


Amanda Maria Sandes Lemos1; Beatriz Gomes de Castro1; André Luis Oliveira do Nascimento1; Carlos Alberto de Oliveira Rocha1; João Paulo Oliveira de Almeida1; Gustavo Nascimento Monteiro Siqueira1; Myllena Vitória Bispo Santana2; João Vitor Bispo Santana1; Tânia Rita Moreno de Oliveira Fernandes3; Maria Deysiane Porto Araújo1; Thaysa Kelly Barbosa Vieira Tomé1; José Roberto Amorim1; Rodrigo Feliciano do Carmo4,5; Carlos Dornels Freire de Souza1,6
Submitted on: 18/04/2022
Approved on: 10/07/2022
Financial support: None
Conflict of interest: None
How to cite this article: Lemos AMS, Castro BG, Nascimento ALO, Rocha CAO, Almeida JPO, Siqueira GNM, et al. Melanoma mortality in the capitals of Northeast Brazil, 2001-2017: analysis by the regression model by inflection points. Surg Cosmet Dermatol. 2022;14:e20220145.
INTRODUCTION: Melanoma comprises 3% of all skin tumors and can produce metastasis with high mortality.
OBJECTIVE: To analyze the temporal behavior of mortality from skin melanoma in the capitals of Northeast Brazil from 2001 to 2017.
METHODS: We conducted an ecological time series study involving all deaths due to melanoma registered in the capitals of the Northeast region of Brazil from 2001 to 2017. Crude and standardized rates by the world and Brazilian populations were analyzed. We obtained the indicators from the National Cancer Institute (INCA). The regression model by inflection points was used in the statistical analysis, calculating the annual variation and the average annual variation percentages.
RESULTS: There were 954 deaths from melanoma. The three rates analyzed showed a linear growth trend over the time series: proportional mortality increased from 2.1% to 8.28% (AAPC 6.0%; p<0.02), the crude mortality grew from 0.22 to 0.64/100 thousand (AAPC 5.0%; p<0.01) and the mortality adjusted by the world population in the capitals of the Northeast rose from 0.28 to 0.61/100 thousand (AAPC 2.7%; p<0.01).
CONCLUSION: Mortality from melanoma grew in the Northeastern capitals, with inequality between the sexes and according to the capitals.
Keywords: Epidemiology; Melanoma; Mortality; Skin neoplasms.
The progressive increase in chronic degenerative diseases, such as cancer, to the detriment of infectious and parasitic diseases highlights the changes in the Brazilian morbidity and mortality profile.1 Skin cancer is the most frequent neoplasm in Brazil, with about 190,000 annual records and four thousand deaths.2
Skin cancer is classified into melanoma and non-melanoma.3 Non-melanoma skin cancer is the most frequent, corresponding to 30% of all neoplasms in Brazil,3 with an estimated 176 thousand cases in 2020.3,4 Melanoma skin cancer is rarer and comprises 3% of all skin tumors, with an estimated 8,000 cases in 2020.2
Melanoma originates from the cells responsible for producing melanin, the melanocytes, found mainly in the skin and also in many other body regions where these cells migrate during embryonic development from the neural crest pluripotent stem cells.5 Thus, although the largest number of cases of melanoma is cutaneous,2,6 it may also appear in the different places where melanocytes are present, such as mucosa,7 meninges,8,9 and eyes.10
Despite the low incidence, cutaneous melanoma has greater malignancy and the ability to produce metastasis, a disordered proliferation of abnormal cells with a tendency to autonomy and durability. These cells can invade other organic structures via hematogenous or lymphatic pathways, producing deleterious effects in other organs.2,4
However, the prognosis is good when melanoma skin cancer is detected at an early stage, without metastasis. The five-year survival rate after diagnosis for cutaneous melanoma without metastasis is 99%, while for cutaneous melanoma with metastasis to regional lymph nodes is 65%. For cutaneous melanoma with metastasis, the distance is 25%.11
In a country of continental dimensions such as Brazil, where inequalities prevail (economic, environmental, and access to Health Services), it is also noted that epidemiological data differ among regions. In 2020, 8,450 melanoma skin cancer records were estimated. Of these, 1,000 cases (12.8%) are expected for the Northeast,2 even though this region is responsible for 26.7% of the Brazilian population. Unlike the South and Southeast regions, which concentrate scientific and health centers, in the Northeast, investigations on the prevalence and temporal trends are scarce.12
This study aims to analyze the temporal behavior of mortality from melanoma in the capitals of Northeast Brazil from 2001 to 2017.
