


Rodrigo Scabora1; João Gabriel Rodrigues Alberti1; Carolina Scaff Haddad Bartos2; Lucia Mioko Ito1; Ayrton Roberto Pastore1; Deborah Krutman Zveibil3
Submitted on: 30/11/2021
Approved on: 20/07/2022
Financial support: None
Conflict of interest: None
How to cite this article: Scabora R, Alberti JGR, Bartos CSH, Ito LM, Pastore AR, Zveibil DK. Clinically ulcerated and granulomatous pilomatricoma in a cutaneous vaccination site: case report. Surg Cosmet Dermatol. 2022;14:e20220112
Pilomatricoma is a benign skin tumor derived from the hair follicle. It has a varied etiology, and the traumatic one is often described as a triggering factor. The surgical treatment is curative and, therefore, the choice. We report a case of an atypical clinical presentation pilomatricoma – an ulcerated nodule topped by a central hematic crust, with peripheral telangiectasias probably triggered by the HPV vaccination. The ultrasound examination suggested the possibility of a chronic inflammatory granuloma, although the histopathological examination was definitive and confirmed the diagnosis of pilomatricoma.
Keywords: Papillomavirus vaccines; Hair follicle; Ultrasonography, Doppler; Skin neoplasms
Pilomatricoma represents about 1% of benign skin tumors and derives from the hair follicle matrix. They are solitary tumors, usually painless and well-delimited. Clinically, it is associated with many differential diagnoses, and complementary tests are necessary for diagnostic confirmation.1 Ultrasonography (USG) of the skin and soft tissues can be helpful, but confirmation requires an anatomopathological examination. The pathogenesis is still poorly understood, but the appearance of the lesion is often associated with local trauma. Nonetheless, its association with vaccination, and the atypical, ulcerated, with extrusion of material through the center of the lesion, is infrequent, with rare cases reported.
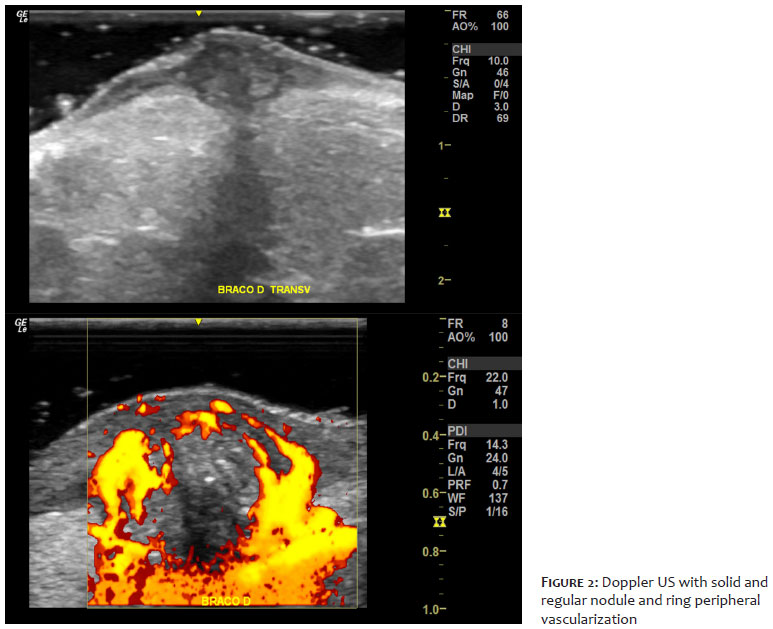
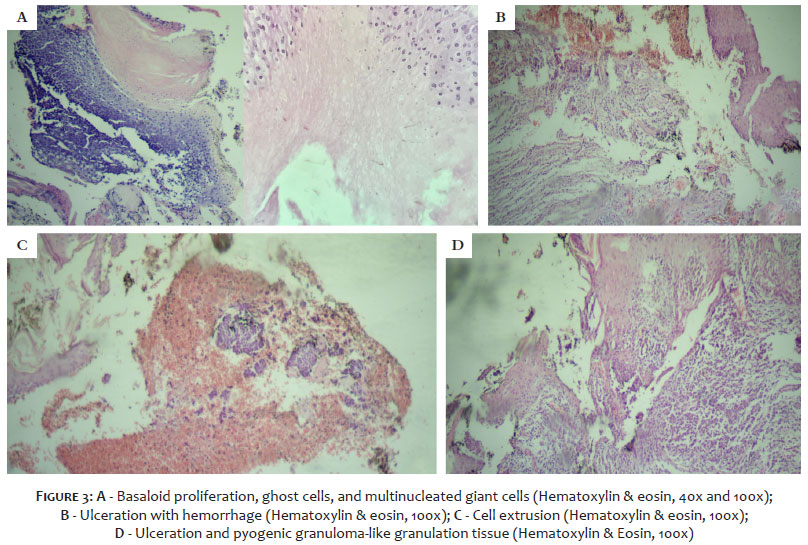
