


Estele Yumi Odo Toledo de Barros1; Letícia Megumi Odo1,2; Marina Emiko Yagima Odo1
Financial support: None
Conflict of interest: None
Acknowledgment: We thank the Odo Clinics staff
How to cite this article: Barros EYOT, Odo LM, Odo MEY. Previous fat grafting and hair transplantation using the FUE technique on scalp scars: Update. Surg Cosmet Dermatol. 2022;14:e20220034.
We developed a narrative literature review on the association of fat grafting and hair transplantation using the Follicular Unit Extraction (FUE) technique in scalp scars. Data were collected from studies found in Medline, Lilacs, and IBECS databases. Bibliographical records of several authors who researched mesenchymal cells in adipose tissue were cited, describing the techniques used. The conclusion was that the two-stage hair transplantation technique, with previous fat transplantation, is effective, according to the reviewed articles.
Keywords: Stem Cells; Mesenchymal Stromal Cells; Adipose Tissue; Hair transplantation
“The Fascinating History of Fat Grafting”, by Mazzola and Mazzola,1 reports the origin of fat grafting, in 1893, when the physician Neuber transplanted adipose tissue from an arm to the orbit to correct a depressed and adherent scar, a sequela of osteomyelitis. Soon after, another surgeon removed a lipoma and filled in the space after removing fibrocystic mastitis nodules. Still in the 19th century, filling with paraffin – discovered by a German chemist – began to be performed. The filler was mixed with Vaseline or olive oil. The disastrous consequences soon appeared: there was the formation of large edemas, difficult to remove, and the paraffinoma infiltrated until resulting in pulmonary embolism and other infections. In 1926, another surgeon, Hollander, observed that grafted fat resulted in a high reabsorption rate. Thus, he mixed the patient’s fat with mutton fat: he heated it until a fluid point and then injected it with a syringe. At first, the patient felt severe pain for two or three days. In Chicago (USA), Miller used gutta-percha and crumb rubber, recommending fat for saddle lips and nose.
The history of hair transplantation began in 1822 when Dieffenbach2 described transplantation in birds. Only in 1959 Norman Orentreich,3 considered the “father of hair transplantation”, applied the technique in humans, using 4 mm punches. In 1998, Barrera4 described the attempt to graft fat in scars after burns. Scleroderma, post-traumatic and post-surgical scars treatment followed. Barrera interprets that micro and mini-hair grafts present lower metabolic needs and that mesenchymal stem cells derived from adipose tissue are comparable to bone marrow cells.
This review aims to assess the current knowledge about fat grafting in scalp scars and describe hair transplantation using the Follicular Unit Extraction (FUE) technique since fat grafting performed before hair transplantation can provide better graft survival. The World Congress for Hair Research (WCHR) participants already foresee the significant progress of this technique, such as stem cells and hair cloning, starting from the principle that hair transplantation offers predictable and long-lasting results. Some authors, such as Epstein,5 use this graft even on the scalp without signs of scarring, as in the case of early androgenetic alopecia.
We consulted existing articles on fat grafting on Medline, with 8294 published papers; in Lilacs, with 42; and in IBECS, with 40. About hair transplantation, 1202 publications were consulted in Medline, 24 in Lilacs, and 19 in IBECS.
The stem cells that Kinnaird et al. found among adipose cells were matched to those in the bone marrow.6 In 2019, Obara7 described pluripotent cells with the potential to differentiate into multilineage in the hair follicle.
In 2004, Kinnaird et al. demonstrated that the bone marrow has stromal cells that release cytokines such as Vascular Endothelial Growth Factor (VEGF) and Basic Fibroblastic Growth Factor (bFGF), stimulating new vessels or remodeling existing ones. Normal human mesenchymal cells were cultured under normal O2 and hypoxic conditions for 72 hours. The wide genetic range was confirmed using Elisa and Immunoblot assays. Mesenchymal Stem Cells-Conditioned Media (MSC-CM) is now called Adipose-Derived Stem Cells-Conditioned Media (ADSC-CM), promoting the proliferation and migration of endothelial cells “in vitro”. Anti-VEGF and anti-FGF antibodies attenuate these effects.