Ecological time series study involving all deaths due to melanoma registered in the capitals of the Northeast region of Brazil from 2001 to 2017.
The study was conducted in all nine capitals of the Northeast region of Brazil: São Luís (Maranhão), Teresina (Piauí), Fortaleza (Ceará), Natal (Rio Grande do Norte), João Pessoa (Paraíba), Recife (Pernambuco), Maceió (Alagoas), Aracaju (Sergipe), and Salvador (Bahia).
The Northeast region has a predominantly tropical and semi-arid climate.13,14 Also, it has the highest solar irradiation rate in Brazil, with an average total daily value of horizontal global irradiation of 5.49 kWh/m2.15 Highlighting the capitals, the average annual temperature is 27.1ºC.14
This study included only the capitals, considering the homogeneity of health scenarios; the fact that the capitals concentrate diagnosis and treatment centers for the most complex diseases; and similar environmental and climatic conditions.14
The following indicators were analyzed:
• Proportional mortality from melanoma;
• Crude melanoma mortality rate; and
• World population-adjusted melanoma mortality rate.
Rates were stratified by sex. Data were obtained from the online Mortality Atlas of the National Cancer Institute José Alencar Gomes da Silva (Instituto Nacional de Câncer José Alencar Gomes da Silva - INCA).16 The document was accessed on March 30, 2020. It’s noteworthy that the rates obtained were already calculated by the INCA platform.
After data collection, statistical treatment was performed using the joinpoint regression model. The model tests whether a line with multiple segments is statistically more adequate to describe the temporal evolution of a set when compared to a straight line or with fewer segments.17 Based on the line inclination, trends were classified as increasing, decreasing, or stationary. Also, the annual percent change (APC) and the average annual percent change (AAPC) were obtained considering a 95% confidence interval (95% CI) and 5% significance. The analysis was performed using the joinpoint regression software (version 4.5.0.1, National Center Institute, Bethesda, MD, USA).
The study did not require approval from the ethics committee since it used secondary data in the public domain and there was no individual identification of any patient.
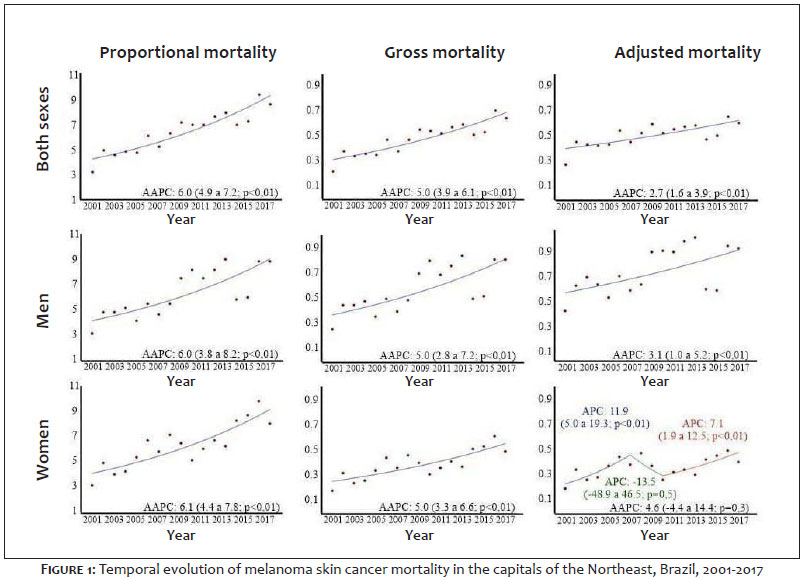
From 2001 to 2017, 954 deaths from melanoma were recorded in the capitals of Northeast Brazil. Of these, 57.02% (n=544) were women. Fortaleza (CE) and Salvador (BA) concentrated 23.48% (n=224) and 19.81% (n=189) of the records, respectively. Considering both sexes, the three rates analyzed (proportional mortality, crude rate, and adjusted rate) showed a linear growth trend over the time series: proportional mortality increased from 4.9% to 7.2% (AAPC 6.0%; p<0.01); crude mortality grew from 3.9% to 6.1% (AAPC 5.0%; p<0.01); and world population-adjusted mortality in capital cities in the Northeast rose from 1.6% to 3.9% (AAPC 2.7%; p<0.01) (Figure 1).
