


Luana Amaral de Moura; Paulo Sergio Emerich Nogueira; Elton Almeida Lucas; Lucia Martins Diniz; Emilly Neves Souza
Submitted on: 27/05/2022
Approved on: 20/06/2022
Financial support: None
Conflict of interest: None
How to cite this article: Moura LA, Nogueira PSE, Lucas EA, Diniz LM, Souza EN. Basaloid follicular hamartoma. Surg Cosmet Dermatol. 2022;14:e20220152.
Basaloid follicular hamartoma (BFH) is a rare and benign adnexal tumor that resembles basal cell carcinoma (BCC) and may present with different clinical manifestations. A mutation in the PTCH gene, involved in Gorlin-Goltz syndrome, could be associated with the pathogenesis of this neoplasm. We describe the case of a 7-year-old girl with multiple papules on her face.
Keywords: Hamartoma; Carcinoma, Basal cell; Genes, Tumor suppressor.
Basaloid follicular hamartoma (BFH) is a rare benign tumor of hair follicles whose histopathological features can mimic basal cell carcinoma (BCC).1,2 It can be hereditary or acquired and localized or generalized. Generalized hereditary forms are usually associated with systemic manifestations, which vary according to the subtype.1,3
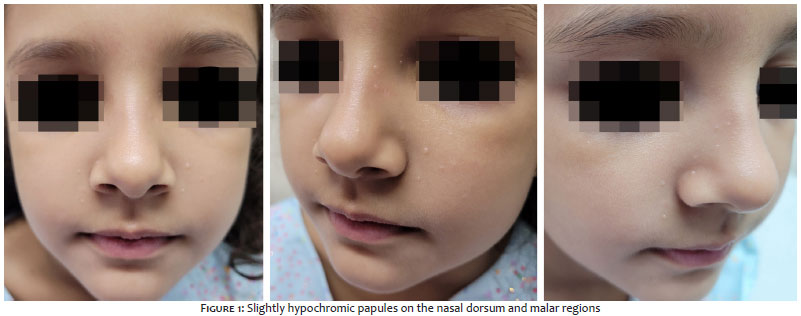
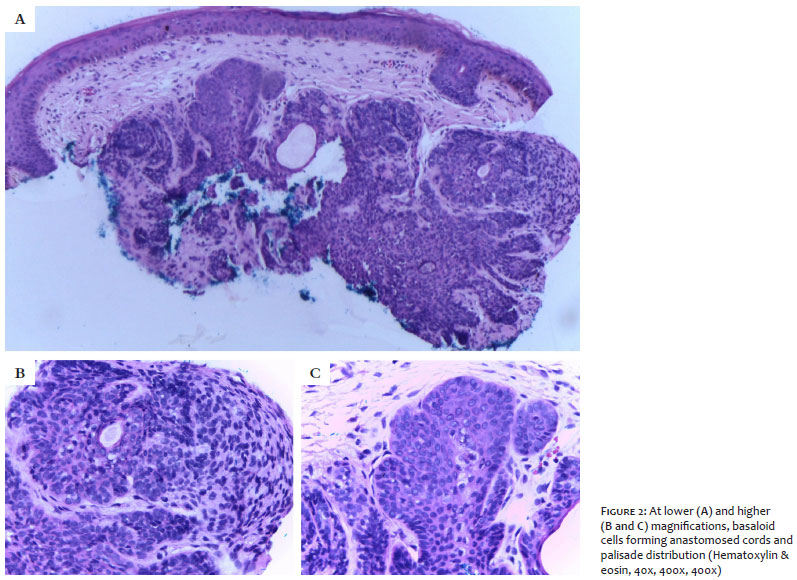
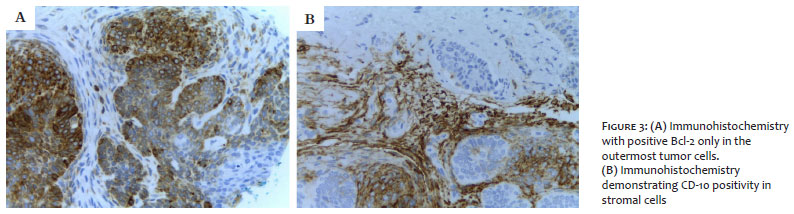
A seven-year-old girl, previously healthy, presented papules in the central region of the face for about a year without associated symptoms. There was no relevant family history. The examination revealed mildly hypochromic papules on the nasal dorsum and malar regions (Figure 1), with no other skin lesions. The diagnostic hypotheses were milia, sebaceous hyperplasia, and syringoma. We performed an incisional biopsy, whose histopathology showed basaloid cells forming anastomosed cords and palisade distribution, initially suggesting nodular basal cell carcinoma (Figure 2). We opted for an anatomopathological review and immunohistochemistry, which showed positive Bcl-2 in the outermost layer of tumor cells, positive CD-10 in the surrounding stromal cells, Ki-67 index (proliferative activity) of 20%, and CD- 34 negative (Figure 3). Thus, we established the diagnosis of basaloid follicular hamartoma. The patient initiated a thorough investigation to rule out associated syndromes.
Although the pathogenesis of BFH is unknown, it is believed that a mutation in the PTCH (protein patched homolog) gene, which encodes a receptor involved in the Sonic hedgehog–Patched–Gli (Shh-Ptch-Gli) signaling pathway, could contribute to the tumor formation. This abnormality would promote an inadequate regulatory function, with constant positive signaling, resulting in atypical and uncontrolled cell division and growth.3-5
The clinical manifestations are varied, but most cases of BFH present with one or multiple papules of 1 mm to 2 mm of normochromic to brownish color on the face, scalp, neck, axilla, trunk, and pubic region.1,5 In this case, the lesions were mildly hypopigmented, multiple, and bilateral.
