


Cesar Augusto Zago Ferreira; Bruno Augusto Alvares; Priscila Neri Lacerda; Helio Amante Miot
Financial support: None
Conflict of interest: None
Submitted on: 20/12/2021
Approved on: 27/01/2022
How to cite this article: Ferreira CAZ, Alvares BA, Lacerda PN, Miot HA. Dermatoscopia do cisto veloso eruptivo. Surg Cosmet Dermatol. 2022;14:e20220119
Eruptive vellus hair cyst is a rare and benign dermatological condition in the development of vellus-type hair follicles. It affects mainly children and young adults, and is characterized by multiple asymptomatic papules, especially on the trunk. We report the case of a 33-year-old white man who presented multiple erythematous papules and pustules located on the trunk for about five years, refractory to topical treatments for acne. Dermoscopy revealed oval lesions with eccentric exulceration and rare protruding filiform structures. We established the diagnosis of eruptive vellus hair cyst based on the findings of dermoscopy and histopathological examination.
Keywords: Cysts; Acneiform eruptions; HIV
A 33-year-old man, white, unemployed, was referred to Dermatology due to isolated erythematous, non-pruritic lesions on the trunk for five years.
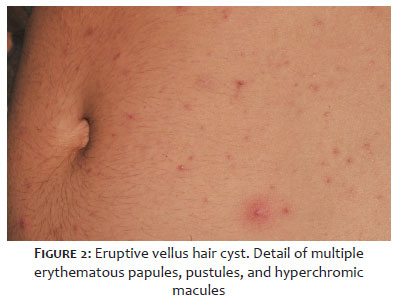
The examination showed multiple erythematous papules, between 1 mm and 2 mm in diameter, and pustules located mainly on the anterior and posterior trunk, with mild involvement of the upper and lower limbs, interspersed with areas of post-inflammatory hyperchromia (Figures 1 and 2). The patient denied a family history of similar lesions. He had HIV infection as comorbidity and was receiving antiretroviral therapy, with CD4 248 and undetectable viral load.
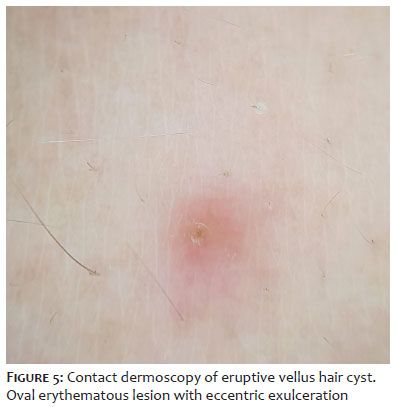
Dermoscopy revealed erythematous or hyperchromic oval macules, some showing eccentric exulceration, others revealing tiny filaments protruding from the center of the papule (Figures 3, 4, and 5).
Histopathology revealed small dermal cysts with keratinized epithelium and vellus hairs inside, surrounded by a foreign body giant cell reaction.
The patient began treatment with oral isotretinoin 20 mg/d. However, he was lost to follow-up during the covid-19 pandemic.
Eruptive vellus hair cyst (EVHC) is a rare benign condition associated with autosomal dominant inheritance, but it can also be acquired.1 It has no preference for gender or race, affecting mainly young adults.2 It was initially described in 1903, but only in 1977 Esterly considered it a clinical entity when he observed children with a clinical picture of multiple monomorphic, hyperchromic, asymptomatic papules on the trunk and limbs.1
The pathogenesis of the disease is unknown, and it is considered an abnormality of follicular development, with occlusion and dilation of the follicular unit and subsequent retention of the hair and keratinous material.3 On the other hand, some studies associate the process with hamartomatous follicular growth and mutations in the gene encoding keratin 17.3 It is also related to other conditions such as pachyonychia congenita, Lowe syndrome, and steatocystoma multiplex, which has already been described in association with EVHC.1
Multiple papules of 1-3 mm, regular or hyperchromic, with a smooth surface and increased consistency characterize the clinical picture. The lesions predominate in the thorax, upper and lower extremities, and are found rarely in the abdomen, neck, armpits, face, and groin.1,3 Generally, the cysts are closed, and whitish material may be eliminated by manual pressure.