In men, the same temporal growth behavior was observed: proportional mortality increased from 3.8% to 8.2% (AAPC 6.0%; p<0.01); the crude rate rose from 2.8% to 7.2% (AAPC 5.0%; p<0.01); and world population-adjusted mortality rate grew from 1.0% to 5.2% (AAPC 3.1%; p<0.01). In women, proportional mortality showed a linear increase, rising from 4.4% to 7.8% (AAPC 6.1%; p<0.01); the crude rate, also with a linear growth trend, grew from 3.3% to 6.6% (AAPC 5.0; p<0.01); and a stationary pattern was observed in the world population-adjusted rate when considering the total period (2001-2017). In this rate, we observed two inflections and three trends, the last one with significant growth from 2010 (AAPC 4.6%; p<0.01) (Figure 1).
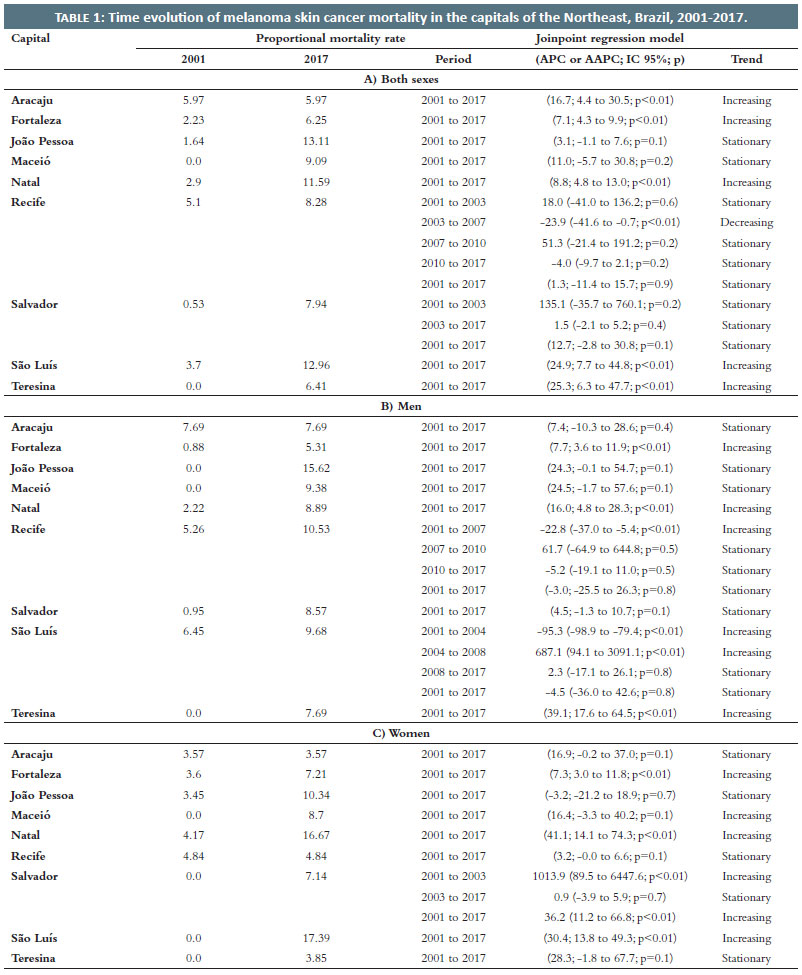
Among the capitals of the Northeast, considering both sexes, five cities showed an increasing temporal trend in the proportional mortality rate: Aracaju (APC 16.7; p<0.01), Fortaleza (APC 7.1; p<0.01), Natal (APC 8.8; p<0.01), São Luís (APC 24.9; p<0.01), and Teresina (APC 25.3; p<0.01). João Pessoa (APC 3.1; p=0.1) and Maceió (APC 11.0; p=0.2) showed stationary trends. Recife and Salvador presented different trends over the years, with a predominant stationary behavior (Table 1).
In men, three capitals showed an increasing temporal trend in the proportional mortality rate for melanoma skin cancer: Fortaleza (APC 7.7; p<0.01), Natal (APC 16.0; p<0.01), and Teresina (APC 39.1; p<0.01). Aracaju (APC 7.4; p=0.4), João Pessoa (APC 24.3; p=0.1), Maceió (APC 24.5; p=0.1), and Salvador showed stationary trends. (APC 4.5; p=0.1). Recife and São Luís presented differences between trends over the years, with a predominance of a stationary trend (Table 1).