Pesce and Scholer8 described, in 2001, the origin of stem cells Oct4 and Nanog (transcription factors), which are inside bulge cells and also in embryonic stem cells. The bulge produces cytokines - growth factors necessary for stem cell activity, such as FGF, Platelet-Derived Growth Factor (PDGF), Bone Morphogenic Protein (BMP), and VEGF. All of them need a cytokine originating from the neural crest described by Tanimura.9 Epidermal stem cells are also present in the sub-bulge region to complete differentiation into a hair follicle.
Authors such as Fukuoka et al.10,11 and Shin12 used the ADSC protein solution on the scalp. Fukuoka applied it using the mesotherapy technique (nappage), observing satisfactory results in 12 women and 13 men. All presented increased hair strands and thickness. After four months of treatment, ADSC cells secreted cytokines – keratinocyte growth factor, vascular endothelial growth factor, platelet-derived growth factor, and hepatocyte growth factor.
Today it is known that normal adipose tissue, which can be obtained by liposuction, has similar characteristics to bone marrow stem cells. ADSC has paracrine effects with secretion, as VEGF, HGF, bFGF, PDGF, KGF, Transforming Grow Factor (TGF-beta1), insulin-like IgF-Bp, fibronectin precursors, and superoxide dismutase. These proteins have a rejuvenating effect by stimulating collagen synthesis and fibroblast migration during healing. When stem cells are subjected to the hypoxia regimen, the lesion induces an increased concentration of VEGF-A, PDGF, and TGF-beta1.
The adipose-derived stem cell protein extract (AAPE) is a ready-to-use product from the Korean Research Team at Prostemics Co., Ltd. (Seoul, Korea), with numerous growth factors. The hair treatment adds vitamins B, H, C, and E, buflomedil, CoQ10, and cysteine. Patients received 0.02 ml to 0.05 ml injections into the scalp, totaling 3 ml to 4 ml per treatment, in four sessions lasting three to five weeks, until the hair regenerated.
Zhu13 described that supplementation with adipose tissue makes a difference in hair transplantation due to the presence of Mesenchymal Embryonic Stem Cells in the adipose tissue. The author found an improvement in adipose tissue retention and also in capillary density with angiogenesis.
The 2016 literature review by Amirkhani14 presented many reports showing that human bone marrow has fat tissue similar to the function of mesenchymal cells. The study observed that umbilical cord cells derive from embryonic mesenchymal stem cells and have functions similar to those of mesenchymal cells derived from adipose tissue.
Epstein,15 in a 2018 study, addressed mesenchymal stromal cells, which are undifferentiated until they differentiate into specialized ones. Mesenchymal stromal cells are found in the bone marrow and other tissues such as the umbilical cord, placenta, adipose tissue, dental pulp, and liver. ADSC are easily isolated and secrete several cytokines, which are growth factors with paracrine effects, such as VEGF, HGF, IGF, and PDGF. These factors play a role in neovascularization. The author also argues that fat grafting before hair transplantation has helped the grafts to settle. She also states that the antiandrogenic effect of fat comes from the Aldo-keto reductase (AKR1C2) enzyme, which converts DHT into 3-Alpha Diol through 3-alpha reductase, with no systemic effect when injected into the alopecia area.
The role of fat grafting to improve facial contours began with Coleman.16
How adipose tissue is obtained with less trauma to adipose cells, as well as processing, is essential, as described by Coleman, Zhu, Benemond, and Gentile.17,18
The autologous fat grafting protocol comprises some phases.
- Donor region asepsis (abdomen, inner thigh, knee, hips, flanks, and/or buttocks).
- Infiltration of tumescent anesthesia with a solution containing SF, 2% Lidocaine without vasoconstrictor, 8.4% sodium bicarbonate, and 1:1000 epinephrine. Most researchers mention that these substances have no influence on the survival of fat cells and that their use reduces liposuction complications.
