


Masoumeh Roohaninasab1; Kimia Gandomkar2; Azadeh Goodarzi1
Financial support: None
Conflict of interest: None
How to cite this article: Roohaninasab M, Gandomkar K, Goodarzi A. Microneedling in vitiligo: A systematic review. Surg Cosmet Dermatol. 2022;14:e20220123.
BACKGROUND: Microneedling was initially introduced for skin rejuvenation. This review analyzes the current literature on microneedling techniques, efficacy, and safety for vitiligo treatment.
METHODS: An extensive PubMed search was performed to identify literature on microneedling therapy for vitiligo. Case reports, case series, and clinical trials were included.
RESULTS: All 14 articles evaluated showed improvement of lesions after microneedling treatment. Combination of microneedling and topical tacrolimus, 5-FU, topical calcipotriol and betamethasone, NB-UVB with or without PDT, and triamcinolone acetonide solution yielded more efficacy than microneedling monotherapy.
CONCLUSION: Microneedling is a safe and efficient technique and an adjuvant treatment for vitiligo treatment.
Keywords: Vitiligo; Efficacy; Evaluation of the efficacy-effectiveness of interventions; Review; Rejuvenation; Dermatology; Depigmentation; Needling
Vitiligo is characterized by the appearance of circumscribed depigmented spots affecting the skin, hair, and mucous membrane. The disease has a high relapsing rate and negatively affects the quality of life.1-3 Patients who have vitiligo experience low self-esteem. Global prevalence of vitiligo is between 0.5% and 2%, with reported rates varying geographically, according to a self-reported survey conducted in Europe, Japan, and the United States (US), which polled participants aged 18 and up in an online global survey.1 The average age of onset for this disorder is under 20, but it can strike at any age. Owing to the absence of melanocytes from the cutaneous epidermis or the inability to secrete melanin, dyschromia manifests as depigmented macules. This is caused by a lack of the tyrosine enzyme in melanocytes, which activates the pigment formation process. The psychological and emotional toll this disorder takes on patients is significant, and developing new, more appropriate treatment options is essential.2 Vitiligo has complex pathogenesis, and the precise etiology is still unclear. It was suggested that different factors, especially genetic influences, stress, autoimmune predisposition, dysfunctional biochemical pathway, and trauma might act synergistically in the disappearance of melanocytes from the skin.4-6
Vitiligo is not ‘‘just a cosmetic disorder”: it is challenged by social outcasting and stigmatization causing an overwhelming psychological burden in affected patients.1,2 Six multiple therapeutic modalities are currently available to treat vitiligo, but none of them achieve long-term remission in this unpredictable disease. Tacrolimus (T) is one of the topical immunomodulators that inhibits calcineurin. It has been successfully used to treat vitiligo. Tacrolimus inhibits T-cell activation, and it can be used as an adjuvant or alternative to topical steroids to avoid the associated adverse events that may result from its prolonged use.7 Microneedling (Mn) enables the delivery of drugs and larger protein molecules through the epidermis. The device has fine needles to create micro channels into the skin. Moreover, Mn stimulates the release of growth factors that are essential for skin rejuvenation.8,9 A recent approach using needling showed favorable degrees of repigmentation.7 It can be performed using simple injection needles or microneedling devices such as manual rollers, dermarollers, automatic needle pen devices, and microneedling fractional radiofrequency devices.8,9
Microneedling is better than simple needles in controlling penetration depth, thus preventing excessive pain during injection.8 It causes micro-inflammation in the epidermal layer that enhances melanocytes and keratinocyte migration and stimulates vitiligo areas repigmentation.10 Additionally, it provides successful melanocytes grafting from pigmented to unpigmented areas and improves the penetration of topical agents into the skin.3, 11
Microneedling in monotherapy or combined with therapeutic injection can be a potential treatment for vitiligo. The technique has been modestly expanded in recent years without a standardized approach. Since there is no unified method to treat the causes of vitiligo, choosing the right treatment modality and predicting its efficacy is difficult. Also, microneedling has been increasingly used in clinical practice. Thus, it seemed vital to review all studies, including clinical trials, to offer better insight for physicians.
