


Thais Florence Duarte Nogueira; Mariana Reis e Rocha Dultra; Mariana de Freitas Valente; Glaucio Farina
Financial support: None
Conflict of interest: None
How to cite this article: Nogueira TFD, Dultra MRR, Valente MF, Farina G. A-T flap for cheek reconstruction. Surg Cosmet Dermatol. 2022;14:e20220141
The cheek is the largest anatomical unit of the face. In this area, surgical skin cancer treatment must aim for its complete eradication and the best aesthetic-functional result. A 69-year-old woman presented with a 3.5 cm tumor in the left cheek for three years. Biopsy showed moderately differentiated squamous cell carcinoma. We performed an A-T flap, where the surgical defect corresponded to the “A” and the junction of the inferior orbital, nasofacial, and nasolabial grooves, to the top of the “T”. The patient evolved without recurrence and had an excellent aesthetic-functional aspect.
Keywords: Skin neoplasms; Carcinoma, Squamous cell; Zygoma; Surgical flaps; Reconstructive surgical procedures.
Approximately two to three million people are diagnosed every year with non-melanoma skin cancer nowadays.1 Also, there is a trend towards an increase in the condition incidence in recent decades due to the population aging.1,2
Among all skin malignant neoplasms, studies show that 70-80% are basal cell carcinoma (BCC) and 20% are squamous cell carcinoma (SCC).3
Regarding the topography of these skin cancers, the most affected areas of the human body are the face and neck since they are frequently exposed to ultraviolet radiation (UV), considered the most significant risk factor.3-5 The malar region is one of the areas most affected by these face tumors.5
Current treatments for skin cancer and premalignant lesions include surgical excision, curettage and electrocautery, cryotherapy, and irradiation. However, surgical excision is considered the best method for treating cancer and preventing recurrence.2
When located in the malar region, even though the complete eradication of the tumor is the primary objective, it is also essential to achieve the best possible functional and cosmetic result.4
Regarding the functional aspect, the malar anatomical unit is connected to the surrounding facial structures: eye, nose, and lip.5 The malar region defect site and possible sequelae – ectropion, effaced nasolabial fold, and mastication, phonation, and facial expression changes – should be assessed during surgical planning to avoid them.6
Concerning the cosmetic result, the malar region is complex since it is the largest facial anatomical unit and has a prominent position on the face.6,7 As it has a flat and slightly convex contour, with few shadows or depressions, it is difficult to camouflage scars and irregularities. Also, it is a critical area for emotional expression. Thus, dynamic facial movement can further highlight the surgical sequelae. One should also pay attention to the symmetry, contour, skin color and texture in the surgical planning of this area.7
Cutaneous neoplasms and surgical scars on the face can be extremely visible and cause a significant psychosocial impact on the patient. Changes in facial appearance, regardless of magnitude, can result in anxiety, depression, and social isolation.8
To obtain a good surgical result and avoid undesirable consequences, reconstructing surgical defects after surgical excision of skin cancer in the malar region becomes challenging. The used surgical reconstruction methods are primary closure, skin graft, and local and free flaps. The choice of one of these methods is based on the tumor type, size and location, the recurrence possibility, the patient’s age and health condition, and functional and cosmetic factors.2,9
Primary closure is generally an excellent reconstruction option when the surgical defect is small.9,10 However, most surgical defects in the malar region present moderate size, thus they are not responsive to primary closure. Therefore, local flaps and skin grafts are widely used to correct these defects. Among these, local flaps present superior aesthetic results.10
In this case report, we used an A-T flap to reconstruct a malar defect after the excision of a squamous cell carcinoma (SCC), a technique rarely described in the literature for reconstructing defects in this site.
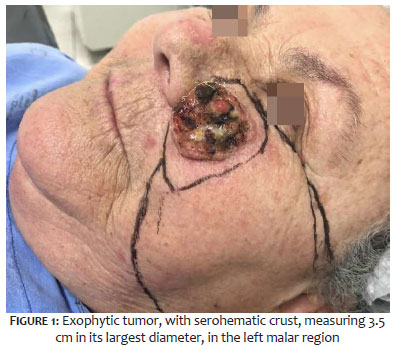
A 69-year-old white woman with osteoarthrosis presented to our Service with an exophytic tumor with serohematic crust, measuring 3.5 cm in its largest diameter, in the left malar region, three years ago. Anatomopathological examination showed moderately differentiated squamous cell carcinoma, ulcerated, and infiltrating into the hypodermis.
