


Luciana Takata Pontes; Antonio Ruston
Submitted on: 02/02/2022
Approved on: 21/02/2022
Financial support: None
Conflict of interest: None
How to cite this article: Pontes LT, Ruston A. FUE hair transplantation: how I do it? Surg Cosmet Dermatol. 2022;14:e20220128.
Modern hair transplant is constantly evolving. We intend to demonstrate our techniques and methodologies, and especially to describe the dynamics of the entire surgical process of the FUE (Follicular Unit Extraction), technique, from the discussion of the surgical strategy with the patient and evaluation of the donor area to extraction and implantation. The dermatologist must understand the complexity of the procedure and the need for adequate training to achieve a good surgical result.
Keywords: Alopecia; Hair; Hair follicle; Transplant donor site
A hair transplant is not a simple procedure. Regardless of the technique, there is a need for a trained team and an apt and experienced surgeon to achieve better results.
Initially, it was performed using large flaps. Then, the technique evolved to grafts with larger punches. Now we refined the method to follicular unit transplants. Follicular unit (FU) identification as a particular structure of hair follicles was essential to achieve the most natural result.1
In the Follicular Unit Transplant (FUT), a strip of the scalp is removed from the occipital donor region, reaching the temporal regions, and the FUs are separated under the microscope. In the Follicular Unit Extraction (FUE) method, FUs are taken individually from the entire safe donor area where there is no risk of miniaturization. Punch diameters ranging from 0.8 mm to 1.0 mm are used in most cases. These microincisions heal by secondary intention, with no need for sutures.1
Modern hair transplant is constantly evolving, and we intend not only to demonstrate our techniques and methodologies but also to describe the dynamics of the FUE technique surgical process, from the discussion of the surgical strategy with the patient and evaluation of the donor area to extraction and implantation.
In the preoperative room, photos are taken with the hair long, first dry, and then wet to better assess the rarefaction area. The surgical strategy is discussed with the patient (such as hairline height and priority areas), aligning expectations with what is possible in each case.2 Then, the patient’s hair is shaved between 0.5 mm and 1.0 mm and new photos are taken (Figure 1). In case of rarefaction, only at the entrances (Norwood-Hamilton 2) can one opt for a military-style shave (Figure 2).
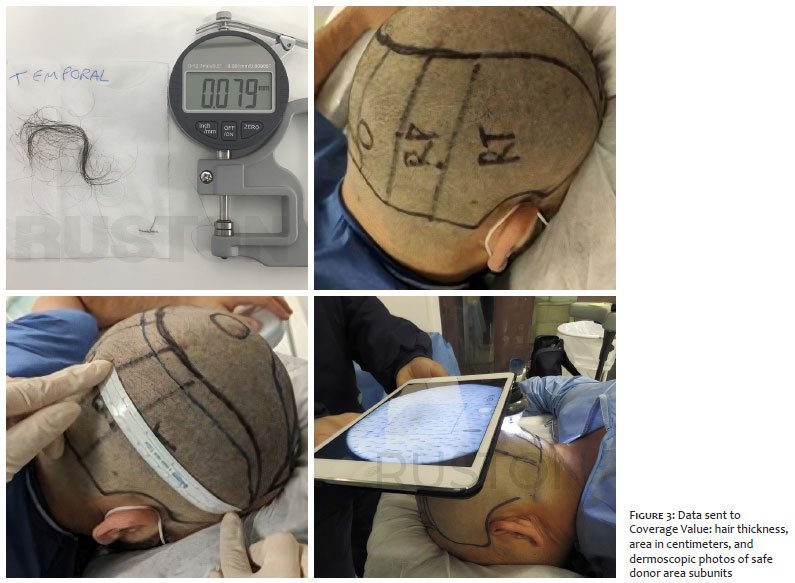
Hair samples are taken from the occipital, parietal, and temporal regions to assess the donor area. A digital micrometer is used to evaluate the thickness of these hairs (Figure 3) and calculate the Coverage Value (CV). The software determines how many FUs can be extracted without visible rarefaction of the donor area.