This work aims to provide a current guide for practice based on the best available evidence of microneedling for vitiligo treatment and comparing the different methods and its efficacy when accompanied with topical therapies.
We sought eligible studies, without limitation publication status, which met the following criteria: (i) randomized controlled trials (RCTs) involving vitiligo patients; (ii) undergoing NB-UVB therapy in the treatment group, whatever combined with other treatments or not; (iii) undergoing photo (chemo) therapy in the control group, combined with other treatments or not; (iv) measurement of re-pigmentation degree and (v) articles published in English.
Two investigators independently searched The PubMed and Cochrane libraries using the open strings “UVB”, “NB-UVB”, “narrow-band ultraviolet B”, “vitiligo”, “random”, “randomized control trial” and “RCT”. Searches were conducted to cover the period from the earliest available date to November 2013. Reference lists of prior reviews, systematic reviews, and trials were also checked.
Two investigators independently screened studies for inclusion, retrieved potentially relevant studies, and determined eligible studies. Disagreements were resolved by consensus. Two investigators independently extracted data from included studies using standardized forms, and a third investigator was assigned to check the process. The data included the number and age of participants, duration, vitiligo type or stage, treatments sessions, mean sessions of the initial response, cumulative dose of total phototherapy, cumulative dose of the initial response, treatment interval, interventions of treatment group and control group, efficacy and safety.
We used the criteria recommended by the Cochrane Collaboration Handbook to assess the methodological quality of included trials. It chiefly concentrated on description of randomization (sequence generation progress), allocation concealment, blinding, addressing incomplete outcome data, reporting of selective outcome and other potential threats to validity.11 The conclusive answer for each was “Yes”, indicating “low risk of bias”; “No”, indicating “high risk of bias”; and “Unclear”, indicating “either lack of information or uncertainty over the potential for bias”.11 Consensus among the third investigator resolved the disagreements.
The primary outcome was re-pigmentation degree. We estimated the trials that mentioned the number of patients who achieved 50%, 60% or 75% re-pigmentation. Secondary outcomes included: (i) adverse events; (ii) mean sessions of initial response; and (iii) cumulative dose of total phototherapy or cumulative dose of initial response.
Two investigators performed all statistical analyses using the duplicate data entry facility of RevMan 5.0. In addition to 95% confidence intervals (CIs), relative risks (RRs) were used for dichotomous outcomes. The I2 statistics were calculated to determine the proportion of between-study variation due to heterogeneity. The value ranges from 0 to 100%, and high values indicate strong heterogeneity. If heterogeneity was low (p40.1, I 2 550%), a fixed-effects model was used for analysis; otherwise, a random effects model or descriptive analysis was used. A funnel plot was used to detect publication bias. P50.05 was considered statistically significant between the treatment group and control group.