In women, five capitals showed an increasing temporal trend in the proportional mortality rate for melanoma: Fortaleza (APC 7.3; p<0.01), Maceió (APC 16.4; p=0.1), Natal (APC 41.1; p<0.01), São Luís (APC 30.4; p<0.01), and Salvador (APC 36.2; p<0.01). The latter, however, showed an increasing trend from 2001 to 2003 (APC 1013.9; p<0.01) and stationary from 2003 to 2017 (APC 0.9; p=0.7). Aracaju (APC 16.9; p=0.1), João Pessoa (APC -3.2; p=0.7), Recife (APC 3.2; p=0.1), and Teresina (APC 28.3; p=0.1) showed a stationary trend (Table 1).
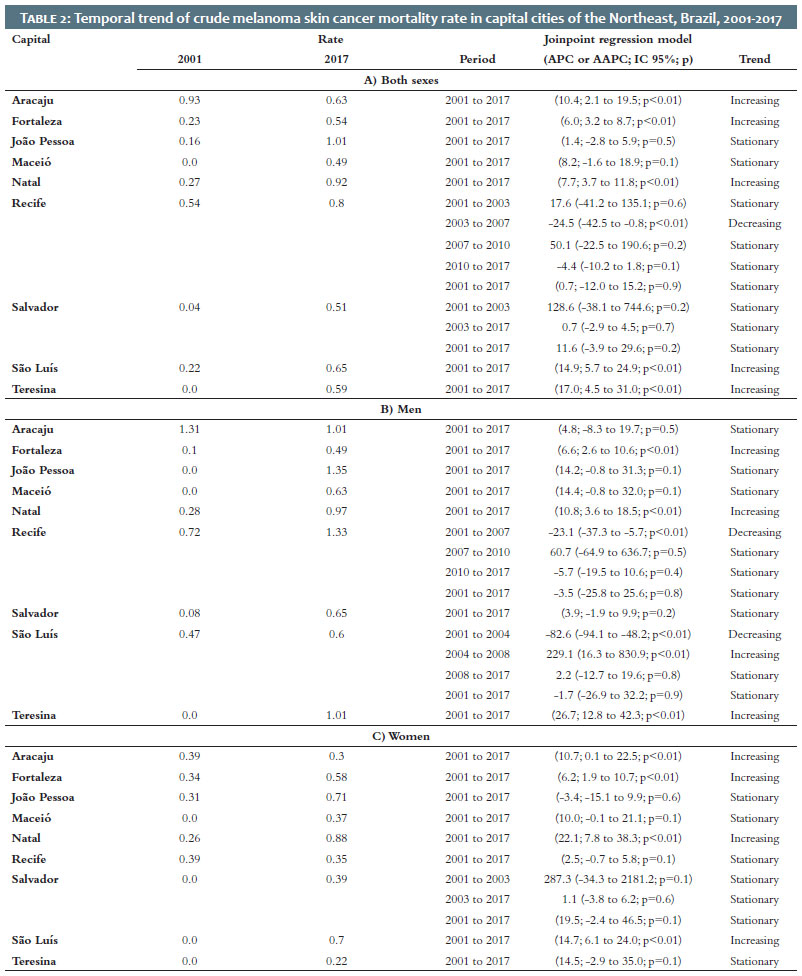
In the analysis of the temporal trend of the crude mortality rate from melanoma skin cancer, considering both sexes, five capitals in the Northeast showed an increasing tendency: Aracaju (APC 10.4; p<0.01), Fortaleza (APC 6.0; p<0.01), Natal (APC 7.7; p<0.01), São Luís (APC 14.9; p<0.01), and Teresina (APC 17.0; p<0 .01). João Pessoa (APC 1.4; p=0.5) and Maceió (APC 8.2; p=0.1) presented a stationary trend. Recife and Salvador showed different tendencies during the period, with a prevalence of a stationary pattern (APC 0.7; p=0.9 and APC 11.6; p=0.2, respectively) (Table 2).
When considering men, Fortaleza (APC 6.6; p<0.01), Natal (APC 10.8; p<0.01), and Teresina (APC 26.7; p<0.01) showed an increasing trend. Aracaju (APC 4.8; p=0.5), João Pessoa (APC 14.2; p=0.1), Maceió (APC 14.4; p=0.1), and Salvador (APC 3.9; p=0.2) presented a stationary trend. There were different trends for Recife (APC -3.5; p=0.8) and São Luís (APC -1.7; p=0.9), but both with a predominance of a stationary pattern (Table 2).
In women, there was an increasing trend in Aracaju (APC 10.7; p<0.01), Fortaleza (APC 6.2; p<0.01), Natal (APC 22.1; p<0.01), and São Luís (APC 14.7; p<0.01). João Pessoa (APC -3.4; p=0.6), Maceió (APC 10.0; p=0.1), Recife (APC 2.5; p=0.1), and Teresina (APC 14.5; p=0.1) showed a stationary trend. Salvador presented variation during the period, with a predominance of a stationary pattern (APC 19.5; p=0.1) (Table 2).
