


Afsaneh Sadeghzadeh-Bazargan1; Masoumeh Roohaninasab1; Farnoosh Seirafianpour2; Mahsa Shemshadi1; Arezoo Mohammadi2; Samaneh Mozafarpoor3; Azadeh Goodarzi1
Submitted on: 02/10/2021
Approved on: 12/06/2022
Financial support: None
Conflict of interest: None
How to cite this article: Sadeghzadeh-Bazargan A, Roohaninasab M, Seirafianpour F, Shemshadi M, Mohammadi A, Mozafarpoor S, et al. A systematic review and meta-analysis on the association between androgenic alopecia and the risk of metabolic syndrome. Surg Cosmet Dermatol. 2022;14:e20220098.
This study conducted a systematic review of studies on the relationship between androgenic alopecia and metabolic syndrome. We performed a comprehensive review of databases including PubMed, Web of Knowledge, Google Scholar, Scopus, and Embase, and extracted relevant articles published from 2010 to 2018. The case reports, review articles, or studies lacking full-text articles were excluded. We examined nine studies for the meta-analysis step. The results showed a significant relationship between alopecia and metabolic syndrome (OR = 2.81; CI 95% = 2.16-3.66; I2 = 73%; P = 0.0003). There is a significant correlation between androgenic alopecia and metabolic syndrome.
Keywords: Alopecia; Systematic review; Metabolic syndrome; Hair diseases; Insulin resistance; Review hair
Androgenetic Alopecia (AGA) is a type of alopecia that shows hair thinning and loss in the frontal and central regions of the head or the vertex.1
According to evidence, 50% of men and women suffer from androgenic alopecia.2 AGA mainly affects people in the third and fourth decades of life but can occur any time after puberty and is more common in men than women. Also, the pattern of hair loss is different between the sexes.3
The etiology of AGA is multifactorial. Two fundamental changes occur in the hair cycle causing the condition: first, the hair anagen phase decreases, producing vellus and miniaturized hairs; second, the distance between the telogen and anagen phases increases, resulting in an increased number of empty hair follicles.4 Dihydrotestosterone (DHT) is a major factor in AGA pathogenesis. Five-alpha reductase enzyme converts testosterone to DHT. There are two types of 5-alpha reductase enzymes: type 1 and type 2. Type-2 5-alpha reductase plays an essential role in AGA. DHT binds to androgen receptors in the dermal papilla of the hair follicle, inhibits adenyl cyclase, and activates the genes responsible for transforming terminal hair to vellus hair in the anagen phase, resulting in empty follicles.5,6 Excess insulin and insulin resistance decrease the sex hormone-binding globulin levels and lead high free testosterone levels.7-9An increased serum androgen level also causes hypertension through the androgen receptors in the arterial endothelium, causing the proliferation and hyperplasia of smooth muscle cells in the arteries and contracting the lumen leading to high blood pressure.10,11 Also, microvascular disorders and follicular hypoxia decrease the number of hair follicles.12
Studies on the effects of androgens on the serum lipid index show that anabolic steroids such as testosterone cause decreased HDL, increased LDL, hyperlipidemia, and coronary artery disease.13 Research show that androgenic alopecia is a risk factor for insulin resistance and type-2 diabetes mellitus in men.13,14 Insulin resistance and high blood insulin levels are also risk factors for cardiovascular disease.15 Metabolic syndrome consists of insulin resistance, obesity, dyslipidemia, and hypertension, increasing the risk of cardiovascular diseases, stroke, and diabetes.16-18 Studies show that some dermatologic conditions and metabolic syndrome are correlated,19 but there is still controversy about the association between AGA and metabolic syndrome.7,8
The classic pattern of hair loss in men involves the frontal, temporal, and vertex regions of the scalp, while the hair on the parietal and occipital areas remains.1 Female Pattern Hair Loss (FPHL) appears first as thinning and then as hair loss around the ear. However, some women experience other configurations, such as centralized, Christmas tree, or male patterns. The scattered pattern is graded using the Ludwig scale, the centralized pattern using the Olsen scale, and the male pattern using the Hamilton-Norwood scale to assess AGA.3
The present study systematically reviewed studies on the relationship between AGA and metabolic syndrome.