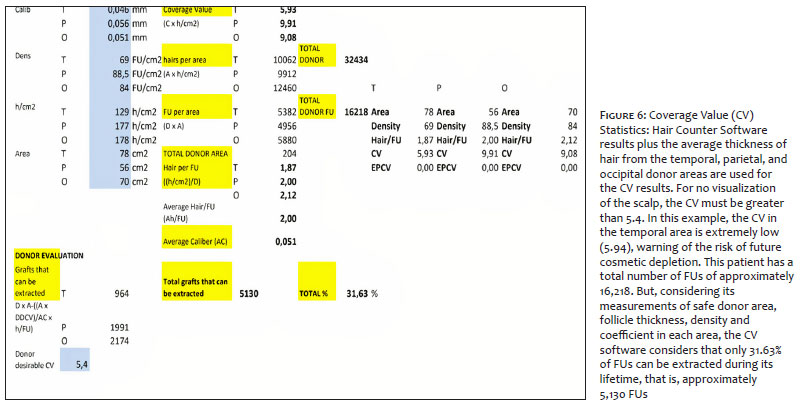
The area is divided into five subunits, and photographic documentation is conducted using a dermatoscope attached to a tablet (Figure 4). Both the measurement in centimeters and the photographs are sent to the Coverage Value Software (Asmed Hair Transplant, Istanbul). The approximate value of FUs/cm2 and hairs/cm2 in each subunit is calculated and a report is generated, providing information for management during extraction, such as the approximate value of FUs for future surgeries and regions where treatment be more aggressive without depletion of the donor area or cosmetic impairment (Figures 4 and 5).
Anesthetic infiltration and regional block are performed with 2% lidocaine with vasoconstrictor extremely slowly and associated with a vibrating stimulus to minimize discomfort.3 A tumescent solution is used both in the donor and recipient areas.
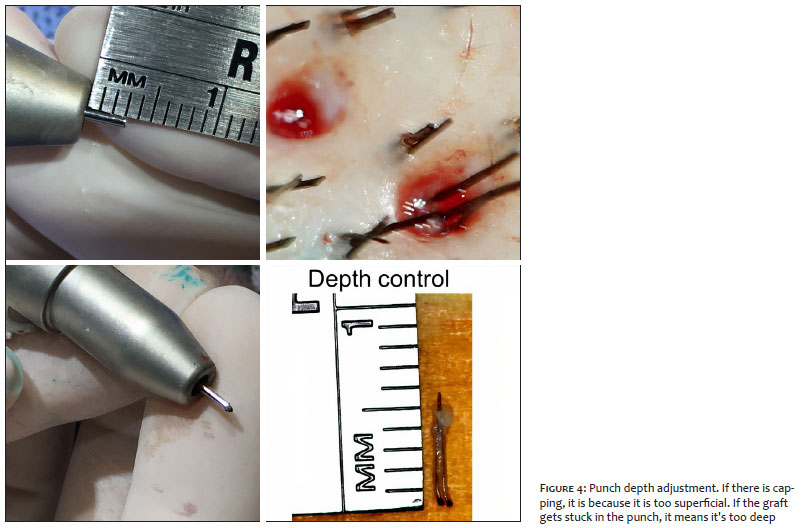
The first step is to decide the punch depth. We started the extraction with a depth of 3.0 mm to 3.5 mm. If there is capping (the epidermis is removed but the follicle remains trapped), probably the punch is too superficial (Figure 6). If the graft undergoes transection and gets stuck inside the punch, possibly the punch is too deep.4
The next step is to decide the best punch diameter. The choice will depend on the characteristics of the graft, such as the degree of waviness, the level of opening, and how the follicles are distributed in each follicular unit. We performed a test extraction of approximately 50 grafts with each one to evaluate the hair/UF ratio and the transection rate.5 For most patients, we used punches of 0.8 mm to 0.9 mm.
We started the procedure with the patient in the prone position to extract the occipital region. Then, we moved the patient laterally to extract the parietal and temporal regions.
We use the device Trivellini Mamba FUE (Trivellini Tech, Paraguay) as it can be used to determine, on a case-by-case basis, the rotation time followed by the punch oscillation time during skin perforation, decreasing the transection rates of the follicular bulbs.6,7 After perforation, the grafts are extracted with two delicate forceps: one thinner and straighter to hold the epidermis and another serrated to remove the graft.8
All grafts are reviewed under the microscope, separated into UFs of 1, 2, 3, or more hairs, and total and partial transection rates are calculated. The team cleans the grafts, removing excess epidermis, as there is less formation of crusts in the postoperative period, also allowing a higher final density since it is possible to place these grafts closer to each other.
The UFs are separated in flasks according to the area extracted and the amount of hairs (1, 2, 3, or more hairs). The first grafts removed are the first to be implanted, thus reducing the time out of the body as much as possible. They are stored in a specific refrigerator (4 oC) in saline. Air humidifiers are used throughout the procedure.