An 11-year-old female patient, sought medical assistance due to a complaint of a wound in her right arm for more than a year. The lesion appeared one month after the HPV vaccination at the injection site. She reported that the lesion progressively evolved with an increase in diameter and sporadic drainage of purulent secretion and nonspecific material through its central portion. The patient received several treatments - topical (association of neomycin and bacitracin, ketoconazole, betamethasone, and collagenase) and systemic (azithromycin and cephalexin) - with no resolution. On clinical examination, she presented an erythematous nodule measuring 1.5 cm in diameter, with firm consistency, ulceration, and central serohematic crust, painless on superficial palpation but painful on deep palpation. The lesion had some peripheral telangiectasia and a small and discrete superficial bluish area, (Figure 1). The hypothesis of pyogenic granuloma was raised, and skin and soft tissue USG with Doppler were requested for further diagnostic investigation. The examination revealed the presence of a solid nodule, predominantly hypoechogenic, heterogeneous, and with regular contours, affecting the epidermis, dermis, and hypodermis (Figure 2). Color Doppler showed marked peripheral vascularization in the shape of a ring and inside the nodule. The diagnostic impression was of possible chronic granulomatous disease. We performed a ellipticall excision. The anatomopathological examination showed the presence of basaloid cells, ghost cells, and multinucleated giant cells, as well as epidermal ulceration with cell extrusion, compatible with the diagnosis of ulcerated pilomatricoma associated with a chronic granulomatous inflammatory process (Figure 3). The patient evolved with complete resolution of the condition after surgery.
Pilomatricoma, or calcifying epithelioma of Malherbe, is a rare benign tumor of the hair follicle matrix. It is usually located in the head and neck region and presents as a firm, solitary, well-defined, slow-growing dermal or subcutaneous mass.
Epidermal ulceration may accompany the clinical presentation of the lesion.2,3,4 Different clinical forms of pilomatricoma are described, such as anetodermic, proliferating, pigmented, familial, and perforating.2,4 The latter presentation can be considered in the atypical case reported, both from the clinical and histological perspectives.