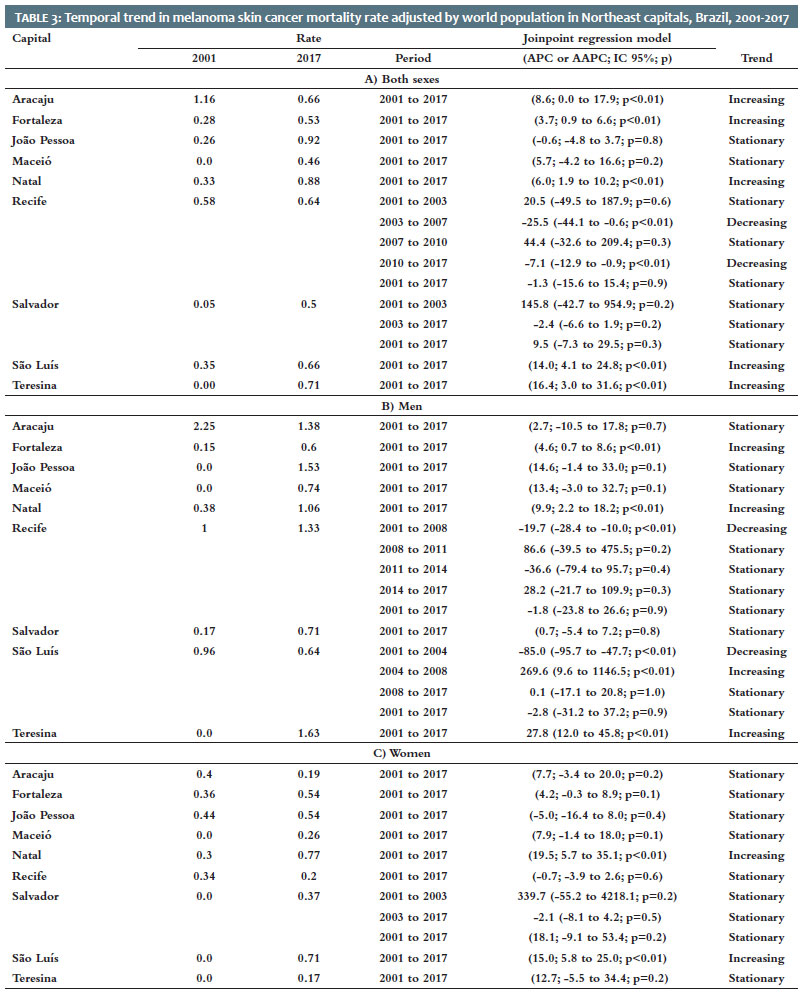
The temporal trend of world population-adjusted mortality rate in the capitals of the Northeast, considering both sexes, was increasing for five cities: Aracaju (APC 8.6; p<0.01), Fortaleza (APC 3.7; p<0.01), Natal (APC 6.0; p<0.01), São Luís (APC 14.0; p<0.01), and Teresina (APC 16.4; p< 0.01). There was a difference between trends from 2001 to 2017 in Recife (APC -1.3; p=0.9) and Salvador (APC 9.5; p=0.3), both with a stationary predominance. There was also a stationary pattern in the cities of João Pessoa (APC -0.6; p=0.8) and Maceió (APC 5.7; p=0.2) (Table 3).
In men, the temporal trend of the adjusted mortality rate increased in three capitals in the Northeast: Fortaleza (APC 4.6; p<0.01), Natal (APC 9.9; p<0.01), and Teresina (APC 27.8; p<0.01). The trend was predominantly stationary in Aracaju (APC 2.7; p=0.7), João Pessoa (APC 14.6; p=0.1), Maceió (APC 13.4; p=0.1), Recife (APC -1.8; p=0.9), Salvador (APC 0.7; p=0.8), and São Luís (APC -2.8; p=0.9) (Table 3).
In women, the temporal trend of the adjusted mortality rate increased in two cities: Natal (APC 19.5; p<0.01) and São Luís (APC 15.0; p<0.01). The trend was stationary in Aracaju (APC 7.7; p=0.2), Fortaleza (APC 4.2; p=0.1), João Pessoa (APC -5.0; p=0.4), Maceió (APC 7.9; p=0.1), Recife (APC -0.7; p=0.6), Teresina (APC 12.7; p=0.2), and Salvador (APC 18.1; p=0.2) (Table 3).