- Then, manual collection with 10ml syringes is performed, preserving the adipocytes’ integrity by using 3 mm to 4 mm blunt cannulas. It’s possible to use a 1 mm cannula, but thicker cannulas produce less negative pressure, keep the adipocytes intact, and ensure satisfactory viability. Most authors agree that fat manipulation should be as little as possible.
- The extraction of oil and blood from the liposuction can use several techniques: decanting the fat and washing two to three times with SF followed by centrifugation for 30 to 60 seconds using different speeds; mesh filtering; or the closed system Puregraft 50® (Bimini Health Tech-TX, USA-ANVISA 8058839), where the aspirated fat is injected into a sterile bag.
- The fat is injected with 3 mL syringes and 1 mm to 2 mm blunt cannulas, one hole in the tip, after the infiltration with an anesthetic solution in a ring in the area to be reconstructed.
Klinger19 implanted 1 cm3 of this tissue with mesenchymal stem cells reserves from aspirated fat on a surface of 3 cm2, demonstrating that it increases the fat grafting adherence, as well as capillary density and angiogenesis. Tesauro20 described tissue regeneration, showing the significance of fat transfer in 21 cases of alopecia. He proved that the best result of hair transplantation occurred in the region of scarring alopecia after fat grafting with tissue regeneration. The author suggested transplanting the follicles using the FUE technique three months after fat grafting.
Contrary to Tesauro, Doornaert21 contests fat survival, stating that its reabsorption is between 20% and 90%, with the replacement of adipose tissue by fibrosis and cysts.
The graft replacement theory has gained importance in numerous studies. Eto22, in 2012, collected rat inguinal fat and transplanted it into the scalp. He observed the areas of the periphery and center of the graft: the region that survived would present regeneration, and, in this process, adipocytes die and mesenchymal stromal cells survive. It produces pre-adipocytes, 20 times smaller than adult adipocytes, and with greater tolerance to ischemia. The study concluded that very few adipocytes survive grafting; however, “adipose-derived stromal cells” replace them. Fu et al.,23 supported this hypothesis by finding convincing evidence that the donor vascular fraction participates in adipogenesis and angiogenesis.
Others believe that mesenchymal host cells would replace the grafted material.
Barrera knew that in scars after third-degree burns on the scalp, when numerous procedures are performed to improve the aesthetic and physiological aspects, each surgical procedure causes more scars. For hair follicles that need microvascular anastomoses, there would be a decrease in blood flow and a consequent reduction in nutrients. However, he concluded that, due to their size, micro and mini grafts do not have many metabolic needs.
In 2013, Jung24 studied 25 cases of alopecia after burns, trauma, and surgery. The donor area was the occipital region. The recipient sites were the scalp, eyebrows, lips, and eyelids. The results were excellent in 44.4% of subjects; good in 38.9%; regular in 11.1%; and poor in 5.6%. Transplantation into scar tissue is more challenging due to impaired blood circulation and tissue stiffness. Jung also noted that the results are unsatisfactory when there are deep surgical scars. Moreno Arias25 performed four sessions of 6500 microtransplants in an inelastic plaque.
Hori,26 50 years ago (in 1972), observed that in cases of less than 24 hours post-mortem of men due to accidents, increased age showed a decrease in all layers of the scalp, except for the galea aponeurotica (male androgenetic alopecia pattern). In 70-year-old women, the dermis and hypodermis were more abundant than in men (24% and 44% less). It raised the question of whether the adipose layer would have any meaning for the health of the hair follicles.
The camouflage technique27 used on the cleft lip surgery scar was cosmetically and aesthetically acceptable. Three months after the fat grafting, hair transplantation was applied using the FUE technique, with a follow-up for 12 months. Between 2008 and 2016, Riyat28 conducted 746 studies in 1158 patients using fat grafting, with improvement in the scar (color, thickness, and volume), pain, and restoration of functions in affected areas after treatment. There was an improvement in pain in 567 of 966 patients.