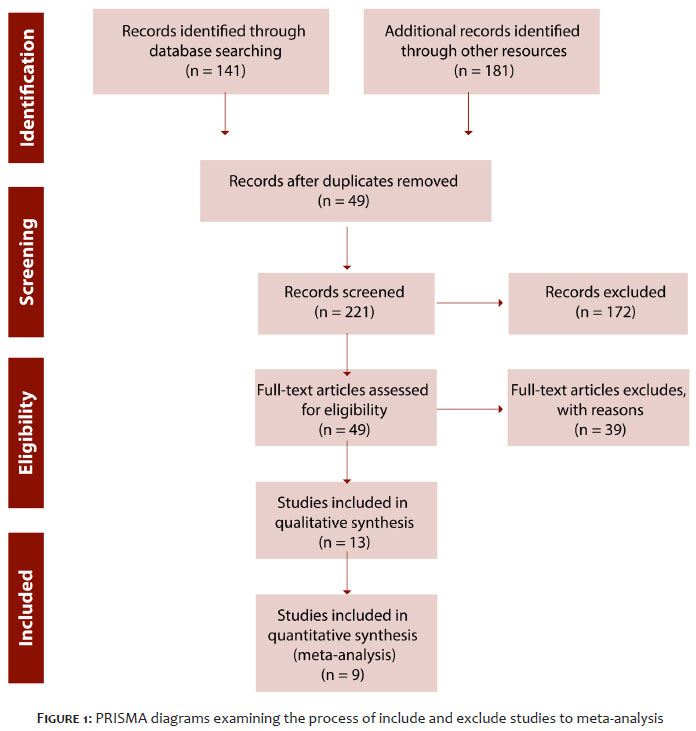
All the design steps were based on the PRISMA guidelines and the study sought to answer the question of whether the prevalence of the metabolic syndrome is higher in androgenic alopecia patients than in healthy controls.
We conducted a comprehensive review of databases including PubMed, Web of Knowledge, Google Scholar, Scopus, and Embase, and extracted pertinent articles.
The keywords used to find the articles included: Metabolic syndrome, central obesity, high blood pressure, high blood sugar, high serum triglycerides, low serum high-density lipoprotein, and androgenic alopecia.
The search strategy for PubMed was: (Metabolic syndrome) OR (central obesity) OR (high blood sugar) OR (high serum triglycerides) OR (low serum high density lipoprotein) AND (androgenic alopecia) AND (“2010/01/01” [PDat]: “2018/12/31” [PDat])
After extracting pertinent articles from the databases, we entered all of them into Endnote and removed the duplicates. Subsequently, two researchers selected the articles independently, and whenever there was disagreement about the selections for the final review, a third researcher was recruited to make the final decision.
This study included all articles published in English from 2010 to 1018 on patients with androgenic alopecia examined in terms of metabolic syndrome. Case reports, review articles, or studies lacking full-text articles were excluded.
STATA version 13.2 and Metan software were used to determine the prevalence of the condition. The pooled odds ratio was finally calculated, and the result was determined based on a 95% confidence interval (CI). The heterogeneity of the results of the studies was determined based on I2 statistics and P-value. Publication bias was also determined based on a funnel plot graph and Egger test.
There was a significant relationship between metabolic syndrome and alopecia. This result is contrary to the findings of some studies, perhaps because these other studies had not appropriately examined the confounding factors. The odds ratio (OR) of 2.81 shows that androgenic alopecia is a risk factor for metabolic syndrome. The incidence of metabolic syndrome was 43% to 51% in the groups with androgenic alopecia and 20% to 28% in the healthy controls.
Figure 1 shows the selection process for the databases.
