


Laura Nunes Lopes; Roberta Akeme de Oliveira Sato; Clóvis Antônio Lopes Pinto; Juliana Arêas de Souza Lima Beltrame Ferreira; Célia Antônia Xavier de Moraes Alves
Submitted on: 24/01/2022
Approved on: 05/08/2022
Financial support: None
Conflict of interest: None
How to cite this article: Lopes LN, Sato RAO, Pinto CAL, Ferreira JASLB, Alves CAXM. NK/T cell lymphoma, nasal-type (rare, rapidly evolving, mutilating, and highly lethal lymphoid neoplasm): a case report. Surg Cosmet Dermatol. 2022;14:e20220126
NK/T cell lymphoma is a rare, aggressive, non-Hodgkin tumor that is closely related to the Epstein-Barr virus. It has a poor prognosis and poor response to treatments. We report the case of a 91-year-old woman with a history of injury in the nasal region for three months. Histological study showed diffuse infiltration of the dermis by small and atypical lymphoid cells and positive immunohistochemistry for Ki-67, CD30, and CD3 (cytoplasmic). Due to the fast growth of the lesion and the high morbidity of the neoplasm, the patient was referred to the hospital for assistance but died before starting treatment.
Keywords: Epstein-Barr Virus Infections; Lymphocytes; Medical oncology; Extranodal T-NK Cell Lymphoma; Lethal Midline Granuloma
NK/T cell lymphoma is a non-Hodgkin tumor commonly described in Asia and Latin America. It is rare (about 1% of cutaneous T-cell lymphomas), very aggressive, and closely related to the Epstein-Barr virus1,2,3,4 (the infection can happen before or simultaneously with the tumor genesis).2 The precursor cell has lymphoid lineage, and in 95% of cases, it comes from the NK cell (cytolytic function).2
It constitutes the group of non-mycosis fungoid/non-Sézary syndrome cutaneous lymphomas (10% of cases),4 with a rapid, mutilating, and highly lethal evolution (five-year survival rate <5%).1
The tumor is divided into non-nasal and nasal subtypes (former lethal midline granuloma2,3,4,5). It affects the nasal or nasopharyngeal region in 80% of cases.2,4 However, it can also involve the aerodigestive tract,4 testicles,5 muscles, and the uterus, or evolve contiguously to the orbit, salivary glands, and paranasal sinuses. Many non-nasal cases probably had their subclinical onset in the nose (primary site).2
It has a poor prognosis and poor response to treatments.
A 91-year-old woman, white, hypertensive, presented a history of a nasal lesion for three months and weight loss (5 kg in 30 days). An erythematous and edematous lesion was found in the left nasal region, with local ulceration and an area of necrosis, at the initial dermatological examination. The diagnostic hypotheses of invasive squamous cell carcinoma (SCC), NK/T cell lymphoma, leishmaniasis, and mucormycosis were raised. The investigation was then started.
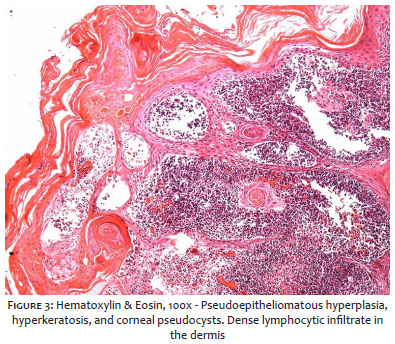
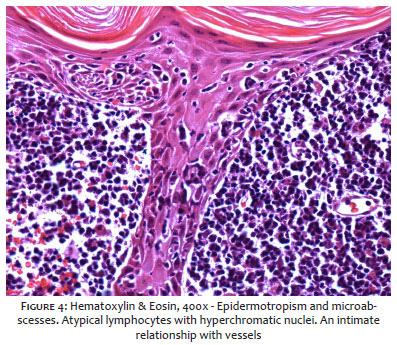
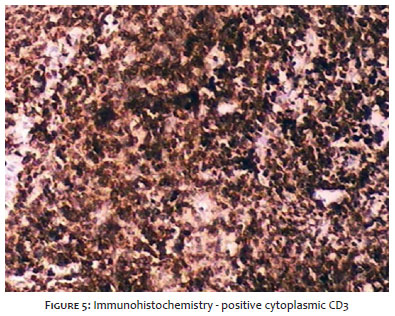
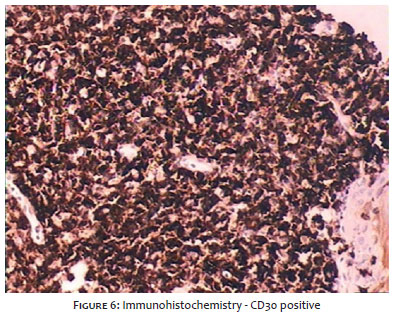
One week after the initial evaluation, the lesion worsened considerably in size and appearance, and antibiotic therapy was then introduced. Laboratory tests showed hypochromic and microcytic anemia, leukocytosis, thrombocytosis, and increased ESR and CRP (28 and 138, respectively). Cranial tomography revealed an area of dermal ulceration from the left nasal/malar region to the adjacent bone limits without signs of invasion, chronic osteomyelitis, or organized collections. An anatomopathological study (Figures 3 and 4) showed diffuse infiltration of the dermis by small and atypical lymphoid cells. Immunohistochemistry (Figures 5 and 6) was positive for Ki-67 (estimated at 80%), CD30, and CD3 (cytoplasmic), confirming the diagnosis of high-grade (CD30+) T lymphoma (CD3e+) or NK/T lymphoma nasal-type.
