


Rogerio Nabor Kondo; Betina Samesima e Singh; Victória Prudêncio Ferreira; Milene Cripa Pizzato de Araújo
Financial support: None
Conflict of interest: None
How to cite this article: Kondo RN, Singh BS, Ferreira VP, Araújo MCP. Upper eyelid transposition flap for reconstruction of a lower eyelid defect: a case report. Surg Cosmet Dermatol. 2022;14:e20220156.
Squamous cell carcinoma (SCC) is the second most common skin cancer. When it is located in the lower eyelid region, the reconstruction of the resulting defect can be challenging for the dermatological surgeon, due to the local cosmetic and functional peculiarity. We report the use of an upper eyelid transposition flap for lower eyelid reconstruction with satisfactory results, both in terms of aesthetics and the resulting functionality
Keywords: Carcinoma; squamous cell; Surgical flaps; Eyelids; Eyelid neoplasms
Squamous cell carcinoma (SCC) is the second most common type of skin cancer.1 Depending on its size and location, the complete excision of this type of tumor requires using a flap to close the resulting defect.1,2 Reconstructions in the lower eyelid region become more challenging for the dermatological surgeon due to local characteristics such as aesthetic and functional aspects.3
The transposition flap (TF) is one of the possibilities for closing larger skin lesions. It uses part of the adjacent skin to fill a nearby defect with little skin laxity. The redirection of tension vectors must be carefully analyzed in advance not to generate local anatomical deformities.4
We report the case of a patient who received the modified RT technique for the reconstruction of a lower eyelid defect, using a triangular and longer flap segment instead of a rectangular, short, and slightly rounded at the distal end. This case report aims to exemplify and demonstrate a technique option to correct defects in the lower-lateral eyelid, with easy execution, in a single surgical procedure, and with satisfactory aesthetic results.
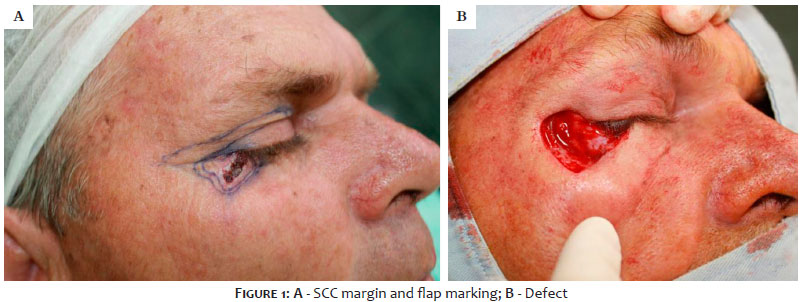
We treated a patient with SCC in the lower-lateral eyelid region on the right. A 52-year-old man, white, presented a 16 mm ulcerated plaque in the right infraocular region/outer corner (infra-lateral eyelid on the right). The histopathological examination confirmed SCC. We performed the excision of the lesion with safety margins of 4 mm. The resulting defect was 24 mm in the longest axis, and RT of the upper eyelid region was chosen (Figures 1, 2, and 3).
• Patient in horizontal supine position;
• Marking with methylene blue or surgical pen of the lesion with a 4 mm margin and flap incision sites. The marking of the flap starts at the outer corner of the orbital region, 2 mm below the eyebrow tail, extending medially for 30 mm (near the inner corner) and ending at 4 mm below the eyebrow, returning with the incision marking until meeting the upper portion of the defect. The distance from the inferior incision of the flap to the supraciliary edge must be kept above 8 mm. (Figure 1A, 2A and 2B)
• Antisepsis with topical 10% polyvinyl-iodine;
• Placement of surgical drapes:
• Infiltrative anesthesia with 2% lidocaine with vasoconstrictor;
• Incision with blade 15 of the lesion and bloc excision of the level of subcutaneous depth;
• Hemostasis;
• Incision of the flap, starting at the outer corner of the orbital region, on the upper eyelid, below the eyebrow tail, extending medially to the inner corner and returning with an incision to meet the upper portion of the defect (Figure 2A);
• Detachment of the flap of the level of subcutaneous depth (Figure 2B);
• Transposition movement of the flap from the upper eyelid portion to the defect in the lower eyelid region (Figure 2C);
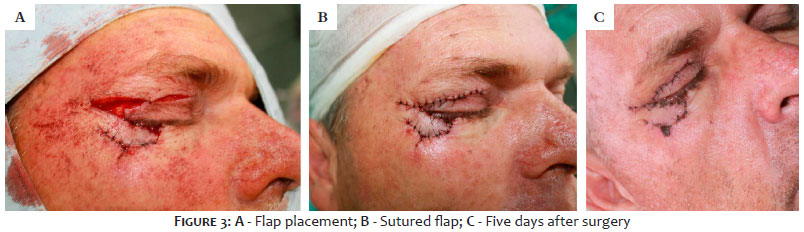
• Removal of the distal excess of the flap. Fixation of the RT over the defect and closure of the donor area with sutures with mononylon 6.0, single stitches. (Figures 3A and 3B);
• Local cleaning with saline solution;
• Occlusive dressing.