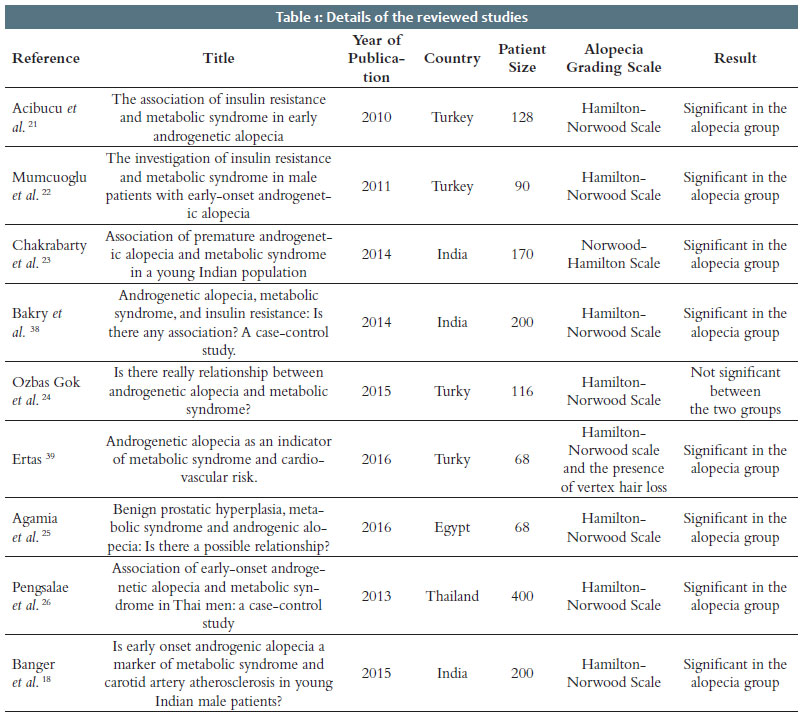
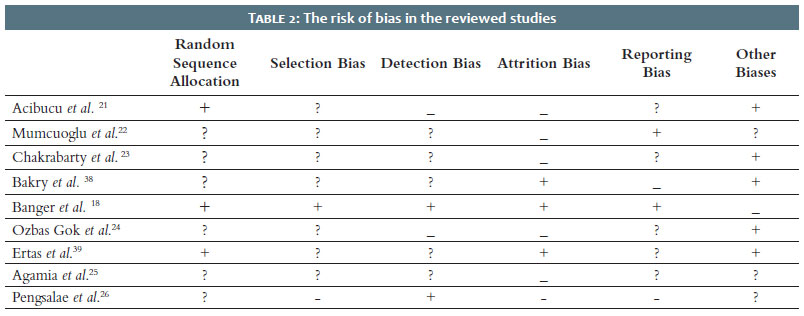
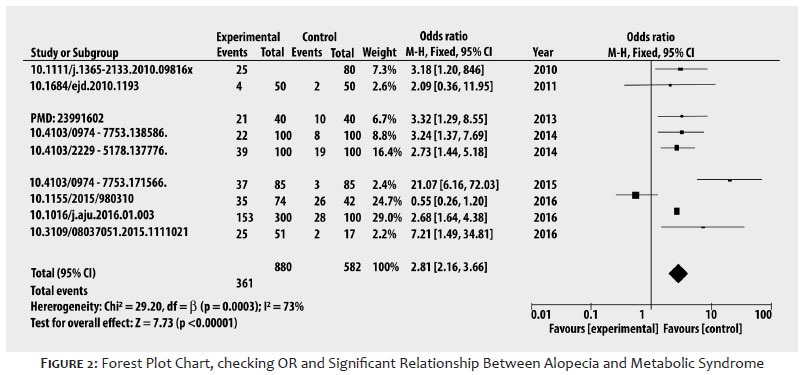
The meta-analysis included a total of nine studies. The total sample size of the studies was 1,452, and 880 cases had AGA. Table 1 presents the list of studies included in the meta-analysis. Table 2 shows the risk of bias in the studies. We used a forest plot chart to calculate the numerical results of the studies (Fig. 2). Based on this chart, the results showed a significant relationship between alopecia and metabolic syndrome (OR = 2.81; 95% CI = 2.16-3.66; I2 = 73%; P = 0.0003).
Figure 2: The forest plot chart for examining the OR and significance of the relationship between alopecia and metabolic syndrome.
