


Marielle de Godoi Spader1; Ana Paula Naspolini1; Sérgio Emerson Sasso1; Tassiana de Boit Milanez2; Guilherme Suchard3
Financial support: None
Conflict of interest: None
How to cite this article: Spader MG, Naspolini AP, Sasso SE, Milanez TB, Suchard G. Intravascular papillary endothelial hyperplasia (Masson's tumor) in hallux nail matrix: a case report. Surg Cosmet Dermatol. 2022;14:e20220157.
Intravascular endothelial hyperplasia, or Masson’s tumor, is a benign vascular lesion with no well-defined pathogenesis. The response to vascular damage is believed to be one of the main reasons for its development. It is a typically painless injury, solitary, with slow evolution. This report aims to describe a case of Masson’s tumor in an unusual place, the hallux nail matrix, and discuss its main characteristics.
Keywords: Hyperplasia; Hallux; Endothelium, Vascular.
Intravascular papillary endothelial hyperplasia (IPEH) was primarily reported by Pierre Masson in 1923. It is characterized as a benign vascular lesion that causes reactive proliferation of endothelial cells.1,2 Since then, it has been described as intravascular angiomatosis, vascular proliferation, Masson’s pseudoangiosarcoma, or Masson’s tumor. Initially described as a specific type of hemangioma, Folke Henschen later confirmed it as a reactive non-neoplastic endothelial proliferation.2
We report the case of a 50-year-old man who presented a painless nail alteration in the right hallux with two years of evolution. He declared having already performed previous therapy for onychomycosis with oral fluconazole 150 mg/week for six months in addition to treatment with podiatry and topical antifungal for another four months, without success.
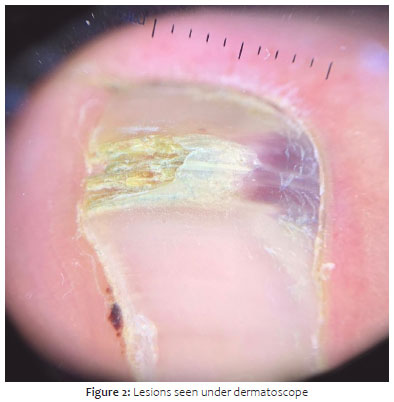
The examination revealed the presence of a longitudinal onychodystrophy of 0.5 cm, with a purplish/hemorrhagic area in the proximal 3 mm, painless to palpation (Figures 1 and 2). The ultrasound study identified a poorly defined, echogenic, subungual nodular lesion with a thickening area with little vascularization on Doppler.
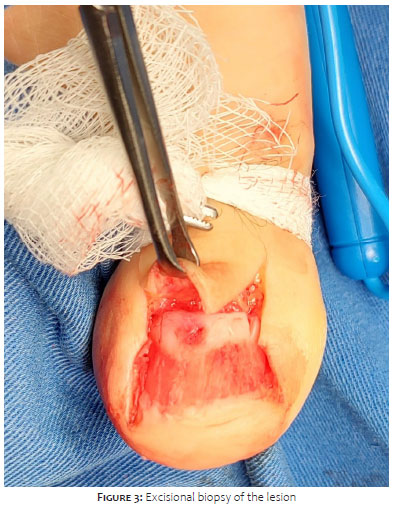
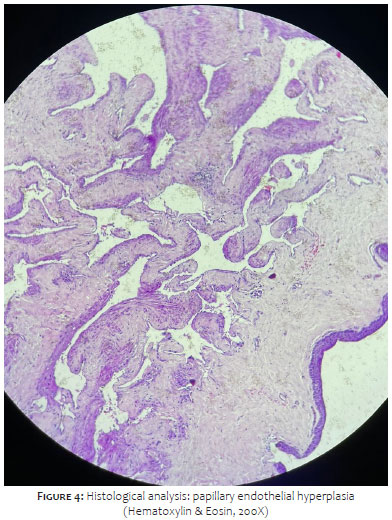
We performed an excisional biopsy of the lesion (Figure 3), whose histological section showed a proliferation of vessels in the dermis, revealing endothelium of mild cytology with papillary formations of intraluminal fibrous bundles and no atypia or atypical necrosis and/or mitosis figures. (Figure 4). The microscopic diagnosis was characteristic of papillary endothelial hyperplasia (intravascular angiomatosis) in a lesion of the nail matrix of the right hallux, and the injury extended focally to the deep margin of the fragment.