Roh29 described 20 patients with scleroderma: with two graft sessions and 12 months of controlled follow-up, he obtained 51% to 75% improvement. In 2013, Zhu30 observed that different fat preparation techniques mattered: separation by gravity, centrifugation, or simultaneous washing and filtering in a closed system. He opted for the latter procedure due to reproducibility. Grafting with the elimination of supernatant oil, debris, and especially red blood cells outperforms other methods.
Cho31 showed that autologous fat improves localized scleroderma, with failure in the scalp en coup de sabre, even with hair growth.
Farjo32 assessed which patients have good or poor donor areas, mainly for implants in eyebrows, eyelashes, beard, and scalp. Mostly, it depends on the status of the donor area, such as good nutrition and vascularity. As for the hair receptor area, atrophy and post-burn scars are indications for prior fat grafting. Preparation is conducted three months before the hair transplantation. Farjo also mentions other non-surgical resources, such as scalp dyes and micropigmentation, colored spray, keratin microfibers, eyebrows and eyelashes makeup, fake eyelashes and eyebrows, partial or complete wigs, adhesive prostheses with hair, and combined wigs with ear prosthesis (indicated when there is hair loss behind the ear). He added that multiple transplants of hair follicles by FUE or FUT techniques require several years before satisfactory results.
Moreno and Akidag performed FUE hair transplantations, following them for 12 months. The procedures were conducted in two stages: first, the fat grafting; second, hair transplantation after three months. Epstein33 advocates two procedure stages to correct the scalp: fat grafting to improve scars, atrophies, and hypertrophies, and then hair transplantation. Matsumura34 observed that the hair aging process is due to the elimination of stem cells via proteolysis.
Lee, in 2020,35 made an organoid culture from a TGFbeta and FGF stem cell. He obtained an organoid cyst with a stratified epidermis, fat-rich dermis, hairy and pigmented follicles with a complete sebaceous gland, and neoformation of one follicle.
The surgeon will shave the patient’s head immediately before the surgery. Only around 1 mm of the hair in the donor area should be left to visualize and guide the hair strand direction. This author mentions the piloscope (endoscope) to predict how many FUs are in each hole and recommends platelet-rich plasma (PRP) one to two months after transplantation to avoid anagen effluvium.
The author of “Hair Transplant and Local Anesthetics”, Lam,37 mentions that many surgeons do not want to enter this field because it is overwhelmingly tedious, but it represents a perception error. When the technique is mastered, this surgery is rewarding for both the surgeon and the patient. However, this process takes a long time. The ring block marks the area to be anesthetized in the occipital and frontal regions. Buffered solutions should not be used to avoid eyelid edema. It is advisable not to reach the galea, avoiding injuries to the nerves and vessels that run alongside it.
The first consultation evaluates patients regarding the extent of the procedure, the type of alopecia, and the donor area. Laboratory tests are requested to rule out hormonal changes, autoimmune diseases, and serology for Hepatitis B, C, and HIV. Cardiac exams such as ECG, echocardiogram, and chest X-ray are also requested, in addition to photography and informed consent for FUT and FUE. Eventually, it may be necessary to switch from FUE to FUT.
The protocol includes antibiotics (cephalosporin, azithromycin, etc.), steroids (methylprednisolone 8 mg), and an oral antiemetic 30 minutes before surgery. The recipient area is carefully marked, considering the compromised region, the susceptible areas, and the patient’s expectations. Topical anesthesia helps reduce the pain of injections, but it should be applied about two hours before surgery, with an occlusive dressing for proper action.
In the FUE technique, all the hair is shaved, leaving 1 mm in length to allow the visualization of the hair strands’ orientation. After shaving, the scalp is washed with chlorhexidine degerming agent. Asepsis is performed with alcoholic chlorhexidine after monitoring vital controls and positioning the patient. Then, sterile fields are placed.