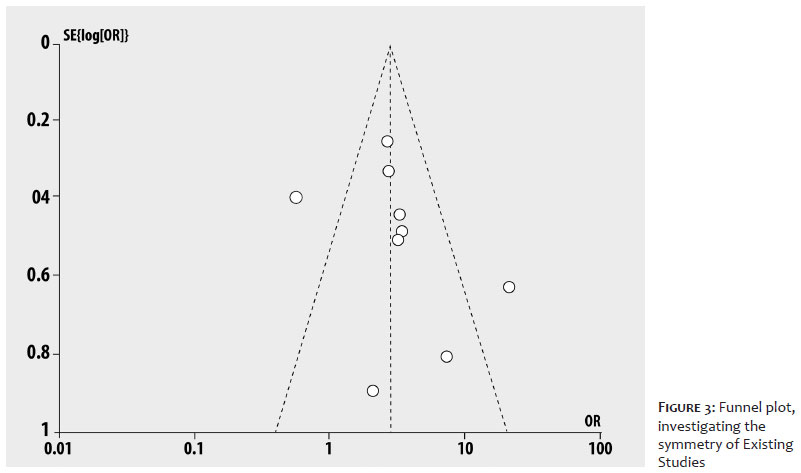
The funnel plot chart was used to investigate publication bias. As shown in figure 3, the studies are reasonably accurate, and there is no significant publication bias.
Figure 3: The funnel plot investigating the symmetry between the studies
Just two review studies have been conducted on metabolic syndrome and endogenous alopecia, and both confirm the results of our analysis. According to these analyses, there is a significant correlation between androgenic alopecia and metabolic syndrome.
In 1972, Cotton et al.20 showed a significant relationship between hair loss and cardiovascular diseases for the first time. In 2010, Acibucu et al.21 revealed, assessing 168 patients, that the probability of metabolic syndrome was 2.7 times higher in the AGA group than in the control group. The main problem of their study was the small sample size in the control group, although they showed significant intergroup correlations.21 In 2011, in Turkey, Mumcuoglu et al.22 examined insulin resistance and metabolic syndrome in men with early androgenic alopecia and showed that insulin resistance-related diseases and coronary artery diseases are more common in men with androgenic alopecia. This study included 50 men (18-30 years) with AGA ≥3 on the Hamilton-Norwood scale and BMI <27 and 40 men matched in weight and age. According to the results, high Homeostatic Model Assessment for Insulin Resistance (HOMA-IR) and Fasting Insulin Resistance Index (FIRI) scores indicate that men with AGA have insulin resistance.22 In a 2014 case-control study, Chakrabarty et al.23 examined the frequency of metabolic syndrome in people with primary AGA at a cognitive therapy clinic in Bangalore, India. They assessed 85 cases of AGA and 85 matched controls using the Norwood-Hamilton scale to evaluate the degree of AGA. The study used the Chi-square test to compare the ratios between the groups and compared the means between the subjects with metabolic syndrome and the controls using the independent t-test.
AGA was associated with metabolic syndrome in Indian men younger than 30 years old (P<0.001), but the severity of AGA was not correlated with metabolic syndrome. A 2015 case-control study by Banger et al.18 in India examined the clinical characteristics of AGA and the presence of metabolic syndrome and carotid artery atherosclerosis in men with early AGA and compared the results against a control group. The samples consisted of 100 men aged 18-35 years with AGA and several healthy controls; 22% of the patients with early androgenic alopecia met the criteria for metabolic syndrome compared to 8% in the control group. Nonetheless, there was no significant difference in the mean cholesterol levels. The research found an atherosclerotic plaque in two patients in the case group and no plaque in the control group.