Thus, we planned the lesion excision. Both the patient’s late search for the Health Service and the surgery delay occurred due to the pandemic caused by the Coronavirus-19. Before the surgical procedure, the safety margin of the lesion and the configuration of the A-T advancement flap design were performed (Figure 1).
After infiltration with perilesional local anesthesia and in the flap area, the tumor was excised with a 1 cm safety margin resulting in a surgical defect with a circular shape of 4.5 cm in diameter. The flap was dissected in a plane immediately superior to the superficial aponeurotic muscle, providing an easier, faster, and safer dissection due to less bleeding and a lower risk of neural injury. The flap was sutured with 5.0 mononylon, single stitches (Figure 2).
One week later, the patient presented edema and a slight left periorbital hematoma (Figure 3). However, she evolved with good integration of the flap and the receptor area, satisfactory and rapid surgical healing, and no suture dehiscence or signs of secondary infection. Secondary ectropion did not occur.
After one year, the patient has no signs of skin cancer recurrence and has an excellent aesthetic and functional appearance (Figure 4).
The malar region reconstruction planning must consider several factors: relaxed skin tension lines orientation, maximum distensibility lines, skin surface contour, subcutaneous anatomy, patient age, comorbidities, previous surgery or radiation, tumor size, depth, and location regarding other facial subunits.7
Appropriate margins for skin tumors depend on the type of cancer, tumor size and irregularity, and the time elapsed since its onset.2 For SCC patients, surgical excision with a radial safety margin of 4 mm to 6 mm is recommended for low-risk primary cases. However, there is no consensus on the adequate safety margin for high-risk cases, and some references recommend a safety margin of 1 cm.11,12 High-risk SCCs are those with a size >2 cm, ill-defined margins, subcutaneous extension, recurrence, immunosuppression, high-risk location, or previous irradiation.4, 10, 11
In this case, the patient had a high-risk SCC since the tumor measured 3.5 cm and was located in the malar region, a high-risk anatomical site. We chose a safety margin of 1 cm to minimize the risk of recurrence.
With a safety margin of 1 cm, a 4.5 cm circular surgical defect was established in the medial malar region.
The main objectives of the ideal closure of surgical defects on the face are skin closure under minimal tension, replacement of the tissue for one as similar as possible, main anatomical structures (eye, nose, lip) preservation, and scar location corresponding to the functional and aesthetic facial units. The objective is to provide the patient with a complete reconstruction with invisible scars.12
For the surgical planning of the surgical defect, it is essential to understand the anatomy of its location. The malar region can be divided into four anatomical subunits: medial, lateral, zygomatic, and buccal. The hair implantation line in the temporal region, the preauricular crease and the mandibular inferior border delimit the malar region laterally and inferiorly. The central facial subunits mark their boundaries through the lower eyelid, nasal dorsum and ala, nasolabial folds, lip, and labial commissure superiorly and medially. Closure or flap margins should be projected along these anatomical borders or parallel to relaxed skin tension lines to camouflage surgical scars.7
Another method is grafting. An advantage of this technique is that it enables the detection of a tumor recurrence more easily.8 Moreover, the incompatibility of the graft color and texture with the skin adjacent to the defect can result in a “patch” appearance.6 8 Healing of the graft can also produce retraction capable of causing deformities of the central facial subunits that surround the malar region.13
We chose a local flap to minimize damage to normal tissue and avoid complications such as dog ears or excessive tension.14 Local flaps promote better results in terms of color, texture, and skin thickness compared to grafts.8 The choice of local flap depends on the availability of skin tissue and the location of the surgical defect. In practice, choosing the best flap depends on the surgeon’s preference.2
For moderate-sized defects in the medial malar region, the most described flaps in the literature iarea the advancement and rotation flaps. Nonetheless, many authors use the cervicofacial flap for large defects in this location.7 There are few reports on using the A-T flap at that location.
We chose to perform the A-T flap, where the surgical defect corresponded to the “A” and the junction of the inferior orbital, nasofacial, and nasolabial grooves, to the top of the “T”. The A-T flap is classified as a bilateral advancement flap according to its main movement toward the defect area.15 It is an excellent method to solve a moderate and deep defect, where the adjacent tissue does not allow direct closure.