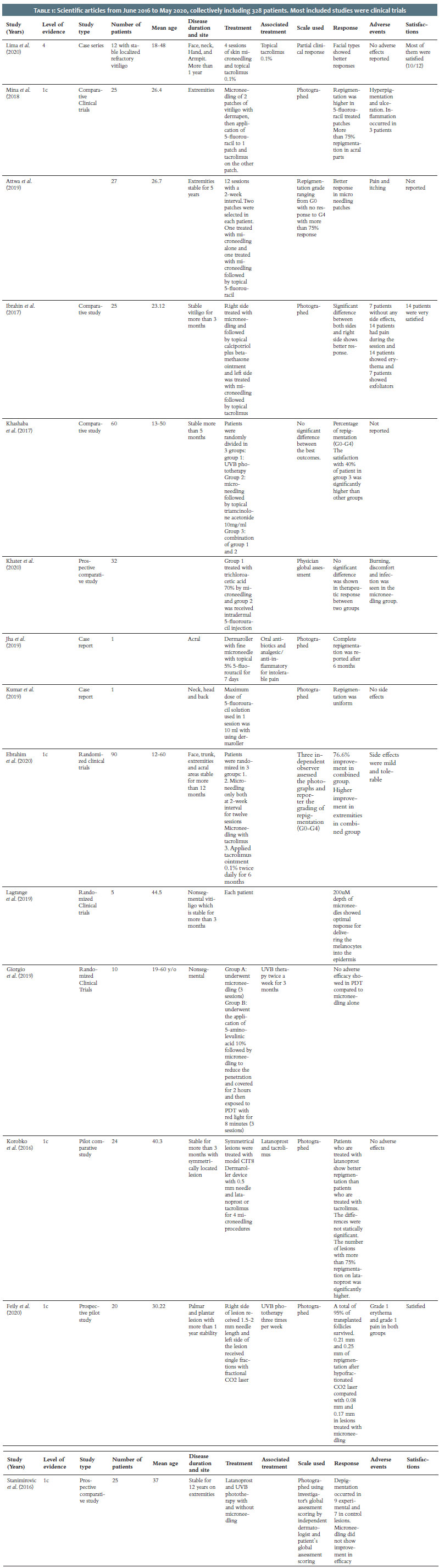
The authors’ search identified 14 scientific articles from June 2016 to May 2020, comprising 328 patients. Most included studies were clinical trials. The level of evidence ranged from 1B (2 studies) and 1C (9 studies) to 4 (3 studies) (Table 1). 12
Most patients were photographed pre and post-treatment using standard camera or UV light pictures. The most common measure used to assess repigmentation was the 5-grade repigmentation scale (or Physician’s Global Assessment - PGA), ranking from G0 to G411: G4 (excellent: >75% repigmentation), G3 (very good: 50%-75% repigmentation), G2 (good: 25%-50% repigmentation), G1 (satisfactory: <25% repigmentation), and G0 (poor: no repigmentation).11,13-18 Visual analog scale was used in three studies. 10, 18-20 Other studies used the investigator’s global assessment (IGA) score and the measure of repigmentation diameter. 21, 22
Microneedling relies on the principle of neovascularization and neocollagenesis that result from micro-injuries following needle piercing.
Two clinical trials proved that microneedling is effective to treat vitiligo using a five grading scale to assess repigmentation.14,16 The study included 57 patients with localized stable vitiligo for at least three years. Topical anesthetic cream (lidocaine) was applied to the lesion. An electronic dermapen with needles varying from 1 mm or 1.5 mm to 2 mm according to the skin thickness was applied until bleeding appeared. The patient received 6 to 12 sessions at two week-interval.14,16 The authors observed a clinical response in 38.5% of patients among which 17.5% had excellent repigmentation. The best response was seen on the face, followed by the trunk. 16
Topical tacrolimus has been successfully used to treat vitiligo. Since microneedling enhances drug delivery across the skin barrier,16 tacrolimus ointment was applied after microneedling under occlusive dressing for six hours, and patients were then advised to apply it once daily every two weeks.13,16 All patients underwent 12 microneedling sessions (at two-week interval), except in one study where the patients received four sessions at 15-day interval. 3, 15, 16
Microneedling combined with tacrolimus was more efficient than microneedling monotherapy.16 The studies observed a clinical response in 83.6% (n=97) of patients receiving combined therapy.3,13,15,16,23 The clinical response grades were: partial clinical response (n=10, 11.6%), G1 (n=14, 16.3%), G2 (n=24, 31.4%), G3 (n=15, 17.4%), G4 (n=4, 4.7%), G2 (n=42, 48.8%), with >24% repigmentation (n=12, 14%).