Another case-control study by Ozbas Gok S. et al.24 in 2015 in Turkey assessed 74 men with AGA and 42 male controls. Of the 74 male AGA patients (age range of 20-50 years, mean age of 32.14 years), 24 were in stage 2, 26 in stage 3, 17 in stage 4, 1 in stage 5, and 5 were in stage 7. In the case group, 35 out of 74 individuals had metabolic syndrome. However, 26 out of the 42 subjects in the control group were affected. There was no significant difference in metabolic syndrome prevalence between the AGA patients and the control group (P=0.135). Among the studied parameters, only systolic blood pressure was significantly higher in the AGA group than in the control group. 24A study by Agamia et al.25 in Egypt in 2016 found a significant association between benign prostatic hyperplasia (BPH) and metabolic syndrome with AGA: the risk of metabolic syndrome was 2.68 times higher in the patients with androgenic alopecia. Androgenic changes in men’s bodies also increase the chance of developing prostate cancer.25 A study by Pengsalae et al.26 in Thailand in 2013 evaluated the association between androgenic alopecia and metabolic syndrome in Thai men. The research selected 80 male subjects, including 40 with early diagnosis of AGA (before 35 years of age) and 40 controls without alopecia. The patients with early androgenic alopecia were 3.48 times more likely to have metabolic syndrome than the control group (P =0.015, OR = 3.48, 95% CI = 1.25-9.75). Pengsalae et al.26 found a significant association between androgenic alopecia and metabolic syndrome. Also, they observed a correlation between the severity of AGA and metabolic syndrome (P= 0.629). They concluded that the early detection of metabolic syndrome in this population might be helpful in preventing cardiovascular diseases. 26A study in South Korea by Yi et al.27 in 2012 using the Norwood scale for men and the Ludwig scale for women examined a total of 3,408 individuals (1,707 men and 1,701 women) from January 2008 to February 2010. The relationship between AGA and all five metabolic syndrome components (waist circumference, triglycerides, high-density lipoprotein, blood glucose, and blood pressure) was statistically non-significant.
When multiple regressions were used to adjust for age, family history, and smoking status, there was no significant relationship between the prevalence of metabolic syndrome and AGA in the male group. In contrast, there was a statistically significant relationship between the prevalence of metabolic syndrome and AGA in the female group. A 2010 study by Acibucu et al.21 in Singapore assessed the frequency of insulin resistance, hyperinsulinemia, and metabolic syndrome in patients with androgenic alopecia. The study analyzed 80 patients with primary AGA and 48 healthy controls. The results showed that the difference in insulin resistance between the groups was statistically significant, as this index was higher in patients with preterm AGA compared to the healthy controls. Also, the incidence of metabolic syndrome was significantly higher in the AGA group than in the control group. The study showed that the prevalence of insulin resistance and metabolic syndrome increases in patients with AGA.21 A 2010 study by Su L. H. et al. in Taiwan evaluated the relationship between metabolic syndrome and androgenic alopecia in 740 individuals aged 40 to 91 years.6 It used the Norwood scale to evaluate the rate of hair loss. The research collected data on the components of metabolic syndrome and other possible risk factors, and the results showed a significant relationship between AGA and metabolic syndrome (OR= 1.67, 95% CI= 1.01-2.74) as well as a significant relationship between AGA and the number of components of the metabolic syndrome (OR= 1.21, 95% CI= 1.03-1.42). Among the components of the metabolic syndrome, high-density lipoprotein cholesterol (HDL-C) was identified as the most important factor associated with AGA (OR= 2.36, 95% CI= 1.41-3.95; P= 0.001). This finding may have significant implications for the detection of metabolic syndrome in patients with moderate or severe AGA.6 A 2016 cross-sectional study by Gopinath H. et al.17 in India, examined the association between metabolic syndrome and early androgenic alopecia in men aged 18-55 years. The research included 85 cases with clinically diagnosed early-onset (less than 35 years) androgenic alopecia (Norwood III) plus 85 controls without androgenic alopecia. Metabolic syndrome was observed in 19 (22.4%) patients with androgenic alopecia and eight (4.9%) controls (P = 0.021). Abdominal obesity, hypertension, and low-density lipoprotein levels were higher in patients with androgenic alopecia compared to the controls.17 A 2014 study by Eckel et al.28 in India evaluated the link between metabolic syndrome and insulin resistance in patients with AGA. It recruited 100 men with stages III-VII AGA based on the Hamilton-Norwood scale and 100 controls of the same sex and age. They observed a significant correlation between AGA and metabolic syndrome (P = 0.002) and between AGA and IR (P<0.001).