This study aimed to analyze the trend in mortality from melanoma, allowing us to observe a predominance of an increasing tendency in proportional, crude, and adjusted mortality rates in the capitals of Northeast Brazil between 2001 and 2017, especially in Natal and Fortaleza, with inequalities regarding sex and among the capitals.
International epidemiological data indicate a continuous growth in the incidence of melanoma in Europe, Canada, and the United States in recent decades. The highest incidence rate is in New Zealand, with 50 cases per 100,000 inhabitants.18 In the United States, United Kingdom, Sweden, and Norway, rates rise by more than 3% per year, and projections estimate that this increase will continue until at least 2022.19 In the United States, there are almost 7,000 annual deaths due to melanoma.11 This growth is in line with what we observed in our study regarding the world population-adjusted rate, whose annual growth percentage was 2.7%. On the other hand, the annual increase in proportional mortality reached 6.0%.
Melanoma is a disease with multifactorial etiology. However, it is estimated that at least 80% of cases are due to exposure to the sun, which is the primary risk factor for developing the disease.20 In this context, the intensity of solar radiation in the Northeast region may represent a risk factor for the disease.
Excessive and cumulative sun exposure in the first 20 years of age and the number of sunburns throughout life increase the chances of developing melanoma skin cancer in adulthood.20 Childhood, in particular, is a phase more vulnerable to the sun’s harmful effects because children spend more time outdoors and exposed to sunlight. Also, approximately 25% to 50% of all sunlight exposure during a lifetime occurs before the age of 21.20
Furthermore, individuals who perform work activities subject to this exposure are more likely to develop photobiological skin reactions that lead to the emergence of skin cancer. Although there is incisive legislation on the use of personal protective equipment (PPE), there is none requiring sunscreen, which would be beneficial for specific skin areas where PPE does not provide the desired protection. 21
International studies indicate that another significant factor for a future increase in skin cancer cases is life expectancy growth. By 2050, it is expected that up to 32% of the world population will be over 60 years, contributing to the progression in numbers, given the increased skin cancer cases due to growing age.18 This increase is because a longer life span means a longer time of photodamage to skin cells and, mainly, more time for the damage to manifest itself in the form of neoplasms.22
A study conducted in Teresina, the capital of the state of Piauí, showed that most of the cutaneous melanoma diagnoses performed at the referral service were in patients over 50 years. The lesion was found predominantly in chronically photoexposed areas, such as the head and neck, trunk – especially in men – and limbs.12
Melanoma also shows high variation in its incidence in different ethnic groups, mainly due to the photoprotective property of melanin, which is reduced in certain ethnicities.23 North American studies indicate that the risk for developing melanoma during life is 2.6% for whites, 0.6% for Hispanics, and 0.1% for blacks.24 The states of the capitals with a significant increasing trend in the rates analyzed, Natal and Fortaleza, had, according to the last IBGE Demographic Census, 41.2% and 32% self-declared white, respectively.25
The adjusted mortality rates analysis demonstrated stationary predominance for both sexes. However, proportional and crude mortality rates showed a predominance of increasing trends for women and stationary for men. In the adjusted mortality rate the opposite was observed – more increasing trends for men (three capitals - Fortaleza, Natal, and Teresina) than for women (two capitals - Natal and Teresina). In general, men use Health Services less than women. The reasons revolve around the difference in the health needs profile, the search for these services between genders, and the existence of more public health policies aimed at the female population.26,27
Early diagnosis is still the most effective way to reduce mortality from melanoma.12 The early discovery of skin lesions by neoplastic melanocytes still restricted to the epidermis or superficial dermis provides a greater possibility of cure through adequate treatment.27 In recent decades, an improvement in five-year survival was observed with a decrease in the overall mortality rate between 70% and 80% due to early diagnosis and treatment.28
The Brazilian Society of Dermatology (Sociedade Brasileira de Dermatologia - SBD) started, in 2014, the national skin cancer prevention campaign called “Orange December”. Among other educational actions, the campaign warns about the dangers of unprotected sun exposure. Also, SBD conducted 26,161 consultations in 2018, identifying 3,852 cases of skin cancer, including 363 melanomas, in an early detection campaign implemented since 1999.29
The present study, although considering all the necessary methodological precautions, has limitations. The first concerns the use of secondary data, which is influenced by the operational context of surveillance services in the states of the region, with consequent underdiagnosis of the disease and underreporting of deaths (there were capitals with zero cases in certain years, such as Maceió and Teresina in 2001). The second refers to the lack of standardization in data centralization and collection, making it difficult to conduct investigations and comparisons between regions. The third comprises the scarcity of epidemiological studies on the subject.