Regardless of the surgeon’s skills, it is essential to emphasize that the surgery success rate depends on numerous patient factors, such as age, general health status, medications in use, smoking, skin characteristics (elasticity, actinic and sebaceous damage, thickness), previous scars, and individual healing capacity.12
The patient in the case evolved with excellent healing. The scar resulting from the top of the “T” was naturally hidden in the preexisting grooves (infraorbital, nasofacial, and nasolabial folds), and the “A” scar (bottom of the “T”), in the bisector of the grooves of the infraorbital and nasolabial folds (Figure 4).
The A-T flap may be a good option for resolving large defects secondary to the excision of skin tumors in the malar region. It has the advantages of being performed with local anesthetic and resolution in a single surgical time.
Thais Florence Duarte Nogueira 0000-0002-7343-0218
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Mariana Reis e Rocha Dultra 0000-0003-0510-221X
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Mariana de Freitas Valente 0000-0002-6798-7116
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Glaucio Farina 0000-0002-2273-7033
Approval of the final version of the manuscript; study design and planning; active participation in research orientation; critical revision of the manuscript.
1. WHO. Radiation: ultraviolet (UV) radiation and skin cancer. Available at: https://www.who.int/news-room/questions-and-answers/item/radiation-ultraviolet-(uv)-radiation-and-skin-cancer. 2017 Oct 16.
2. Kwon KH, Lee DG, Koo SH, Jo MS, Shin H, Seul JH. Usefulness of v-y advancement flap for defects after skin tumor excision. Arch Plast Surg. 2012;39(6):619-25.
3. Park YJ, Kwon GH, Kim JO, Kim NK, Ryu WS, Lee KS. A retrospective study of changes in skin cancer characteristics over 11 years. Arch Craniofac Surg. 2020;21(2):87-91.
4. Badash I, Shauly O, Lui CG, Gould DJ, Patel KM. Nonmelanoma facial skin cancer: a review of diagnostic strategies, surgical treatment, and reconstructive techniques. Clin Med Insights Ear Nose Throat. 2019;12:1179550619865278.
5. Choi JH, Kim YJ, Kim H, Nam SH, Choi YW. Distribution of basal cell carcinoma and squamous cell carcinoma by facial esthetic unit. Arch Plast Surg. 2013;40(4):387-91.
6. Başağaoğlu B, Bhadkamkar M, Hollier P, Reece E. Approach to reconstruction of cheek defects. Semin Plast Surg. 2018;32(2):84-9.
7. Cass ND, Terella AM. Reconstruction of the cheek. Facial Plast Surg Clin North Am. 2019;27(1):55-66.
8. Lee KS, Kim JO, Kim NG, Lee YJ, Park YJ, Kim JS. A comparison of the local flap and skin graft by location of face in reconstruction after resection of facial skin cancer. Arch Craniofac Surg. 2017;18(4):255-60.
9. Chang JW, Lim JH, Lee JH. Reconstruction of midface defects using local flaps: An algorithm for appropriate flap choice. Medicine (Baltimore). 2019;98(46):e18021.
10. Work Group; Invited Reviewers, Kim JYS, Kozlow JH, Mittal B, Moyer J, Olenecki T, Rodgers P. Guidelines of care for the management of cutaneous squamous cell carcinoma. J Am Acad Dermatol. 2018;78(3):560-78.
11. Veness MJ. High-risk cutaneous squamous cell carcinoma of the head and neck. J Biomed Biotechnol. 2007;(3):80572.
12. Bordianu A, Bobirca F. Facial skin cancer surgery under local anesthesia. J Med Life. 2018;11(3):231-7.
13. Pérez-Paredes MG, González-Sixto B, Otero-Rivas MM, Rodríguez-Prieto MÁ. Reconstructive surgery of the medial zygomatic region of the cheek: presentation of 5 cases. Actas Dermosifiliogr. 2014;105(4):e27-31.
14. Heller L, Cole P, Kaufman Y. Cheek reconstruction: current concepts in managing facial soft tissue loss. Semin Plast Surg. 2008;22(4):294-305.
15. Li ZR, Jiang Y, Zhang JY, Su YW, Hu JZ. Modified O-T advancement flap for reconstruction of skin defects. Int J Clin Exp Pathol. 2017;10(9):9158-63.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}