The vein is punctured, and intravenous anesthetic drugs are administered. The dosage of psychotropic medications varies according to weight, sex, and time: Fentanyl 1 mcg/kg to 3 mcg/kg, Midazolam 0.1 mg/kg to 0.5 mg/kg, Propofol 20 mg/min to 50 mg/min, in a continuous infusion pump. Doses are distributed throughout the procedure to keep the patient calm, responsive, and without losing control and airway reflexes.
Hair transplantation begins with the patient in a prone position. After sedation, tumescent infiltration is conducted inside the donor areas marking (occipital and temporal), with a solution containing 250 ml of 0.9% saline solution, 1.25 ml of epinephrine 1:1000, and 12.5 ml of 2% lidocaine without vasoconstrictor. Then, ring block anesthesia is performed. Vibration anesthesia (Blaine Labs, Santa Fe Springs CA) can be applied to mitigate the pain of the injection. The solution contains 10 ml of 1% lidocaine with 1:100,000 epinephrine, which is infiltrated subcutaneously along the lower border of the donor area. 10 ml of 1% lidocaine with 1:100,000 epinephrine is added and infiltrated to complete the anterior part of the ring. Anesthesia is infiltrated slowly, minimizing the pain. When ring anesthesia has already been administered, it is necessary to quickly inject in the subcutaneous plane of the donor area, 100 ml to 250 ml of solution with 250 ml of 0.9% SF and 1.25 ml of epinephrine 1:1000, until the tissue is rigid and whitish and achieve good tumescence, thus minimizing the transection of the neurovascular structures below the follicles.
At this point, the doctor begins harvesting the grafts. The safe donor area is situated around the occipital protuberance in the occipital midline and arches upward to approximately two fingers above the ear helix. Grafts can be removed manually, motorized, or using a robotic arm.
The punches currently used are between 0.8 mm and 1.15 mm in diameter. The most used is 0.9 mm.
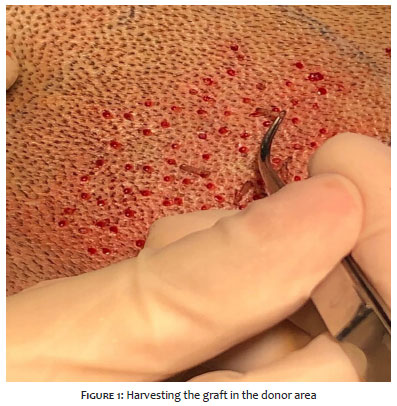
In the manual method, the surgeon cuts around the hair follicle to a depth of 2.5 mm to 3 mm using a 0.9 mm punch. At greater depths, there is a risk of transection. Blunt and hybrid punches, due to their more significant dissection effect and smaller cut, can be introduced in greater depth – larger than 4 mm – with less risk of transection (Figure 1).
In motorized methods, the punch is attached to the motor and cuts with the sharp end, which rotates up to 20,000 rpm. It’s possible to start with a speed of up to 10,000 rpm, and when reaching 2.5 mm to 3 mm in depth, the procedure is stopped and the follicle is pulled. There are the following devices: the SAFE by Harris (HSCDevelopment, Colorado, USA), the Vortex by Cole (Cole Instruments, Georgia, USA), the Ertip FUE Micromotor Silver with Nsk (autoclavable Handle), and the Artas (Restoration Robotics) just for FUE. One person pulls out the graft and places it in ice-cold saline to avoid delay. It is recommended to put a bag of ice or recyclable ice under the tub. A compress is placed to absorb the anesthetic from the holes, and the patient changes position.
ARTAS’ robotic arm employs a blunt-edge punch that slides into a sharp punch. Whether manual or motorized arm, it is recommended to place the hair in the center of the sharp punch to harvest it. It goes to a depth of 2.5 mm to 3mm; then moves to another point, and so on. It’s noteworthy that the instrument is as important as the surgeon’s skill.
After a few grafts harvesting, the FOX test should be performed.