The analysis of the time series of mortality from melanoma in the capitals of the Northeast region of Brazil between 2001 and 2017 showed an increasing trend for crude mortality, proportional mortality, and adjusted mortality rates considering both sexes in five capitals: Aracaju, Fortaleza, Natal, São Luís, and Teresina. In men, Fortaleza, Natal, and Teresina showed a growing trend in the three rates. In women, we observed a variation according to the rate: five capitals in proportional mortality, four in the crude rate, and two in the adjusted rate.
The results found can have significant value in understanding the health scenario of the region, and they can support the development of prevention and early diagnosis strategies aimed at the regional reality of the Brazilian Northeast and, in particular, its capitals.
Amanda Maria Sandes Lemos 0000-0002-0655-4093
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Beatriz Gomes de Castro 0000-0002-7547-1240
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
André Luis Oliveira do Nascimento 0000-0001-5274-3277
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Carlos Alberto de Oliveira Rocha 0000-0003-2927-5043
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
João Paulo Oliveira de Almeida 0000-0002-0414-4744
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Gustavo Nascimento Monteiro Siqueira 0000-0002-3966-2488
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Myllena Vitória Bispo Santana 0000-0001-8090-0911
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
João Vitor Bispo Santana 0000-0002-5642-1643
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Tânia Rita Moreno de Oliveira Fernandes 0000-0002-7061-2825
Approval of the final version of the manuscript; active participation in research orientation; critical literature review; critical revision of the manuscript.
Maria Deysiane Porto Araújo 0000-0002-1258-0845
Approval of the final version of the manuscript; active participation in research orientation; critical literature review; critical revision of the manuscript.
Thaysa Kelly Barbosa Vieira Tomé 0000-0001-5538-3772
Approval of the final version of the manuscript; active participation in research orientation; critical literature review; critical revision of the manuscript.
José Roberto Amorim 0000-0001-5884-639X
Approval of the final version of the manuscript; active participation in research orientation; critical literature review; critical revision of the manuscript.
Rodrigo Feliciano do Carmo 0000-0001-9601-6995
Approval of the final version of the manuscript; preparation and writing of the manuscript; active participation in research orientation; critical literature review; critical revision of the manuscript.
Carlos Dornels Freire de Souza 0000-0001-7995-1893
Statistical analysis; approval of the final version of the manuscript; study design and planning; active participation in research orientation; critical literature review; critical revision of the manuscript.
1. Fonseca D. Morbimortalidade no Brasil. Cad Saúde Colet. 2015;23(1):1.
2. NCA. Estimativa 2020: incidência de câncer no Brasil. Rio de Janeiro: Ministério da Saúde; 2019. Available from: https://www.inca.gov.br/publicacoes/livros/estimativa-2020-incidencia-de-cancer-no-brasil.
3. INCA. Câncer de pele não melanoma. Rio de Janeiro: Ministério da Saúde; 2020. [Cited 2022 Apr 5]. Available from: https://www.inca.gov.br/tipos-de-cancer/cancer-de-pele-nao-melanoma/profissional-de-saude
4. Prati WJ, Silva FC. Levantamento demográfico e epidemiológico do câncer de pele no Estado de Rondônia. Braz J Surg Clin Res. 2018;24(1):13–6.
5. Ali Z, Yousaf N, Larkin J. Melanoma epidemiology, biology and prognosis. EJC Suppl. 2013;11(2):81-91.
6. Azulay RD, Azulay DB, Azulay-Abulafia L. Dermatologia. 7th ed. Rio de Janeiro: Guanabara Koogan; 2017.
7. esus, AMA. Melanoma primário oral: uma revisão da etiopatogenia, clínica e diagnóstico diferencial [dissertation]. Lisboa: Universidade de Lisboa; 2021.
8. Burgos R, Cardona AF, Santoyo N, Ruiz-Patiño A, Cure-Casilimas J, Rojas L, et al. Case report: differential genomics and evolution of a meningeal melanoma treated with ipilimumab and nivolumab. Front Oncol. 2022;11:691017.
9. Lang-Orsini M, Wu J, Heilman CB, Kravtsova A, Weinstein, G, Madan Net, et al. Primary meningeal melanoma masquerading as neurofibromatosis type 2: illustrative case. Journal of Neurosurgery: Case Lessons. 2021; 2(20).