There are many articles on the rise regarding the significant association between dermatologic disorders, metabolic syndrome, and its correlated laboratory markers and also possible logical adjunctive therapeutic options, especially psoriasis, acne, androgenic alopecia, acanthosis nigricans, hidradenitis suppurativa, and lichen planus.19,29-42 This systematic review and meta-analysis focused on the association between androgenic alopecia and metabolic syndrome.
The authors would like to thank the staff of the Rasool Akram Medical Complex Clinical Research Development Center (RCRDC), specially Mrs Farahnaz Nikkhah, for their technical assistance in editing and improving quality of the paper.
Abbreviations:
AGA: Androgenic Alopecia
DHT: Dihydrotestosterone
FPHL: Female Pattern Hair Loss
HOMA-IR: Homeostatic Model Assessment for Insulin Resistance
FIRI: Fasting Insulin Resistance Index; BPH: Benign Prostatic Hyperplasia
HDL-C: High-Density Lipoprotein CholesterolReview criteria:
• This systematic review was conducted using five databases to assess the relationship between androgenic alopecia (AGA) and metabolic syndrome.
• This systematic review adheres to the PRISMA guidelines. Two independent reviewers extracted data, and an expert epidemiologist performed the meta-analysis.
Implications for clinical practice:
• According to the results of this study, there was a significant relationship between metabolic syndrome and androgenic alopecia;
• Androgenic alopecia could be a risk factor for metabolic syndrome;
• The incidence of metabolic syndrome was 43% to 51%in the groups with androgenic alopecia and 20% to 28% in the healthy groups.
Afsaneh Sadeghzadeh-Bazargan 0000-0003-1102-6241
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Masoumeh Roohaninasab 0000-0002-2862-6422
Approval of the final version of the manuscript; preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Farnoosh Seirafianpour 0000-0003-3794-6206
Approval of the final version of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Mahsa Shemshadi 0000-0002-6912-0532
Author's Contribution: Statistical analysis; approval of the final version of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Arezoo Mohammadi 0000-0002-8881-6340
Approval of the final version of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Samaneh Mozafarpoor 0000-0001-9417-4295
Statistical analysis; approval of the final version of the manuscript; data collection, analysis and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Azadeh Goodarzi 0000-0002-1249-4429
Statistical analysis; approval of the final version of the manuscript; preparation and writing of the manuscript; data collection, analysis, and interpretation active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Habif T. A color guide to diagnosis and therapy. Clin Dermatol. 2nd ed. ST Louis: Mosby Co; 2004.
2. Berker D, Messenger AG, Sinclair RD. Disorders of hair. Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook’s textbook of dermatology Massachusetts. New Jersey: Blackwell Science Ltd; 2004. p. 63.
3. Wolff K, Johnson RA. Fitzpatrick's color atlas and synopsis of clinical dermatology. New York: McGraw Hill; 2009.
4. Hoffmann R. Steroidogenic isoenzymes in human hair and their potential role in androgenetic alopecia. Dermatol. 2003;206(2):85-95.
5. Matilainen V, Laakso M, Hirsso P, Koskela P, Rajala U, Keinänen-Kiukaanniemi S. Hair loss, insulin resistance, and heredity in middle-aged women. A population-based study. J Cardiovasc Risk. 2003;10(3):227-31.
6. Su LH, Chen TH. Association of androgenetic alopecia with smoking and its prevalence among asian men: a community-based survey. Arch Dermatol. 2007;143(11):1401-6.
7. Stough D, Stenn K, Haber R, Parsley WM, Vogel JE, Whiting DA, et al. Psychological effect, pathophysiology, and management of androgenetic alopecia in men. Mayo Clin Proc. 2005;80(10):1316-22.
8. Inui S, Itami S. Molecular basis of androgenetic alopecia: from androgen to paracrine mediators through dermal papilla. J Dermatol Sci. 2011;61(1):1-6.
