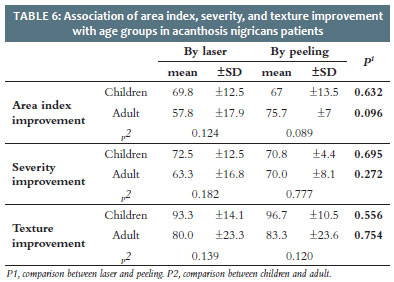
Comparing the effect of laser and peeling on children had no statistically significant differences regarding area index, severity, and texture (p=0.632, p=0.695, p=0.556, respectively).
Comparing the effect of laser and peeling on adults had no statistically significant differences regarding area index, severity, and texture (p=0.096, p=0.272, p=0.754, respectively) (Table 7).
Regarding laser, no statistically significant differences were found between children and adults concerning area index, severity, and texture (p=0.124, p=0.182, p=0.139, respectively).
Regarding peeling, no statistically significant differences were found between children and adults concerning area index, severity, and texture (p=0.089, p=0.777, p=0.120, respectively).
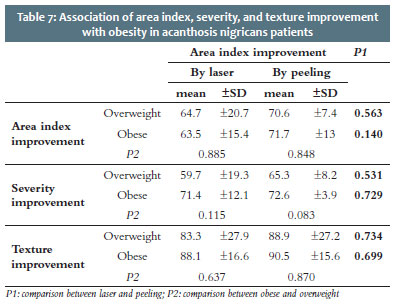
Comparing the effect of laser and peeling on overweight patients, we observed no statistically significant differences regarding area index, severity, and texture (p=0.563, p=0.531, p=0.734, respectively).
Comparing the effect of laser and peeling on obese patients, we observed no statistically significant differences regarding area index, severity, and texture (p=0.140, p=0.729, p=0.699, respectively).
Regarding laser, no statistically significant differences were found between obese and overweight individuals concerning area index, severity, and texture (p=0.885, p=0.115, p=0.637, respectively).
Regarding peeling, no statistically significant differences were found between obese and overweight individuals concerning area index, severity, and texture (p=0.848, p=0.083, p=0.870, respectively).
We conducted a comparative study with 20 patients with pseudo-acanthosis nigricans.
All cases were women and the mean age was 17.5. Half of them were children and the other half were adults. In Zaki et al. study the age ranged from 18 to 40 years with a mean age of 27.5 (±8.10).10 In Leerapongnan et al. study the age ranged from 18 to 60 years and the mean age (±SD) was 28.33 (± 9.92).6
The mean BMI was 32.4 kg/m2, and most of the patients were obese (70%), while 30% were overweight. This finding agrees with Leerapongnan et al. (6) who found that the mean BMI was 29.88 (SD ± 5.17). Body mass index is an important confounding factor in the association of acanthosis nigricans with type 2 diabetes mellitus, which is why it is said that “acanthosis nigricans is not a skin disease per se but a cutaneous sign of an underlying condition or disease”.11
Regarding HOMA-IR, the current study demonstrated that the median HOMA-IR was 1, ranging from 0.5 to 3. HOMA-IR is a widely used and validated tool for quantifying IR in clinical and epidemiological studies on the association of AN and IR among children and young adults.12 Álvarez-Villalobos et al. (13) study shows that homeostasis model assessment of IR values was significantly higher in the AN group than in the control group (3.71 versus 2.5) in cases with fasting plasma glucose below 100 mg/dL. A relationship between AN and IR has been described.12 The role of AN as a precursor to IR and/or obesity should also be considered.13 AN screening may help to identify coexisting comorbidities related to adiposity or patients at high risk.14
There was an overall improvement in area index, severity, and texture across time in patients subjected to a CO2 laser (p<0.001). This finding agrees with the Eldeeb et al.3 study, which reported that fractional CO2 laser markedly improved AN texture and pigmentation.
In contrast to the current findings, in Zaki et al.10 the mean severity SD of the lesion did not improve after using a CO2 laser on the right side of the neck, where the mean Acanthosis Nigricans Area and Severity Index (ANASI) at the start of the study was 23.50 (8.85), decreasing to 19.10 (7.62) after the laser treatment sessions, indicating no statistical improvement (P=0.1). The discrepancies between the current study and the previously mentioned works might be attributed to better patient preparation and selection, as well as different laser machines.
There was an overall improvement in area index, severity, and texture across time in patients subjected to GA peel (p<0.001). In agreement with our result, Zaki et al.10 reported that the mean severity ± SD of the lesion at the start of the study, according to ANASI, was 23.55 (± 8.68), decreasing to 13.50 (± 8.33) after the GA treatment sessions on the left side of the neck. The improvement was statistically significant (P = 0.001). Also, Ichiyama et al.7 study showed the usefulness of GA peel for Japanese familial AN patients with skin type IV.
We found that no recurrence was reported two months after the last session. In agreement with our result, Campos et al.15 observed no recurrence during the 14 months of follow-up. Similarly, there was no sign of recurrence after a 1-year follow-up period (Wijnberg et al.)16On the contrary, Eldeeb et al.3 found that, among the patients who had an excellent response after the laser therapy, 20% had a recurrence of AN lesions during the six months of the follow-up period.