The highest repigmentation rate was observed on the face (n=12, 70% repigmentation).3,16 The same study recorded excellent repigmentation (grade G4, >75% repigmentation) in three patients with vitiligo patches on the legs, but these results were not achieved on acral areas or bony prominences.3,13,16 However, Ibrahim et al. showed excellent results in vitiligo on the elbows (n=3, 83.33% repigmentation).15
One clinical trial compared the efficacy of microneedling with calcipotriol (0.05 mg/g) plus betamethasone (0.5 mg) versus tacrolimus in vitiligo treatment. Symmetrical patches over the elbows, knees, extremities, and acral areas were treated with microneedling every two weeks for 12 sessions, and calcipotriol plus betamethasone or tacrolimus was applied immediately after the procedure. 15
Microneedling with topical calcipotriol plus betamethasone was superior to microneedling with tacrolimus in treating vitiligo. It showed earlier clinical responses and needed fewer sessions. The study noted a significantly greater repigmentation in the treated extremities patches.15 Excellent results were observed in elbow (n=3, 99% repigmentation) and extremities (n=8, 83.3% repigmentation), moderate results in acral areas (n=6, 50% repigmentation), and knees had the lowest repigmentation rates (n=8, 67.5% repigmentation).15
The efficacy of microneedling in combination with latanoprost and NB-UVB has been investigated on resistant vitiligo patches.21 Patients were divided into two groups: microneedling (four sessions at one-week interval) combined with latanoprost and NB-UVB, and latanoprost associated with NB-UVB without microneedling. Topical latanoprost solution (0,005%) was applied immediately after microneedling. Then, the patients were prescribed NB-UVB in the period between microneedling sessions. The study showed that 37.8% of treated patches achieved satisfactory to very good repigmentation; however, there was no statistically significant difference in repigmentation between the two groups.
Another pilot study confirmed the efficacy of latanoprost combined with NB-UVB. However, the authors could not conclude whether microneedling further improved the therapeutic outcome.23
Two studies assessed the efficacy of Microneedling and 5-FU. Patients received 6 or 12 sessions of microneedling at two-week interval.13,14,20 After microneedling, 5-FU solution (5%) was applied topically over affected areas and covered using an occlusive dressing for one day.13,14 The patient was advised to apply 5-FU once daily for two weeks.13
Attwa et al. showed that the combination of microneedling with 5-FU yielded better results than microneedling monotherapy and increased its efficacy by 3.8 times.14
The second study aimed to compare the efficacy of microneedling with 5-FU versus its efficacy with tacrolimus. This study showed that the combination of 5-FU with microneedling has better results with excellent repigmentation and a higher number of clinical responses than the combination with tacrolimus.13 The 5-FU showed excellent to good results in 40% of acral areas (repigmentation >75%) and in 57.1% of bony prominence regions (elbow and knees).13
Similar case reports showed complete repigmentation in acral, face, and back areas treated with 5-FU and microneedling.19,20
A randomized clinical trial assessed the additional efficacy of PDT on microneedling and NB-UVB therapy in acral areas. Since the NB-UVB is considered the gold standard in vitiligo treatment, it was applied twice a week for three months to treat vitiligo. Additionally, patients received three sessions of microneedling at three-week interval; then a group of these patients received 5-aminolevulinic acid 10% (applied under coverage for two hours) and were exposed to PDT with red light (630 nm) for eight minutes (37 J/cm2).10 This study failed to prove any additional efficacy of PDT to microneedling therapy, and 40% of patients had a clinical response versus 60% in the other group (microneedling + NB-UVB).10
Another clinical study compared the efficacy of microneedling alone or with NB-UVB versus NB-UVB alone. It proved that needling and NB-UVB yielded better results when combined.17 Repigmentation was seen in all patients treated with combined therapy and in 80% of patients treated with NB-UVB or microneedling monotherapy.17 The grade of repigmentation in each group was: NB-UVB monotherapy: G1 (n=6), G2 (n=6), G3 (n=4); microneedling and triamcinolone acetonide solution: G1 (n=3), G2 (n=4), G3 (n=6), G4 (n=3); combination of both modalities: G1 (n=1), G2 (n=5), G3 (n=8), G4 (n=6).