1. All follicular units are intact: excellent, positive Fox.
2. Significant fat loss around the bottom of the follicle or 20% amputation: good Fox.
3. Difficult emerging angle: neutral Fox.
4. Significant avulsion and amputation of surrounding fat: negative Fox.
5. Significant damage, mainly in all grafts with the upper portion of the follicles avulsed from the lower segment: Fox negative.
It may be necessary to move from FUE to FUT (Follicular Unit Transplantation) technique, but one is not superior to the other as both have their own merits and demerits. It is up to the surgeon to decide whether to continue with FUE or switch to FUT. The difference is the linear scar of FUT compared to FUE. Several surgeons prefer FUT’s trichophytic closure. In the FOX test, results 1 and 2 are ideal for FUE. The transection ratio is high in results 3, 4, and 5. Often one has to switch to the FUT technique.
After harvesting the grafts, the surgeon conducts the tumescent infiltration of the receptor area in the frontal region, using 30 ml of 2% lidocaine mixed with 5 ml of 0.5% bupivacaine, 30 ml of normal saline solution, 0.5 ml of adrenaline (1:1000), and 1 ml of triamcinolone 40 mg/ml (in a regular adult).
A blade 11 or a sapphire blade with a cutting edge (ophthalmic tool) is used for incisions in the receiving area. When using needles to open the implant hole, 20 G is calculated for one hair strand, 19 G for two strands, and 18 G for three strands (Figure 2). Each follicular unit is gently implanted in each cleft.
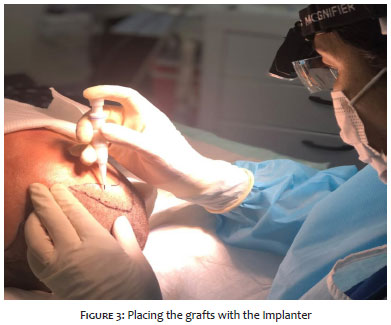
To introduce the graft, that is, to place the follicle in the orifice, a jeweler’s tweezers with a fine and delicate tip is used, which can be placed manually. This process requires two steps: one to open and another to implant. It’s possible to alternatively use the DHI (implanter from various brands such as Choi implanter Pen and Lion implanter Pen). The follicle is attached to the device, and the hole is made, leaving the follicle inside. This technique causes fewer traumas to the follicle (Figure 3). The ideal is to use 40 FUs (follicular units) per cm2 to reach a satisfactory density.
Most patients tolerate the procedure well. Pain is controlled with usual analgesics. Facial and periorbital swelling occurs on the third or fourth day after surgery and is esthetically unacceptable for the patient. Cold compresses, sleeping posture, intra and postoperative corticoids can help. Shampoo with minimal pressure can remove the crusts from the second or third day. The grafts can be washed with antiseptic shampoos, as folliculitis can appear after a few weeks, which is predictable. Prescription of antibiotics for folliculitis is infrequent. The postoperative period is resolved spontaneously without harming the grafts. The donor area heals but leaves hypopigmented spots
Complications include necrosis in the donor area, hair lightening due to hydrogen peroxide, and temporary sensory disturbances in the donor area. There may be anagen effluvium between one and three months after implantation.
In a period ranging from 6 to 12 months, the hair starts to grow.
Jimenez-Acosta38 recommends the International Society of Hair Restoration Surgery (ISHRS) courses and defines the calculation for transplantation: the ideal is to have 40 FUs/cm2 in the receiving area, but not to remove 40 FUs where there are 60 FUs/cm2 or less in the donor area. The best is homogeneous extraction of about 15-20 FUs/cm2. The FUs should not be skeletonized to have good adherence. FUE is a slow technique: it takes approximately three hours to implant 1000 FUs.
The two-stage hair transplantation technique, with prior fat transplantation, is effective for scarred hairy areas, according to the reviewed articles.
Estele Yumi Odo Toledo de Barros 0000-0002-9339-2407
Author’s contribution: Data collection, analysis, and interpretation.