10. Jonas RA, Rokohl AC, Heindl LM. Targeted therapy for malignant ocular melanomas. Ann Eye Sci. 2021;6:1-7.
11. American Cancer Society. Survival rates for melanoma skin cancer. Atlanta: ACS, 2020 [Cited 2022 Apr 5]. Available from: https://www.cancer.org/cancer/melanoma-skin-cancer/detection-diagnosis-staging/survival-rates-for-melanoma-skin-cancer-by-stage.html
12. Vilanova CM, Lages RB, Ribeiro SM, Almeida IP, Santos LG, Vieira SC. Epidemiological and histopathological profile of cutaneous melanoma at a center in northeastern Brazil from 2000 to 2010. An Bras Dermatol. 2013;88(4):545-53.
13. IBGE. Mapa de clima do Brasil. Rio de Janeiro; 2002 [Cited 2022 Apr 5]. Available from: https://www.terrabrasilis.org.br/ecotecadigital/pdf/mapa-de-clima-do-brasil-ibge.pdf
14. EMBRAPA. Boletim de Pesquisa e Desenvolvimento. Recife: Embrapa solos; 2012.
15. Pereira E, Martins F, Gonçalves A, Costa R, Lima F, Rüther R, et al. Atlas brasileiro de energia solar. São José dos Campos: INPE; 2017.
16. INCA. Atlas on-line de mortalidade. Rio de Janeiro, Ministério da Saúde; 2019 [Cited 2020 Mar 30]. Available from: https://mortalidade.inca.gov.br/MortalidadeWeb/pages/Modelo10/consultar.xhtml#panel
17. Kim H-J, Fay MP, Feuer EJ, Midthune DN. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med. 2000;19(3):335–51.
18. Apalla Z, Lallas A, Sotiriou E, Lazaridou E, Ioannides D. Epidemiological trends in skin cancer. Dermatol Pract Concept. 2017;7(2):1-6.
19. Whiteman DC, Green AC, Olsen CM. The growing burden of invasive melanoma: projections of incidence rates and numbers of new cases in six susceptible populations through 2031. J Invest Dermatol. 2016;136(6):1161–71.
20. Criado PR, Melo JN, Oliveira ZNP. Topical photoprotection in childhood and adolescence. J Pediatr. 2012;88(3):203–10.
21. Hayashide J, Minnicelli R, Oliveira O, Sumita J, Suzuki N, Zambianco C, et al. Doenças de pele entre trabalhadores rurais expostos a radiação solar. Estudo integrado entre as áreas de Medicina do trabalho e Dermatologia. Rev Bras Med Trab. 2010;8(2):98-104.
22. American Cancer Society. Cancer Facts & Figures 2020. Atlanta: ACS; 2020 [Cited 2022 Apr 5]. Available from: https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2020.html
23. Ward WH, Farma JM. Cutaneous melanoma: etiology and therapy [Internet]. Brisbane: Codon Publications; 2017. Available from: https://www.ncbi.nlm.nih.gov/books/NBK481860/pdf/Bookshelf_NBK481860.pdf
24. American Cancer Society. Key statistics for melanoma skin cancer. Atlanta: ACS; 2020 [Cited 2022 Apr 5]. Available from: https://www.cancer.org/cancer/melanoma-skin-cancer/about/key-statistics.html
25. IBGE. Censo demográfico 2010. Rio de Janeiro: IBGE; 2011 [Cited 2022 Apr 5]. Available from: https://censo2010.ibge.gov.br/
26. Pinheiro RS, Viacava F, Travassos C, Brito AS. Gênero, morbidade, acesso e utilização de serviços de saúde no Brasil. Ciênc Saúde Colet. 2002;7(4):687–707.
27. Silva CTX, Saddi VA, Arruda JT, Silva KSF, Guillo LA. Prognostic factors and survival of patients with primary cutaneous melanoma. Braz J Hea Rev. 2019;2(6):5241–60.
28. Guidetti MV, Morais GDCG, Rezende LF. Incidência e importância do diagnóstico precoce de melanoma no Brasil. Rev Bras Multidiscip. 2016;19(1):147-154.
29. ociedade Brasileira de Dermatologia. Sociedade Brasileira de Dermatologia oferecerá exames preventivos de câncer da pele no próximo sábado (7/12). Rio de Janeiro: SBD; 2019 [Cited 2022 Apr 5]. Available from: https://www.sbd.org.br/sociedade-brasileira-de-dermatologia-oferecera-exames-preventivos-de-cancer-da-pele-no-proximo-sabado-7-12/
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}