The tumor is frequent in the first and second decades of life, and its pathogenesis is uncertain. Mutations in the Wnt signaling pathway and genetic syndromes may be associated: the relationship with Turner syndrome and myotonic dystrophy is more common, but the association with Gardner syndrome, MUTYH-associated polyposis (MAP), Rubinstein-Taybi syndrome, Sotos syndrome, and gliomatosis cerebri may also occur.2 Previous events, such as vaccination, rarely induce the appearance of pilomatricoma. Long-term inflammation, delayed healing response, and the antigens used in the vaccine are possibly linked to the uncertain pathogenesis of this disease.3
Although described since 1880, these tumors are often underdiagnosed.2 The variety of differential diagnoses includes dermoid or epidermoid cysts, calcified lymph nodes or hematomas, hemangiomas, and parotid gland tumors.3 Combined with its low prevalence, which varies from 0.001% to 0.0031%, the suspected lesion can lead to diagnostic and therapeutic errors.2 Studies indicate that preoperative diagnosis was correct in 30% to 50% of cases.7
The typical clinical presentation of pilomatricoma corresponds to a firm erythematous nodule with a smooth surface in a hairy region, sometimes accompanied by a tiny bluish surface area. Histologically, the presence of basaloid cells and “ghost cells” is observed, associated or not with a granulomatous response and local calcification, which varies according to the evolutionary stage of the tumor.2,3,5 However, the presence of ulceration with the elimination of material through the lesion, combined with the histological presence of epidermal ulceration with extrusion of eosinophilic tumor cells, may configure a rare, atypical, and infrequent form of pilomatricoma, called perforating pilomatricoma, as considered in this case.4
Color Doppler ultrasound helps diagnose nodular skin lesions as it shows the tumor’s position, depth, and degree of calcification. It is an accessible and non-invasive tool capable of increasing the diagnostic accuracy of several dermatoses, determining the degree of local vascularization, and delimiting the tissue planes affected by the lesion. This exam allows for better surgical planning and preparation for the possibility of intraoperative hemorrhage. The sonographic findings regarding pilomatricoma correspond to ovoid, well-defined, hypoechoic masses with internal hyperechoic foci and peripheral hypoechoic edges. Completely echogenic masses with posterior acoustic shadowing in the subcutaneous tissue are observed.2,5,6 The blood flow distribution pattern visualized on color doppler helped differentiate pilomatricoma from hemangiomas and other vascular malformations.2
To date, there are five published cases of post-vaccination pilomatricoma on MEDLINE (PubMed). However, there is no case published in this database of perforating pilomatricoma after the application of vaccines, nor even pilomatricoma occurring after HPV vaccination, which are unique and pioneering characteristics of this case report.
Given the low prevalence and similarity of pilomatricoma to other skin pathologies, clinical and histological examinations, associated with Doppler ultrasound, are extremely important in aiding diagnosis and therapeutic management, especially concerning surgical planning of a highly vascularized lesion. Pilomatricoma should be included as a differential diagnosis in chronic nodular lesions developed at sites of trauma, such as vaccination.
Rodrigo Scabora 0000-0002-3153-3980
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
João Gabriel Rodrigues Alberti 0000-0001-6495-8419
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Carolina Scaff Haddad Bartos 0000-0001-7601-2946
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Lucia Mioko Ito 0000-0001-9899-3036
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Ayrton Roberto Pastore 0000-0002-6607-0488
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Deborah Krutman Zveibil 0000-0002-3252-6192
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Fonseca R, Filho J, Araujo I, Filho A, Pereira N, Carvalho E, et al. Pilomatricoma: epitelioma calcificado de Malherbe. Rev Bras Cir Plást. 2012;27(4):605-10.
2. Jones CD, Ho W, Robertson BF, Gunn E, Morley S. Pilomatrixoma: a comprehensive review of the literature. Am J Dermatopathol. 2018;40(9):631-41.
3. Pirouzmanesh A, Reinisch JF, Gonzalez-Gomez I, Smith EM, Meara JG. Pilomatrixoma: a review of 346 cases. Plast Reconstr Surg. 2003;112(7):1784-9.
4. Endo M, Yamamoto T. A case of multiple perforating pilomatricomas. An Bras Dermatol. 2022;97(2):263-4.
5. Hague JS, Maheshwari M, Ryatt KS, Abdullah A. Proliferating pilomatricoma mimicking pyogenic granuloma. J Eur Acad Dermatol Venereol. 2007;21(5):688-9.
6. Hwang JY, Lee SW, Lee SM. The common ultrasonographic features of pilomatricoma. J Ultrasound Med. 2005;24(10):1397-402.
7. Roche NA, Monstrey SJ, Matton GE. Pilomatricoma in children: common but often misdiagnosed. Acta Chir Belg. 2010;110(2):250-4.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}