Due to the rapid evolution of the neoplasm (Figures 1 and 2) and the patient’s clinical worsening (decrease in general condition, adynamia, difficulty swallowing), she was referred to the hospital for support measures and palliative care, under the supervision of the Dermatology, Clinical Oncohematology, and Head and Neck Surgery (HNC) teams. The patient died on the fifth day of hospitalization.
Nasal-type NK/T lymphoma may present clinically with epistaxis, nasal tumor with perilesional edema, and hard palate perforation (causing communication between the nasal and oral cavities). Also, the patient may complain of nasal obstruction and/or secretion.4 The case reported manifested similarly to the cases described in the literature, focusing on the extensive area of necrosis.
The anatomopathological study revealed infiltration of atypical lymphoid cells, neutrophils, and eosinophils, characterizing the so-called polymorphic reticulosis.2,5 Another histopathological characteristic of this tumor is its close relationship with blood vessels (wall invasion and vascular occlusion).2,3
Immunohistochemistry is generally positive for CD3 (surface: negative; cytoplasmic epsilon chain: positive), CD56, CD2, and cytotoxic molecules (granzyme B, perforin, and TIA1).2,3,5,6,7 Positive Ki-67 indicates a high rate of cell proliferation.
The quantification of EBV-DNA in blood plasma (prognostic indicator) and in situ hybridization to assess tumor medullary bone invasion by detecting the virus genetic material can also be used.2,3,5
Regarding imaging tests, in addition to computed tomography, Pet-scan (PET-CT)5,7,8 and soft tissue magnetic resonance imaging (MRI) are considered, mainly to assess extension and complications. PET-CT is especially important in non-nasal cases as the absence of hypermetabolic areas (the tumor lymphoid cell has a high avidity for 18-fluorodeoxyglucose) in the nasal/nasopharyngeal region excludes the possibility that the primary site is the face.2
Regarding treatment,2,5,6,8,9 combination of radiotherapy and chemotherapy is considered the gold standard. However, new protocols and therapies (targeted therapy, stem cell transplantation, immunotherapy targeting the EBV, among others) have been discussed.6,9 In the case described, as in many others of this type of lymphoma, there was no time for treatment, only comfort measures.
Laura Nunes Lopes 0000-0001-5268-0624
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Roberta Akeme de Oliveira Sato 0000-0001-6449-8870
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Clóvis Antônio Lopes Pinto 0000-0003-1711-0081
Author’s contribution: Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Juliana Arêas de Souza Lima Beltrame Ferreira 0000-0001-7338-3442
Author’s contribution: Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Célia Antônia Xavier de Moraes Alves 0000-0002-8421-8837
Author’s contribution: Approval of the final version of the manuscript; study design and planning; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Bolognia JL, Jorizzo JL, Rapini RP, editors. Dermatology. 2ª ed. St. Louis: Mosby Elsevier; 2008.
2. Tse E, Kwong YL. Diagnosis and management of extranodal NK/T cell lymphoma nasal type. Expert Rev Hematol. 2016;9(9):861-71.
3. Haverkos BM, Pan Z, Gru AA, Freud AG, Rabinovitch R, Xu-Welliver M, et al. Extranodal NK/T Cell Lymphoma, Nasal Type (ENKTL-NT): an update on epidemiology, clinical presentation, and natural history in North American and European cases. Curr Hematol Malig Rep. 2016;11(6):514-27.
4. Moreno L, Ramos-Valencia L, Parra-Charris J, Ángel-Obando R. Accurate diagnose and management of advanced nasal type extranodal NK/T cell lymphoma. A case report. Case Reports. 2017;3(1):42-8.
5. Tse E, Kwong YL. NK/T-cell lymphomas. Best Pract Res Clin Haematol. 2019;32(3):253-61.
6. Chiattone CS. Linfoma extranodal de células NK/T tipo Nasal. Rev Bras Hematol Hemoter. 2009;31(Suppl. 2):26-9
7. Jhuang JY, Chang ST, Weng SF, Pan ST, Chu PY, Hsieh PP, et al. Extranodal natural killer/T-cell lymphoma, nasal type in Taiwan: a relatively higher frequency of T-cell lineage and poor survival for extranasal tumors. Hum Pathol. 2015;46(2):313-21.
8. Chi KY, Shen HN. Extranodal natural killer T-Cell lymphoma. N Engl J Med. 20206;382(6):562.
9. Yamaguchi M, Suzuki R, Oguchi M. Advances in the treatment of extranodal NK/T-cell lymphoma, nasal type. Blood. 2018;131(23):2528-40.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}