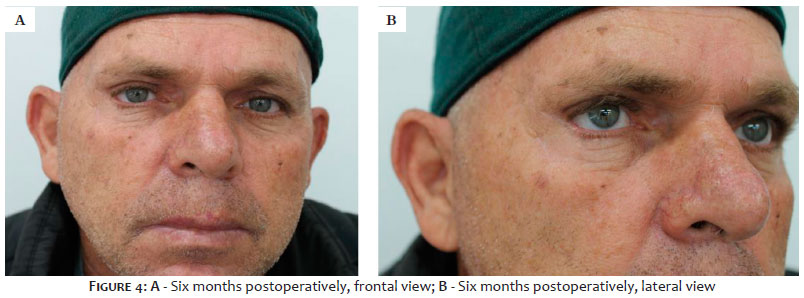
The patient evolved uneventfully in the first postoperative days (Figure 3C). There was good healing and accommodation, with satisfactory aesthetic results in the late postoperative period. (Figures 4A and 4B)
The upper and lower eyelids are complex structures with specific functions, such as protecting the eyeball from trauma, shielding from excessive light and executing movements towards the tear drainage system, also determining the eye’s beauty and expression. Therefore, reconstructions at these sites represent a major challenge for dermatological surgeons, especially when primary closure is not possible.3
Flaps can be used in lower eyelid reconstruction. The transposition flap (TF) has a linear configuration, unlike rotation flaps, which have a curvilinear configuration. A rectangular, rhomboidal, or triangular segment of skin and subcutaneous tissue is used, projecting laterally on an axis until reaching the defect that is next to or near it.4
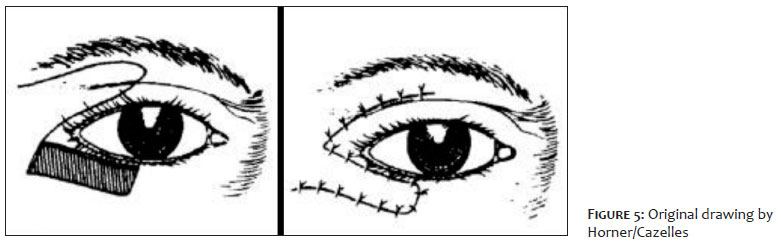
William Horner first described TF from the upper to the lower eyelid in 1837. Then Denonvilliers, in 1854, used the technique to correct cicatricial ectropion of the lower eyelid. But it was Denonvilliers’ student, Cazelles, who established the method by publishing several drawings in his doctoral thesis in 1860 (Figure 5). Currently, some authors erroneously call it Fricke’s transposition since this technique uses a monopedicle skin flap from the temporal or frontal region and not from the upper eyelid, as in the case in question.5
The present authors suggest that the flap starts at the outer corner of the orbital region, 2 mm below the eyebrow tail, as Horner/Cazelles originally proposed (Figure 5). However, they indicate that it extends a little further, near the inner corner, at 4 mm below the eyebrow, then returning to meet the upper portion of the defect. We advise keeping a >8 mm distance from the inferior incision of the flap to the supraciliary edge to avoid lagophthalmos (Figure 2A). The resulting triangular-shaped segment facilitates the primary closure of the donor area (Figures 1A, 2A and 2B).
With the modified Horner/Cazelles technique (Figures 2 and 5), the longer triangular segment and lower flap incision, with a distance greater than 8 mm from the supraciliary edge, will hide the upper eyelid scar will in the upper eyelid orbital sulcus, as the suture sites and final healing show (Figures 3C and 4A). With the stress lines distribution, the resulting force will be lateral to the defect and not caudal, preventing ectropion (Figures 4A and 4B).
Despite the knowledge and use of TF for lower eyelid defects by many dermatological surgeons, there are still few cases reported in the literature. The authors consider this procedure a good surgical option, as in our case.
TF may be a good option to resolve defects in the lower-lateral eyelid regions, considering that it solves the problem in a single surgical procedure with good cosmetics and functionality.
Rogerio Nabor Kondo 0000-0003-1848-3314
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Betina Samesima e Singh 0000-0002-6055-0341
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review.
Victória Prudêncio Ferreira 0000-0001-9642-5940
Approval of the final version of the manuscript; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review.
Milene Cripa Pizzato de Araújo 0000-0001-8749-2586
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review.
1. Gheno V, Kondo RN, Lena CP. Carcinoma espinocelular do lábio inferior: dois casos de reconstrução bilateral com retalho de Gilles associado à zetaplastia. Surg Cosmet Dermatol. 2020;12(2):182-6.
2. Pontello Junior R, Kondo RN, Pontello R. A utilização de retalho A-T para reconstrução de ferida operatória no dorso da mão. Surg Cosmet Dermatol. 2013;5(3):270-2.
3. Subramanian N. Reconstructions of eyelid defects. Indian J Plast Surg 2011;44(1):5-13.
4. Brodland DG. Flaps. In: Bolognia JL, Jorizzo JL, Rapini RP, editors. Dermatology. 4th ed. New York: Elsevier; 2018. p.2496-516.
5. Andrade A, Freitas R. Corrigindo erros históricos na reconstrução de pálpebra inferior. Bras Jour Plast Surg. 2017;32(4):594-98.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}