A study comparing microneedling and non fractioned ablative Erbium laser for autologous cell suspension grafting in nonsegmental vitiligo showed that needling alone was ineffective in preparing the grafting bed, and none of the patients treated with microneedling had repigmentation.11 Laser-assisted dermabrasion followed by suspension in hyaluronic acid achieved better results, where 50% of patients had excellent repigmentation.11
A prospective comparative study assessed the efficacy of trichloroacetic acid (TCA) with microneedling versus 5-FU in non-segmental vitiligo areas. In the first group, TCA was applied immediately after patients underwent microneedling until a uniform ivory white frothing appeared.18 In the second group, an injection of 0.01-0.02 ml 5-FU was applied intradermally in vitiligo areas at 1 cm intervals with a maximum of 250 mg per session. Both groups received treatment every two weeks for two months.18
The study observed no significant difference between patients treated with TCA and 5-FU. In both groups, 43.8% of patients had good-to-excellent improvement (repigmentation >50%).18
A pilot study compared the efficacy of hair transplantation and CO2 laser or microneedling followed by NB-UVB to treat stable and refractory palmoplantar vitiligo.22 The authors compared two treatment approaches on symmetrical and comparable vitiligo lesions. Pigmented follicular grafts were harvested from the scalp and transplanted in vitiligo lesions on day 0. On days 30±4 and 60±4, left-sided lesions received single fractions with a fractional CO2 laser, MX-7000 (10,600 nm, 100-MJ pulse energy, and 200 spots/cm3 in static mode), and right-sided lesions received microneedling (1.5 mm to 2 mm) until bleeding appeared. On both sides, topical anesthesia with lidocaine-prilocaine was used before intervention. On days 30±4 and 60±4, after the primary treatment, silver sulfadiazine ointment was applied to both sides, twice daily, for five days. Both sides received NB-UVB on day 40.22
The study noted no statistically significant difference between both sides, and both had a 0.25 mm repigmentation diameter.22
Most (83.3%) patients treated with microneedling and topical tacrolimus were satisfied with the treatment outcome.3 A higher percentage of patients (92%) were satisfied with topical calcipotriol and betamethasone treatment.15
The combination of microneedling with 5-FU yielded excellent results with a good satisfaction rate in Kumar et al. study.20
Microneedling combined with triamcinolone acetonide solution yielded a good-to-excellent satisfaction rate in 55% of patients, whereas microneedling associated with triamcinolone acetonide solution and NB-UVB raised that percentage to 75%.
The study observed high satisfaction rates in patients treated with hair transplantation and CO2 laser or microneedling followed by NB-UVB.22
A skin biopsy was taken from the lesions during pre and post-treatment sessions for histological evaluation. The biopsies were stained using routine hematoxylin and eosin (H&E) and then with HMB45 to detect any pathological or immunohistochemical changes. Lesions treated with microneedling and tacrolimus had a higher expression than microneedling or tacrolimus monotherapy.16 These results were consistent with the clinical outcome. A comparison between microneedling and tacrolimus and microneedling and 5-FU yielded better results in patients treated with microneedling and 5-FU.13
Also, lesions treated with microneedling with dermapen and topical calcipotriol plus betamethasone had a higher expression than those treated with microneedling and topical tacrolimus.15
No patient presented severe adverse events related to the microneedling treatment. The post-procedure adverse events were: pain,11,14-17,22 erythema,15,16,22 hyperpigmentation,13 itching,14,16 ulceration,13 inflammation,13 and exfoliation15.
No complications were noted in 18.6 % of patients treated with tacrolimus and microneedling (n=26).3,13 Only mild erythema, itching, and pain were observed in symptomatic patients.15,16,23 Most patients (56.2%) treated with TCA and 5-FU had no adverse events. The adverse events reported with TCA were
blister (n=1), burning (n=2), and perilesional hyperpigmentation (n=4). Regarding 5-FU, adverse events were discomfort (n=2) and infection (n=3).18
Significantly greater pain level was noted in patients treated with laser-assisted dermabrasion compared to patients treated with microneedling.