Comparing the effect of CO2 laser and GA peel in different age groups, there was no difference regarding area index, severity, and texture improvement in children or adult cases. Also, comparing the effect of CO2 laser and GA peel on overweight or obese cases, there was no difference regarding area index, severity, and texture improvement. As AN is a common dermatosis in different age groups, it is essential to assess the efficacy and safety when treating the disease.
We conducted a linear regression analysis to predict area index, severity, and texture improvement using age, obesity, TSH, duration, baseline area index, severity, and texture and compared treatment types as confounders. None affected the improvement of area index and severity. However, a better baseline texture and lower HOMA-IR was considered a favorable predictor of better texture improvement after CO2 laser or GA peel treatment. Nonetheless, comparing GA peel and CO2 laser had no significant impact on area index, severity, and texture improvement (p>0.05).
However, the sample size in the current study was small, thus, further research is necessary to confirm if there are predictive factors affecting the prognosis of using fractional CO2 dioxide laser or glycolic acid peel to treat pseudo acanthosis nigricans.
A good history of the onset, course, and other skin symptoms associated with AN is crucial to exclude malignant AN. Also, HOMA-IR is essential in the investigation of AN associated with obesity. Before peeling or laser sessions for AN, it’s important to obtain a good personal and family history to search for a tendency to keloid or hypertrophic scar, PIH, or vitiligo; prepare the skin to enhance the effect of the laser or peeling; test the area before peeling or laser; obtain written consent from all patients.
We recommend further studies on possible predictive factors including baseline clinical data or laboratory investigation to predict outcomes after treatment and predict resistant cases.
Acanthosis nigricans is a common disfiguring dermatological condition. Glycolic acid peel 70% and fractional CO2 laser are considered effective modalities for AN treatment. However, GA peel was more effective, although statically insignificant.
Ahmed Fathy State
Preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Shaymaa ElMongy ElMongy-Mohammed
Study design and planning; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Ghada Elsayed Mohamed
Approval of the final version of the manuscript; active participation in research orientation; critical revision of the manuscript.
1. Das A, Datta D, Kassir M, Wollina U, Galadari H, Lotti T, et al. Acanthosis nigricans: a review. J Cosmet Dermatol. 2020;19(8):1857-65.
2. Patel NU, Roach C, Alinia H, Huang WW, Feldman SR. Current treatment options for acanthosis nigricans. Clin Cosmet Investig Dermatol. 2018;11:407-13.
3. Eldeeb F, Wahid RM, Alakad R. Fractional carbon dioxide laser versus trichloroacetic acid peel in the treatment of pseudo-acanthosis nigricans. J Cosmet Dermatol. 2022;21(1):247-53.
4. Phiske MM. An approach to acanthosis nigricans. Indian Dermatol Online J. 2014;5(3):239-49.
5. Brady MF, Rawla P. Acanthosis Nigricans. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022.
6. Leerapongnan P, Jurairattanaporn N, Kanokrungsee S, Udompataikul M. Comparison of the effectiveness of fractional 1550-nm erbium fiber laser and 0.05% tretinoin cream in the treatment of acanthosis nigricans: a prospective, randomized, controlled trial. Lasers Med Sci. 2020;35(5):1153-8.
7. Ichiyama S, Funasaka Y, Otsuka Y, Takayama R, Kawana S, Saeki H, et al. Effective treatment by glycolic acid peeling for cutaneous manifestation of familial generalized acanthosis nigricans caused by FGFR3 mutation. J Eur Acad Dermatol Venereol. 2016;30(3):442-5.
8. Brickman WJ, Binns HJ, Jovanovic BD, Kolesky S, Mancini AJ, Metzger BE, Pediatric Practice Research Group. Acanthosis nigricans: a common finding in overweight youth. Pediatr Dermatol. 2007;24(6):601-6.
9. Burke JP, Hale DE, Hazuda HP, Stern MP. A quantitative scale of acanthosis nigricans. Diabetes Care. 1999;22(10):1655-9.
10. Zaki NS, Hilal RF, Essam RM. Comparative study using fractional carbon dioxide laser versus glycolic acid peel in treatment of pseudo-acanthosis nigricans. Lasers Med Sci. 2018;33(7):1485-91.
11. Popa ML, Popa AC, Tanase C, Gheorghisan-Galateanu AA. Acanthosis nigricans: to be or not to be afraid. Oncol Lett. 2019;17(5):4133-8.
12. Napolitano M, Megna M, Monfrecola G. Insulin resistance and skin diseases. Scientific World Journal. 2015;2015:479354.
13. Álvarez-Villalobos NA, Rodríguez-Gutiérrez R, González-Saldivar G, Sánchez-García A, Gómez-Flores M, Quintanilla-Sánchez C, et al. Acanthosis nigricans in middle-age adults: a highly prevalent and specific clinical sign of insulin resistance. Int J Clin Pract. 2020;74(3):e13453.
14. Hu Y, Zhu Y, Lian N, Chen M, Bartke A, Yuan R. Metabolic syndrome and skin diseases. Front Endocrinol (Lausanne). 2019;10:788.
15. Campos MA, Varela P, Baptista A, Ferreira EO. Unilateral nevoid acanthosis nigricans treated with CO2 laser. BMJ Case Rep. 2016;2016:bcr2016216073.
16. Wijnberg DS, Deutman HC, Steijlen PM, Spauwen PHM. CO2 laser treatment of benign juvenile acanthosis nigricans. Eur J Plast Surg. 2000;23(4):238–40.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}