9. Kapoor D, Goodwin E, Channer KS, Jones TH. Testosterone replacement therapy improves insulin resistance, glycaemic control, visceral adiposity and hypercholesterolaemia in hypogonadal men with type 2 diabetes. Eur J Endocrinol. 2006;154(6):899-906.
10. Bowles LL, Allen L. The development and demonstration of corneal vascularization in rats deficient in vitamin A and in riboflavin. J Nutr. 1946;32(1):19-35.
11. Bhat PV, Manolescu DC. Role of vitamin A in determining nephron mass and possible relationship to hypertension. J Nutr. 2008;138(8):1407-10.
12. Upton JH, Hannen RF, Bahta AW, Farjo N, Farjo B, Philpott MP. Oxidative stress-associated senescence in dermal papilla cells of men with androgenetic alopecia. J Invest Dermatol. 2015;135(5):1244-52.
13. Matilainen V, Koskela P, Keinänen-Kiukaanniemi S. Early androgenetic alopecia as a marker of insulin resistance. Lancet. 2000;356(9236):1165-6.
14. Starka L, Duskova M, Cermakova I, Vrbiková J, Hill M. Premature androgenic alopecia and insulin resistance. Male equivalent of polycystic ovary syndrome? Endocr Regul. 2005;39(4):127-31.
15. Hirsso P, Rajala U, Hiltunen L, Laakso M, Koskela P, Härkönen P, et al. Association of low-insulin sensitivity measured by quantitative insulin sensitivity check index with hair loss in 55-year-old men. A finnish population-based study. Diabetes Obes Metab. 2006;8(4):466-8.
16. Wu DX, Wu LF, Yang ZX. [Association between androgenetic alopecia and metabolic syndrome: a meta-analysis]. Zhejiang Da Xue Xue Bao Yi Xue Ban. 2014;43(5):597-601.
17. Gopinath H, Upadya GM. Metabolic syndrome in androgenic alopecia. Indian J Dermatol Venereol Leprol. 2016;82(4):404-8.
18. Banger HS, Malhotra SK, Singh S, Mahajan M. Is early onset androgenic alopecia a marker of metabolic syndrome and carotid artery atherosclerosis in young Indian male patients? Int J Trichology. 2015;7(4):141-7.
19. Nasiri S, Sadeghzadeh-Bazargan A, Robati RM, Haghighatkhah HR, Younespour S. Subclinical atherosclerosis and cardiovascular markers in patients with lichen planus: A case-control study. Indian J Dermatol Venereol Leprol. 2019;85(2):138-44.
20. Cotton SG, Nixon JM, Carpenter RG, Evans DW. Factors discriminating men with coronary heart disease from healthy controls. Br Heart J. 1972;34(5):458-64.
21. Acibucu F, Kayatas M, Candan F. The association of insulin resistance and metabolic syndrome in early androgenetic alopecia. Singapore Med J. 2010;51(12):931-6.
22. Mumcuoglu C, Ekmekci TR, Ucak S. The investigation of insulin resistance and metabolic syndrome in male patients with early-onset androgenetic alopecia. Eur J Dermatol. 2011;21(1):79-82.
23. Chakrabarty S, Hariharan R, Gowda D, Suresh H. Association of premature androgenetic alopecia and metabolic syndrome in a young Indian population. Int J Trichology. 2014;6(2):50-3.Ozbas Gok S, Akin Belli A, Dervis E. Is there really relationship between androgenetic alopecia and metabolic syndrome? Dermatol Res Pract. 2015;2015:980310. Epub 2015 Nov 4.
24. Agamia NF, Abou Youssif T, El-Hadidy A, El-Abd A. Benign prostatic hyperplasia, metabolic syndrome and androgenic alopecia: is there a possible relationship? Arab J Urol. 2016;14(2):157-62.
25. Pengsalae N, Tanglertsampan C, Phichawong T, Lee S. Association of early-onset androgenetic alopecia and metabolic syndrome in thai men: a case-control study. J Med Assoc Thai. 2013;96(8):947-51.
26. Yi SM, Son SW, Lee KG, Kim SH, Lee SK, Cho ER, et al. Gender-specific association of androgenetic alopecia with metabolic syndrome in a middle-aged korean population. Br J Dermatol. 2012;167(2):306-13.