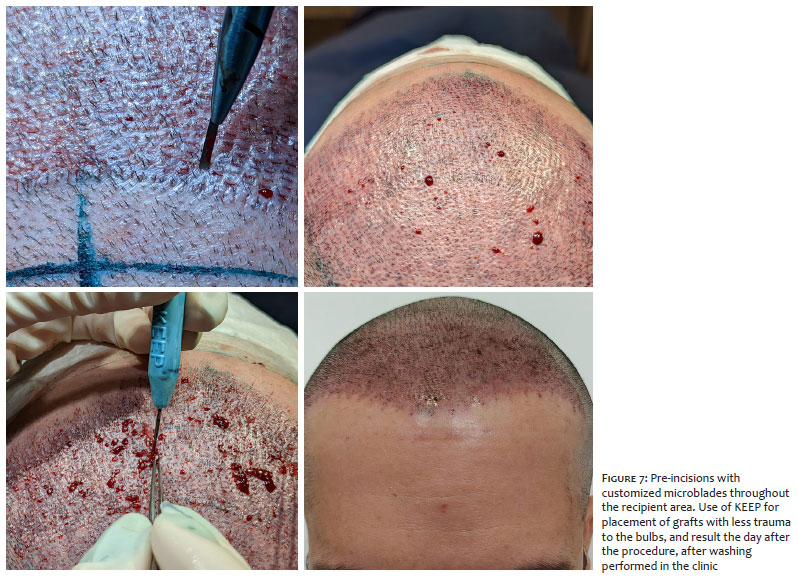
We prefer to make previous incisions in the recipient area with customized blades from 0.65 mm to 0.90 mm in width. We follow a specific order: 1) The irregular frontal line with two to three rows of one-hair UFs; 2) Transition zone with two-hair UFs); 3) Definition zone with UFs of three or more hairs; 4) Other regions of baldness or thinning.9,10 It is important to measure the length of the grafts and reduce the depth of the incision by 1 mm – it allows the epidermis to be just above the skin surface, decreasing post-operative folliculitis and uneven scarring.
We have been using KEEP implants (Figure 7) for the last five years. This tool has a special tip that protects the graft during placement, avoiding traumatizing it. With a rotating movement, the graft is fitted inside the KEEP tip; then, the graft is gently slid into the previous incision with the aid of forceps. KEEP implanters come in different sizes to place UFs with a different number of hairs.
After the procedure is finished the entire surgical area is cleaned with saline solution. We didn’t leave any bandages. The patient is referred to the resting room to receive all the instructions and postoperative medications. We assess the patient the next day for scalp washing and reorientation. We get the intermediate result in around six months and the final result in a year (Figure 8).
Despite being a superficial procedure, FUE hair transplant surgery requires the surgeon to be attentive to all stages of the procedure, considering the treatment of the receiving bald area and also the maximum preservation of the donor area for a better result for the patient.
Luciana Takata Pontes 0000-0002-9383-0569
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Antonio Ruston 0000-0003-0067-9255
Active participation in research orientation; critical literature review.
1. Jimenez F, Alam M, Vogel JE, Avram M. Hair transplantation: basic overview. J Am Acad Dermatol. 2021;85(4):803-14.
2. Shapiro R, Shapiro P. Hairline design and frontal hairline restoration. Facial Plast Surg Clin North Am. 2013;21(3):351-62.
3. Lam SM. Hair transplant and local anesthetics. Clin Plast Surg. 2013;40(4):615-25.
4. Bernstein RM, Rassman WR, Seager D, Shapiro R, Cooley JE, Norwood OT, et al. Standardizing the classification and description of follicular unit transplantation and mini-micrografting techniques. The American Society for Dermatologic Surgery, Inc. Dermatol Surg. 1998;24(9):957-63.
5. Radwanski HN, Ruston A, Lemos RG. Cirurgia da calvície: um histórico. In: Transplante Capilar: arte e técnica. São Paulo: Roca; 2011.
6. Trivellini, R. The trivellini system and technique. Hair transplant forum international september 2018;28(5):188-90.
7. Schambach, M. Why I switched to a multiphasic device. Hair transplant forum international november 2018;28(6):224-6.
8. Unger RH, Wesley CK. Technical insights from a former hair restoration surgery technician. Dermatol Surg. 2010;36(5):679-82.
9. Shapiro R. Principles and techniques used to create a natural hairline in surgical hair restoration. Facial Plast Surg Clin North Am. 2004;12(2):201-17.
10. Nakatsui T, Wong J, Groot D. Survival of densely packed follicular unit grafts using the lateral slit technique. Dermatol Surg. 2008;34(8):1016-22.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}