Recently, there has been heightened interest in using microneedling for skin disorders. It consists of a roll with fine needles. These microneedles create micro-injuries and activate wound healing cascade, releasing several factors including platelet-derived growth factor (PGF), transforming growth factor alpha and beta (TGF-α and TGF-β), connective tissue activating protein (CTAP), connective tissue growth factor (CTGF), and fibroblast growth factor (FGF).24 These factors enhance the collagen secretion by fibroblast and stimulate melanocyte migration to unpigmented patches.10
Vitiligo is a chronic disease characterized by depigmented white patches and caused by the destruction of melanocytes.4,25 These patches occur mainly on extremities and are known to be resistant to conventional therapies, hence the importance of finding an effective treatment modality for these difficult-to-treat areas.26,27 It has a worldwide prevalence of 1%, occurring chiefly before the age of 20 and affecting both sexes equally.4,28-31
Microneedling can treat the loss of melanocytes caused by vitiligo. It can potentially stimulate melanocytes and skin pigmentation by creating micro-injuries, leading to the release of growth factors.10,32 Thus, microneedling alone can act as monotherapy for vitiligo, increasing the transdermal drug delivery of topical treatment options and, therefore, inducing a better repigmentation rate when combined with these topical treatments.
Microneedling is a relatively new treatment in dermatology and has been used for many skin disorders such as vitiligo, acne scarring, and skin rejuvenation. This article emphasized all published studies that assessed the efficacy of microneedling in vitiligo treatment. Microneedling proved to be efficient in all these studies; however, the degree of efficacy varied depending on associated therapies. There was inconstancy in scales used to assess the efficacy of microneedling monotherapy and biotherapy. Nevertheless, the combination of microneedling and topical tacrolimus, 5-FU, topical calcipotriol and betamethasone, NB-UVB with or without PDT, or triamcinolone acetonide solution was more efficient compared to microneedling monotherapy. On the other hand, microneedling was not efficient for autologous cell suspension grafting and showed no clinical response. Also, it showed no additional benefit in patients treated with latanoprost and NB-UVB.21
No life-threatening adverse events were reported. Compared to lasers, microneedling caused significantly less pain.11,33
Satisfaction rate results were not conclusive since only four studies described it. The higher satisfaction rate was seen in microneedling combined with topical calcipotriol and betamethasone, or NB-UVB and triamcinolone.
This study has many limitations. Due to the lack of uniformity of studies, a meta-analysis could not be performed, and this study was limited to a pooled data form. The high variability between scales used to measure satisfaction and repigmentation rate and the scarce number of patients followed up restricted our inter-study comparison. In this study, only the published data from the database mentioned were included, which is also a limitation.
The authors published many studies about vitiligo and its treatments. Therefore, microneedling in vitiligo seems to be a hot topic to work.29-37
Microneedling seems to be a safe adjuvant therapy besides routine treatments and is an efficient and tolerable procedure for vitiligo treatment and can be an added value in resistant patches or difficult-to-treat areas such as the extremities, especially when used in combination with topical agents.
Additional standardization of treatment dosing protocols and further randomized clinical trials are needed to establish a consensus about microneedling in vitiligo. Based on the result, the combination of microneedling and topical tacrolimus, 5-FU, topical calcipotriol and betamethasone, NB-UVB with or without PDT, or triamcinolone acetonide solution was more efficient compared to microneedling monotherapy. However, there was no specific scale between all studies to compare the results, and it we suggest further studies with a single criterion to measure the effectiveness and satisfaction of patients with the treatment.
The authors thank Rasool Akram Medical Complex Clinical Research Development Center (RCRDC) specially Mrs Farahnaz Nikkhah for their technical and editorial assistance.
Masoumeh Roohaninasab 0000-0002-2862-6422
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; active participation in research orientation; critical literature review; critical revision of the manuscript.
Kimia Gandomkar 0000-0002-3901-6718
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Azadeh Goodarzi 0000-0002-1249-4429
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; active participation in research orientation; critical literature review; critical revision of the manuscript.
1. Grimes PE, Miller MM. Vitiligo: patient stories, self-esteem, and the psychological burden of disease. Int J Womens Dermatol. 2018;4(1):32-7.
2. Ongenae K, Dierckxsens L, Brochez L, van Geel N, Naeyaert JM. Quality of life and stigmatization profile in a cohort of vitiligo patients and effect of the use of camouflage. Dermatology. 2005;210(4):279-85.