Letícia Megumi Odo 0000-0002-5754-8857
Author’s contribution: Intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Marina Emiko Yagima Odo 0000-0003-1982-8388
Author’s contribution: Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript.
1. Mazzola RF, Mazzola IC. The fascinating history of fat grafting. J Craniofac Surg. 2013;24(4):1069-71.
2. Dieffenbach JF. Nonnulla de regeneratione et transplantatione. Herbipoli: Typis Richterianis; 1822.
3. Orentreich N. Autografts in alopecias and other selected dermatological conditions. Ann N Y Acad Sci. 1959;83:463-79.
4. Barrera A. The use of micrografts and minigrafts for the treatment of burn alopecia. Plast Reconstr Surg. 1999;103(2):581-4.
5. Epstein GK, Epstein JS. Mesenchymal stem cells and stromal vascular fraction for hair loss: current status. Facial Plast Surg Clin North Am. 2018;26(4):503-11.
6. Kinnaird T, Stabile E, Burnett MS, Lee CW, Barr S, Fuchs S, et al. Marrow-derived stromal cells express genes encoding a broad spectrum of arteriogenic cytokines and promote in vitro and in vivo arteriogenesis through paracrine mechanisms. Circ Res. 2004;94(5):678-85.
7. Obara K, Tohgi N, Mii S, Hamada Y, Arakawa N, Aki R, et al. Hair-follicle-associated pluripotent stem cells derived from cryopreserved intact human hair follicles sustain multilineage differentiation potential. Sci Rep. 2019;9(1):9326.
8. Pesce M, Schöler HR. Oct-4: gatekeeper in the beginnings of mammalian development. Stem Cells. 2001;19(4):271-8.
9. Tanimura S, Tadokoro Y, Inomata K, Binh NT, Nishie W, Yamazaki S, et al. Hair follicle stem cells provide a functional niche for melanocyte stem cells. Cell Stem Cell. 2011;8(2):177-87.
10. Fukuoka H, Suga H, Narita K, Watanabe, R, Shintani, S. The latest advance in hair regeneration therapy using proteins secreted by adipose-derived stem cells. Am J Cosmet Surg. 2012;29(4):273-82.
11. Fukuoka H, Narita K, Suga H. Hair regeneration therapy: application of adipose-derived stem cells. Curr Stem Cell Res Ther. 2017;12(7):531-4.
12. Shin H, Ryu HH, Kwon O, Park BS, Jo SJ. Clinical use of conditioned media of adipose tissue-derived stem cells in female pattern hair loss: a retrospective case series study. Int J Dermatol. 2015;54(6):730-5.
13. Zhu M, Zhou Z, Chen Y, Schreiber R, Ransom JT, Fraser JK, et al. Supplementation of fat grafts with adipose-derived regenerative cells improves long-term graft retention. Ann Plast Surg. 2010;64(2):222-8.
14. Amirkhani MA, Zare S, Shoaei-Hassani A, Torbati E, Nilforoushzadeh MA. Literature review of adipose-derived mesanchymal cells from history to approaches. Iran Red Cresc Med J. 2016;19(1):e22940
15. Epstein GK, Epstein JS. Mesenchymal stem cells and stromal vascular fraction for hair loss: current status. Facial Plast Surg Clin North Am. 2018;26(4):503-11.
16. Coleman SR. Facial recontouring with lipostructure. Clin Plast Surg. 1997;24(2):347-67.
17. Benemond TH, Yokomizo VMF. Lipoenxertia. In: Kadunc B, Palermo E, Addor F, et al. Tratado de cirurgia dermatológica, cosmiatria e laser. Rio de Janeiro: Elsevier; 2013.
18. Gentile P, Scioli MG, Bielli A, Orlandi A, Cervelli V. Stem cells from human hair follicles: first mechanical isolation for immediate autologous clinical use in androgenetic alopecia and hair loss. Stem Cell Investig. 2017;4(58):1-10.