27. Eckel RH, Alberti KG, Grundy SM, Zimmet PZ. The metabolic syndrome. Lancet. 2010;375(9710):181-3.
28. Stefanadi EC, Dimitrakakis G, Antoniou CK, Challoumas D, Punjabi N, Dimitrakaki IA, et al. Metabolic syndrome and the skin: a more than superficial association. Reviewing the association between skin diseases and metabolic syndrome and a clinical decision algorithm for high risk patients. Diabetol Metab Syndr. 2018;10:9.
29. Hallaji Z, Lajevardi V, Abedini R, Soleymani A, Goodarzi A, Salehi-Taleghani M, et al. Serum leptin levels in psoriatic patients with non-alcoholic fatty liver disease. Iran J Dermatol. 2016;19:125-30.
30. Abedini R, Goodarzi A, Saeidi V, Hosseini SH, Jadidnuri A, Salehi Taleghani M, et al. Serum homocysteine level, vitamin B12 levels, and erythrocyte folate in psoriasis: a case-control study. Int J Womens Dermatol. 2019;5(3):171-4.
31. Ehsani AH, Mortazavi H, Balighi K, Hosseini MS, Azizpour A, Hejazi SP, et al. Changes in body mass index and lipid profile in psoriatic patients after treatment with standard protocol of infliximab. Acta Med Iran. 2016;54(9):570-5.
32. Lajevardi V, Hallaji Z, Daklan S, Abedini R, Goodarzi A, Abdolreza M. The efficacy of methotrexate plus pioglitazone vs. methotrexate alone in the management of patients with plaque-type psoriasis: a single-blinded randomized controlled trial. Int J Dermatol. 2015;54(1):95-101.
33. Lajevardi V, Ghodsi S.Z, Daneshpazhooh M, Kazemi H, Aryanian Z, Goodarzi A. The relationship between body mass index and the severity of acne. Iran J Dermatol. 2014;17:13-7.
34. Behrangi E, Sadeghi S, Sadeghzadeh-Bazargan A, Goodarzi A, Ghassemi M, Sepasgozar S, et al. The effect of metformin in the treatment of intractable and late onset acne: a comparison with oral isotretinoin. Iran J Dermatol. 2019;22:47-52.
35. Ehsani A, Noormohammadpour P, Goodarzi A, Mirshams Shahshahani M, Hejazi SP, Hosseini E, et al. Comparison of long-pulsed alexandrite laser and topical tretinoin-ammonium lactate in axillary acanthosis nigricans: A case series of patients in a before-after trial. Caspian J Intern Med. 2016;7(4):290-3.
36. Aryanian Z, Shahabandaz H, Abdollahzadeh Sangrody M, Shirzadian A, Tirgartabari S, Bijani A, et al. Carotid doppler ultrasound evaluation in patients with lichen Planus. Iran. J. Dermatol. 2019;22:133-8.
37. Bakry OA, Shoeib MA, El Shafiee MK, Hassan A. Androgenetic alopecia, metabolic syndrome, and insulin resistance: is there any association? A case-control study. Indian Dermatol Online J. 2014;5(3):276-81.
38. Ertas R, Orscelik O, Kartal D, Dogan A, Ertas SK, Aydogdu EG, et al. Androgenetic alopecia as an indicator of metabolic syndrome and cardiovascular risk. Blood Press. 2016;25(3):141-8.
39. Ghassemi M, Hosseinchi S, Seirafianpour F, Dodangeh M, Goodarzi A. Non-alcoholic fatty liver and lipid profile status in patients with melasma: a case-control study. J Cosmet Dermatol. 2021;20(11):3656-60.
40. Qiu Y, Zhou X, Fu S, Luo S, Li Y. Systematic review and meta-analysis of the association between metabolic syndrome and androgenetic alopecia. Acta Derm Venereol. 2022;102:adv00645.
41. Lie C, Liew CF, Oon HH. Alopecia and the metabolic syndrome. Clin Dermatol. 2018;36(1):54-61.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}