3. Andrade Lima EV, Andrade Lima MMD, Miot HA. Induction of pigmentation through microneedling in stable localized vitiligo patients. Dermatol Surg. 2020;46(3):434-5.
4. Ezzedine K, Eleftheriadou V, Whitton M, van Geel N. Vitiligo. Lancet. 2015;386(9988):74-84.
5. Konstantinova VA, Olisova OY, Gladko VV, Burova EP. Vitiligo - New Treatment Approach. Clin Cosmet Investig Dermatol. 2019;12:911-7.
6. Dillon AB, Sideris A, Hadi A, Elbuluk N. Advances in vitiligo: an update on medical and surgical treatments. J Clin Aesthet Dermatol. 2017;10(1):15-28.
7. Wassef C, Lombardi A, Khokher S, Rao BK. Vitiligo surgical, laser, and alternative therapies: a review and case series. J Drugs Dermatol. 2013;12(6):685-91.
8. AlJasser MI, Altalhab S. Controlled depth of needling using simple injection needles. J Am Acad Dermatol. 2020;83(5):e331-e332.
9. Mujahid N, Shareef F, Maymone MBC, Vashi NA. Microneedling as a treatment for acne scarring: a systematic review. Dermatol Surg. 2020;46(1):86-92.
10. Giorgio CM, Caccavale S, Fulgione E, Moscarella E, Babino G, Argenziano G. Efficacy of microneedling and photodynamic therapy in vitiligo. Dermatol Surg. 2019;45(11):1424-6.
11. Lagrange S, Montaudié H, Fontas E, Bahadoran P, Lacour JP, Passeron T. Comparison of microneedling and full surface erbium laser dermabrasion for autologous cell suspension grafting in nonsegmental vitiligo: a randomized controlled trial. Br J Dermatol. 2019;180(6):1539-40.
12. TCfE-BMOC. Available at https://www.cebm.net/2009/06/oxford-entreevidencebasedmedicine-f, levels-evidence-march-2009/. Accessed January 10.
13. Mina M, Elgarhy L, Al-Saeid H, Ibrahim Z. Comparison between the efficacy of microneedling combined with 5-fluorouracil vs microneedling with tacrolimus in the treatment of vitiligo. J Cosmet Dermatol. 2018;17(5):744-51.
14. Attwa EM, Khashaba SA, Ezzat NA. Evaluation of the additional effect of topical 5- fluorouracil to needling in the treatment of localized vitiligo. J Cosmet Dermatol. 2020;19(6):1473-78.
15. Ibrahim ZA, Hassan GF, Elgendy HY, Al-Shenawy HA. Evaluation of the efficacy of transdermal drug delivery of calcipotriol plus betamethasone versus tacrolimus in the treatment of vitiligo. J Cosmet Dermatol. 2019;18(2):581-8.
16. Ebrahim HM, Albalate W. Efficacy of microneedling combined with tacrolimus versus either one alone for vitiligo treatment. J Cosmet Dermatol. 2020;19(4):855-62.
17. Elshafy Khashaba SA, Elkot RA, Ibrahim AM. Efficacy of NB-UVB, microneedling with triamcinolone acetonide, and a combination of both modalities in the treatment of vitiligo: a comparative study. J Am Acad Dermatol. 2018;79(2):365-7.
18. Khater M, Nasr M, Salah S, Khattab FM. Clinical evaluation of the efficacy of trichloroacetic acid 70% after microneedling vs intradermal injection of 5-fluorouracil in the treatment of nonsegmental vitiligo; A prospective comparative study. Dermatol Ther. 2020:e13532.
19. Jha AK, Sonthalia S. 5-Fluorouracil as an adjuvant therapy along with microneedling in vitiligo. J Am Acad Dermatol. 2019;80(4):e75-e6.
20. Kumar A, Bharti R, Agarwal S. Microneedling with Dermaroller 192 needles along with 5- fluorouracil solution in the treatment of stable vitiligo. J Am Acad Dermatol. 2019;81(3):e67- e9.