Characteristically, they are asymptomatic but may present associated pruritus or a change in sensitivity.1
Histologically, EVHCs are located in the middle or upper dermis, with wall-lining epithelium similar to the infundibular or follicular isthmic portion, and a variable number of layers of squamous epithelium (one to 12 layers), in addition to focal and discontinuous fine granular areas. The cystic cavity contains a variable amount of keratin and vellus hair. Usually, no sebaceous gland is present in the cyst wall, and there may be a granulomatous inflammatory process.3
Electron microscopy (EM) showed the presence of scarce basal lamina around the cyst wall. In epithelial cells, large vacuoles and a marginal band were observed; and, within the cyst wall, scattered melanocytes and Langerhans cells were found.1
EVHC dermoscopy is usually monotonous, but it can provide diagnostic elements in the most characteristic cases. Usually, it reveals circular or oval, erythematous, or hyperchromic lesions, presenting an eccentric hypochromic or yellowish structure, forming a pigmentary halo. In the most exuberant cases, it’s possible to observe eccentric exulcerations and discrete, non-pigmented filiform structures protruding from the lesion, constituting groups of vellus-like hairs.4
Some studies assess EVHC using high-frequency ultrasonography and optical microscopy with 10% potassium hydroxide as an alternative to diagnosis by histopathological examination or dermoscopy.
Microscopic detection consists of making a small incision on the top of a previously anesthetized papular lesion, followed by a gentle pressure on the site, then capturing the cystic content using a sterile 18-gauge needle, with visualization of vellus hairs.6
Although optical microscopy in preparation with 10% potassium hydroxide appears to be a less painful alternative than biopsy for histopathological study, the technique may not be able to differentiate EVHC from steatocystoma multiplex since the latter may also present vellus hairs at the microscopic analysis.
On ultrasound, it is possible to observe ovoid hypoechoic nodules, located in the dermis, associated with strongly echogenic filiform areas in the middle of the cyst, corresponding to the vellus hair. Thus, dermoscopy and ultrasound are painless and non-invasive techniques to diagnose eruptive vellus hair cysts.5
The main differential diagnoses are steatocystoma multiplex, trichostasis spinulosa, folliculitis, and other cysts, such as infundibular and trichilemmal. Thus, dermoscopy and histopathological examination are crucial for diagnostic definition in many circumstances. Steatocystoma multiplex shows the expression of K10 and K17, in addition to a thin wall composed of squamous epithelium and empty cysts due to artificial loss in the fixation process, observed on histopathology. On the other hand, EVHC expresses only K171,3 and, on histopathology, vellus hairs and laminated keratin. Therefore, some authors consider steatocystoma a variant of EVHC.
In cases where non-follicular blue homogeneous pigmentation is present, blue nevus and hemangioma should be considered among the differential diagnosis. Other clinical differentials include acneiform eruption, keratosis pilaris, syringoma, milium, and molluscum contagiosum.3
The presence of light yellow homogeneous circular structures and the absence of vessels help to distinguish between molluscum contagiosum and comedonal acne.4
Most lesions persist if untreated, but spontaneous resolution may occur if vellus hairs penetrate the cyst wall, leading to the formation of a foreign body reaction. Also, inflammatory changes may occur with the appearance of whitish material, which can be eliminated spontaneously or by compressing the papule.2 As a result, spontaneous remission occurs in 25% of cases due to its transepidermal elimination or inflammatory process destruction.5
EVHC treatment is challenging. There are reports of several therapies, such as tretinoin, tazarotene, calcipotriol, topical lactic acid, oral isotretinoin, exfoliation, dermabrasion, CO2 laser, Erbium:YAG laser, needle incision, curettage, and surgical excision. However, they have limited results,1,2 leading to early recurrence, local atrophy, or hypertrophic scar formation. More exuberant cases, simulating acneiform reactions, present more exuberant dermoscopic findings, helping to define the diagnosis.
Cesar Augusto Zago Ferreira: 0000-0001-7299-1710
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Bruno Augusto Alvares: 0000-0002-0061-2969
Approval of the final version of the manuscript; critical literature review.
Priscila Neri Lacerda: 0000-0001-8100-5978
Approval of the final version of the manuscript; critical literature review.
Helio Amante Miot: 0000-0002-2596-9294
Approval of the final version of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Torchia D, Vega J, Schachner LA. Eruptive vellus hair cysts: a systematic review. Am J Clin Dermatol. 2012;13(1):19-28.
2. Coras B, Hohenleutner U, Landthaler M, Hohenleutner S. Early recurrence of eruptive vellus hair cysts after Er:YAG laser therapy: case report and review of the literature. Dermat Surg. 2005;31(12):1741-4.
3. Anand P, Sarin N, Misri R, Khurana VK. Eruptive vellus hair cyst: an uncommon and underdiagnosed entity. Int J Trichol. 2018;10(1):31-3.
4. Jerdan K, St Claire K, Bain M. Eruptive vellus hair cysts in identical triplets with dermoscopic findings. Cutis. 2018;102(5):367-9.
5. Zhu Q, Huang Y, Cui X, Du X, Zhu J. Eruptive vellus hair cysts diagnosed using dermatological imaging technique. Australas J Dermatol. 2021;62(1):86-8.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}