So far, five clinical forms have been described: (1) Solitary or multiple papules, as in the report; (2) Linear or unilateral localized papule or plaque; (3) Localized plaque with alopecia; (4) Autosomal dominant, generalized familial type, without associated diseases; and (5) Generalized papules associated with myasthenia gravis, alopecia, systemic lupus erythematous, hypotrichosis, and cystic fibrosis.2,3,5
Recently, a retrospective study conducted at the University Hospital of Strasbourg, France, evaluating 17 cases of BFH diagnosed between 1998 and 2017, described a higher incidence of the solitary form, characteristically confused with basal cell carcinoma. It also reported that the unilateral linear form often follows Blaschko’s lines, reflecting cutaneous mosaicism. This clinical variant may be related to the ipsilateral brain, bone, and dental abnormalities. It may also be associated with Happle-Tinschert syndrome.4
Despite the variability of BFH manifestations, the histopathological appearance is remarkably constant. There are cords and extensions of branched basaloid epithelial cells arranged vertically in the superficial and middle dermis, most in connection with the epidermis and hair follicles, as in the case reported. When the palisade organization is present, it is much less marked than the BCC. By definition, cell atypia and mitosis are absent or very rare. Follicular involvement is marked by the vertical arrangement that replaces the normal follicle, lesion with a basophilic periphery and eosinophilic center, and mucin-rich stroma.1,4
Immunohistochemistry is not specific but may aid in the diagnosis. In the stroma, there is positivity for CD-34 and CD-10 (which also stains matrix cells). Tumor cells present an immunoreaction for Bcl-2 restricted to a few cells on the periphery of the islands, as in the report. The Ki-67 index is low. PCNA is not very prominent, and PTCH mRNA is overexpressed in cells in direct contact with the dermis, while CD-10 of tumor cells is negative.2
The primary differential diagnosis of localized BFH is basal cell carcinoma, especially the infundibulum cyst. Contrary to BFH, BCC immunohistochemistry shows negative CD-34 in the stroma, diffusely positive Bcl-2, prominent PCNA, diffusely overexpressed PTCH mRNA, and positive CD-10, with a high Ki-67 index.1,2 In cases of multiple localized lesions, as in the present report, other hypotheses would be adnexal tumors, trichoepitheliomas, sebaceous hyperplasias, syringomas, and sebaceous nevi.
The malignancy potential of BFH is uncertain, although transformation to BCC has been documented. Of the ten transitional cases reported, eight were linear or unilateral localized variants.2 It is believed that the rapid growth or change in the clinical appearance of the lesions could alert about BCC development.2-4 Prophylactic excision is not recommended, especially in multiple presentations.4
There is still no established algorithm for the BFH treatment. The literature describes options, such as surgical excision, cryotherapy, CO2 laser, photodynamic therapy, and imiquimod. We chose expectant management with regular clinical follow-up, considering the age of the reported patient and the existence of multiple lesions on the face. Vismodegib, an inhibitor of the hedgehog signaling pathway, may help to treat severe conditions in the future. The use of 5-aminolevulinic acid (5-ALA) associated with photodynamic therapy is safe, being a possible therapy for children with multiple lesions.1-5
The prognosis of basaloid follicular hamartoma is excellent, with a notable exception for cases associated with the development of BCC or systemic disorders.3
Basaloid follicular hamartoma is a rare benign neoplasm easily confused, clinically and histopathologically, with BCC. We present the case of a seven-year-old girl with multiple papules in the malar region and on the nasal dorsum, whose initial anatomopathological examination suggested BCC. It is crucial to consider the BFH in the presence of multiple nonspecific lesions in the pediatric age group in healthy children. In this case, revisions of the histopathological study and immunohistochemistry were essential for the diagnosis.
Luana Amaral de Moura 0000-0002-3697-0186
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Paulo Sergio Emerich Nogueira 0000-0003-1528-1100
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Elton Almeida Lucas 0000-0002-6524-2030
Statistical analysis; approval of the final version of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Lucia Martins Diniz 0000-0001-8107-8878
Statistical analysis; approval of the final version of the manuscript; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; critical literature review; critical revision of the manuscript.
Emilly Neves Souza 0000-0003-1151-8537
Statistical analysis; approval of the final version of the manuscript study design and planning; preparation and writing of the manuscript; active participation in research orientation; critical literature review; critical revision of the manuscript.
1. Edelman S, Huamani ANT, Centeno MDV, Cervini AB. Basaloid follicular hamartoma associated with follicular mucinosis and inflammation. An Bras Dermatol. 2022;97(1):45-8.
2. Jain S, Khopkar U, Sakhiya J. Localized unilateral basaloid follicular hamartoma along Blaschko's lines on face. Indian J Dermatol Venereol Leprol. 2019;85(1):60-4.
3. Cerejeira A, Gomes N, Pacheco J, Pedrosa A, Baudrier T, Azevedo F. Familial multiple basaloid follicular hamartoma. Dermatol Online J. 2021;27(6):1-4.
4. Hazemann G, Michel C, Mahé A, Lipsker D, Cribier B. Hamartome folliculaire basaloïde: étude anatomoclinique [Histopathological study of basaloid follicular hamartoma]. Ann Dermatol Venereol. 2019;146(3):181-91.
5. Segars K, Cooper H, Hogan DJ, Miller R, Heaphy M Jr, Spencer J. Basaloid follicular hamartoma: a case report and a novel cosmetic treatment. J Clin Aesthet Dermatol. 2018;11(3):39-41.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}