21. Stanimirovic A, Kovacevic M, Korobko I, Šitum M, Lotti T. Combined therapy for resistant vitiligo lesions: NB-UVB, microneedling, and topical latanoprost, showed no enhanced efficacy compared to topical latanoprost and NB-UVB. Dermatol Ther. 2016;29(5):312-6.
22. Feily A, Firoozi Farda, Sokhandani T, Elosegui-Rodriguez P, Perez-Rivera E, Lange CS, et al. Follicular transplantation, microneedling, and adjuvant narrow-band ultraviolet-B irradiation as cost effective regimens for palmar-plantar vitiligo: a pilot study. Cureus. 2020;12(4):e7878.
23. Korobko IV, Lomonosov KM. A pilot comparative study of topical latanoprost and tacrolimus in combination with narrow-band ultraviolet B phototherapy and microneedling for the treatment of nonsegmental vitiligo. Dermatol Ther. 2016;29(6):437-41.
24. Singh A, Yadav S. Microneedling: Advances and widening horizons. Indian Dermatol Online J. 2016;7(4):244-54.
25. Singh RK. Impact of ultraviolet light on vitiligo. Adv Exp Med Biol. 2017;996:55-60.
26. Whitton ME, Pinart M, Batchelor J, Leonardi-Bee J, González U, Jiyad Z, et al. Interventions for vitiligo. Cochrane Database Syst Rev. 2015(2):Cd003263.
27. M K, Narayan N. A rare case of hemi - corpus vitiligo. J Evol Med Dent Sci. 2015;04(2):297-302.
28. Whitton M, Pinart M, Batchelor JM, Leonardi-Bee J, Gonzalez U, Jiyad Z, et al. Evidence- based management of vitiligo: summary of a Cochrane systematic review. Br J Dermatol. 2016;174(5):962-9.
29. Ezzedine K, Silverberg N. A practical approach to the diagnosis and treatment of vitiligo in children. Pediatrics. 2016;138(1):e20154126.
30. Khademi M, Roohani Nasab M, Goodarzi A, Seirafi Pour F, Dodangeh M, Khademi A. The healing effects of facial BOTOX injection on symptoms of depression alongside its effects on beauty preservation. J Cosmet Dermatol. 2021;20(5):1411-5.
31. Roohaninasab M, Goodarzi A, Ghassemi M, Sadeghzadeh-Bazargan A, Behrangi E, Najar Nobari N. Systematic review of platelet-rich plasma in treating alopecia: Focusing on efficacy, safety, and therapeutic durability. Dermatol Ther. 2021 Mar;34(2):e14768.
32. Roohani Nasab M, Mansouri P, Seirafi Pour F, Naeini AJ, Goodarzi A. Therapeutic options and hot topics in vitiligo with special focus on pediatrics' vitiligo: a comprehensive review study. Dermatol Ther. 2021;34(1):e14550.
33. Roohani Nasab M, Sadeghzadeh-Bazargan A, Goodarzi A. Effects of laser therapy on periorbital hyperpigmentation: a systematic review on current studies. Lasers Med Sci. 2021;36(9):1781-9.
34. Hedayat K, Karbakhsh M, Ghiasi M, Goodarzi A, Fakour Y, Akbari Z, Ghayoumi A, Gandhi AND. Quality of life in patients with vitiligo: a cross-sectional study based on Vitiligo Quality of Life index (VitiQoL). Health Qual Life Outcomes. 2016;14(1):1-9.
35. Vahideh L, Maryam G, Ali Asghar F, Azadeh G. Evaluation of nail characteristics in patients with vitiligo. Iranian J Dermatol. 2017;20(3):69-74.
36. Karbakhsh M, Hedayat K, Goodarzi A, Ghiasi M, Gandhi AND. Social participation in vitiligo patients and its association with quality of life. Iranian J Dermatol. 2021;24(1):6-10.
37. Yazdanian N, Muzaffarpur S, Goodarzi A. Phosphodiesterase inhibitors and prostaglandin analogues in dermatology: a comprehensive review. Dermatol Ther. 2020;12:e14669.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}