19. Klinger M, Caviggioli F, Klinger FM, Giannasi S, Bandi V, Banzatti B, et al. Autologous fat graft in scar treatment. J Craniofac Surg. 2013;24(5):1610-5.
20. Tesauro P, Trivisonno A, Gennai A, Marliani A, Clauser L. Hair transplantation in cicatricial alopecia: the role of autologous fat transfer. Int J Reg Med. 2020;3(2):1-11.
21. Doornaert M, Colle J, De Maere E, Declercq H, Blondeel P. Autologous fat grafting: latest insights. Ann Med Surg (Lond). 2018;37:47-53.
22. Eto H, Kato H, Suga H, Aoi N, Doi K, Kuno S, et al. The fate of adipocytes after nonvascularized fat grafting: evidence of early death and replacement of adipocytes. Plast Reconstr Surg. 2012;129(5):1081-92.
23. Fu S, Luan J, Xin M, Wang Q, Xiao R, Gao Y. Fate of adipose-derived stromal vascular fraction cells after co-implantation with fat grafts: evidence of cell survival and differentiation in ischemic adipose tissue. Plast Reconstr Surg. 2013;132(2):363-73.
24. Jung S, Oh SJ, Hoon Koh S. Hair follicle transplantation on scar tissue. J Craniofac Surg. 2013;24(4):1239-41.
25. Moreno-Arias GA, Camps-Fresneda A. Hair grafting in postburn alopecia. Dermatol Surg. 1999;25(5):412-4.
26. Hori H, Moretti G, Rebora A, Crovato F. The thickness of human scalp: normal and bald. J Invest Dermatol. 1972;58(6):396-9.
27. Akdag O, Evin N, Karamese M, Tosun Z. Camouflaging cleft lip scar using follicular unit extraction hair transplantation combined with autologous fat grafting. Plast Reconstr Surg. 2018;141(1):148-51.
28. Riyat H, Touil LL, Briggs M, Shokrollahi K. Autologous fat grafting for scars, healing and pain: a review. Scars, Burns & Healing. 2017;3:1-16.
29. Roh MR, Jung JY, Chung KY. Autologous fat transplantation for depressed linear scleroderma-induced facial atrophic scars. Dermatol Surg. 2008;34(12):1659-65.
30. Zhu M, Cohen SR, Hicok KC, Shanahan RK, Strem BM, Yu JC, et al. Comparison of three different fat graft preparation methods: gravity separation, centrifugation, and simultaneous washing with filtration in a closed system. Plast Reconstr Surg. 2013;131(4):873-80.
31. Cho SB, Roh MR, Chung KY. Recovery of scleroderma-induced atrophic alopecia by autologous fat transplantation. Dermatol Surg. 2010;36(12):2061-3.
32. Farjo B, Farjo N, Williams G. Hair transplantation in burn scar alopecia. Scars Burn Heal. 2015 ;1:2059513115607764.
33. Kuka Epstein G, Epstein J. Two-stage procedure to correct scalp and facial scars-autologous fat grafting before hair grafting. Dermatol Surg. 2020;46(9):1262-64.
34. Matsumura H, Mohri Y, Binh NT, Morinaga H, Fukuda M, Ito M, et al. Hair follicle aging is driven by transepidermal elimination of stem cells via COL17A1 proteolysis. Science. 2016;351(6273):aad4395.
35. Lee J, Rabbani CC, Gao H, Steinhart MR, Woodruff BM, Pflum ZE, et al. Hair-bearing human skin generated entirely from pluripotent stem cells. Nature. 2020;582(7812):399-404.
36. Sharma R, Ranjan A. Follicular Unit Extraction (FUE) hair transplant: curves ahead. J Maxillofac Oral Surg. 2019;18(4):509-17.
37. Lam SM. Hair transplant and local anesthetics. Clin Plast Surg. 2013;40(4):615-25.
38. Jiménez-Acosta F, Ponce-Rodríguez I. Follicular unit extraction for hair transplantation: an update. Actas Dermosifiliogr. 2017;108(6):532-37.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}