The pathophysiology of this condition is not yet fully understood, although the response to blood vessel injury or thrombosis seems to be the reason.1 The preference for women has focused on the possible involvement of hormonal factors among the pathogenic cause. The production of angiogenic growth factors and hyperemia by lymphatic stasis are also investigated as possible causes.3
Histologically, IPEH can be classified into three types: primary, pure or intravascular, which corresponds to 56% of cases and is associated with venous dilation or, less frequently, with arterial dilation; secondary or mixed (40%), which occurs due to preexisting vascular abnormalities; and extravascular or tertiary (4%), which is observed in extravascular hematomas.2,4 Histologically, it presents endothelial papillary projection within the intravascular space associated with thrombi, without endothelial stacking, atypia, or necrosis.5
It usually appears on the skin or subcutaneously as a superficial papule or deep nodule with well-defined contours.2 It is a rare tumor, comprising about 2% to 4% of skin and subcutaneous tissue vascular tumors.5 Typically, they are painless, slowly evolving, and more common in women. They are frequent in the upper limbs, head, or neck, manifesting between 30 and 40 years of age. Most injuries are unique, but the literature already described associated lesions have already.2,4
IPEH can be a lobulated, hypoechoic lesion with abundant vascularization on Doppler.6 In the case reported, we observed a heterogeneous, echogenic nodular lesion with little vascularization on Doppler. It shows how the ultrasonographic findings related to this condition can differ.
IPEH must be differentiated from malignant causes such as angiosarcoma and malignant endovascular papilloma due to their clinical and pathological similarities. The differential diagnosis from angiosarcomas is essential, as these are rarely confined to the vascular lumen.3
Surgical excision is the therapy of choice, with a favorable prognosis. Recurrence is not common and is associated with the form the excision was performed.7
Marielle de Godoi Spader 0000-0001-8957-6679
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Ana Paula Naspolini 0000-0002-7201-5709
Statistical analysis; approval of the final version of the manuscript; study design and planning; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Sérgio Emerson Sasso 0000-0002-2743-5026
Approval of the final version of the manuscript; study design and planning; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Tassiana de Boit Milanez 0000-0002-7426-1567
Data collection, analysis, and interpretation.
Guilherme Suchard 0000-0003-0561-5445
Data collection, analysis, and interpretation.
1. Mardani P, Askari A, Shahriarirad R, Ranjbar K, Erfani A, Anbardar MH, et al. Masson's tumor of the hand: an uncommon histopathological entity. Case Rep Pathol. 2020;2020:4348629.
2. Sung KY, Lee S, Jeong Y, Lee SY. Intravascular papillary endothelial hyperplasia of the finger: a case of Masson's tumor. Case Reports Plast Surg Hand Surg. 2021;8(1):23-6.
3. Luigi L, Diana R, Luca F, Pierluigi M, Gregorio L, Cicciù M. Intravascular papillary endothelial hyperplasia of the mandible: a rare entity. J Craniofac Surg. 2022;33(4):e431-3.
4. Chapman SC, Zak PW, Scaife M, Murdoch G, Eslami MH. Masson tumor (intravascular papillary endothelial hyperplasia) arising in a superficial temporal artery aneurysm. J Vasc Surg Cases Innov Tech. 2019;5(3):388-91.
5. Lauder A, Bentley RC, Mithani SK. Intraneural masson tumor of the hand. Eplasty. 2019;19:ic9.
6. Sasso SE, Naspolini AP, Milanez TB, Suchard G. Masson's tumor (intravascular papillary endothelial hyperplasia). An Bras Dermatol. 2019;94(5):620-1.
7. Leal MS, Amado C, Paracana B, Gonçalves G, Sousa M. Masson's tumour: a rare cause of cervical mass. Eur J Case Rep Intern Med. 2021;8(12):003078.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}