


Pedro Colli Rocha Dias1; Hudson Dutra Rezende1
Financial support: None
Conflict of interest: None
Submitted on: 20/06/2021
Approved on: 06/05/2022
How to cite this article: Dias PCR, Rezende HD. Microagulhamento do couro cabeludo como terapia complementar no tratamento da alopecia de padrão feminino. Surg Cosmet Dermatol. 2022;14:e20220062
Female pattern hair loss (FPHL) is one of the most frequent complaints in dermatological practice. It affects up to 50% of climacteric and postmenopausal women. Despite multiple therapies available nowadays, some patients are refractory to conventional treatments, requiring the association of second-line therapies to obtain good aesthetic results. This paper aims to show the advantages of microneedling of the scalp for such cases by reporting the case of a 48-years-old patient who failed to the association of topical minoxidil and oral finasteride therapy.
Keywords: Alopecia; Attachment disorder; Combined modality therapy; Hair diseases
It is estimated that 50% of climacteric and postmenopausal women have some degree of female pattern hair loss (FPHL).1 Although equivalent in practice, the term FPHL has been used more often than androgenetic alopecia (AGA) for women since the participation of dihydrotestosterone in the pathophysiology of follicular miniaturization has significant implications in the disease evolution in men, but it is still questionable in women.2
The Food and Drug Administration (FDA) authorizes only two treatments for FPHL: topical minoxidil and Low-Level Laser Therapy (LLLT).3 Due to the refractoriness to first-line therapies of some cases, new treatments for FPHL have been proposed, such as microneedling, drugs infusion into the scalp, and platelet-rich plasma (PRP) injection, which is currently prohibited in Brazil by the Federal Council of Medicine.4
A 48-year-old woman, menopausal, with no other morbid history, presented a clinical and dermoscopic diagnosis of FPHL. She used topical minoxidil 5%, once daily, and finasteride 5 mg orally for a year. However, she chose to discontinue the treatment due to facial hypertrichosis associated with minoxidil. After six months without the medication, the patient underwent four sessions of microneedling with an electrical device (pen) using twelve 1.5 mm needles and a 90 Hz frequency. The stipulated interval between sessions was 15 days.
The sessions were performed after local antisepsis with an alcoholic chlorhexidine solution. The frontal and vertex regions were treated, and each session lasted the period necessary to produce small bleeding spots (Auspitz sign).
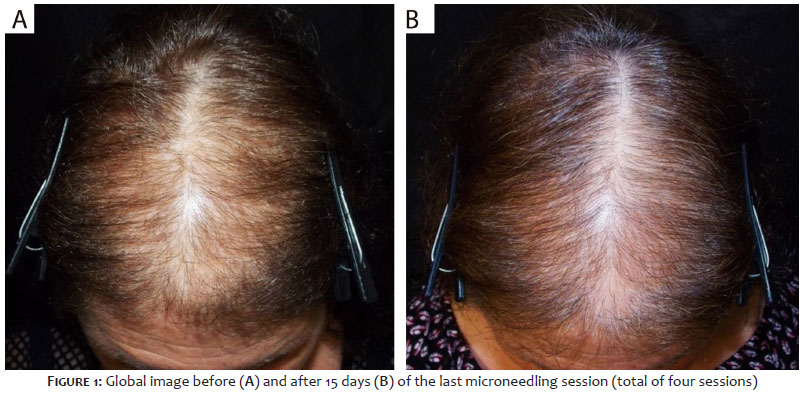
Pre-treatment and post-treatment photographic control was performed with clinical images of the scalp and dermoscopic images corresponding to the area of intersection of the coronal and sagittal lines.
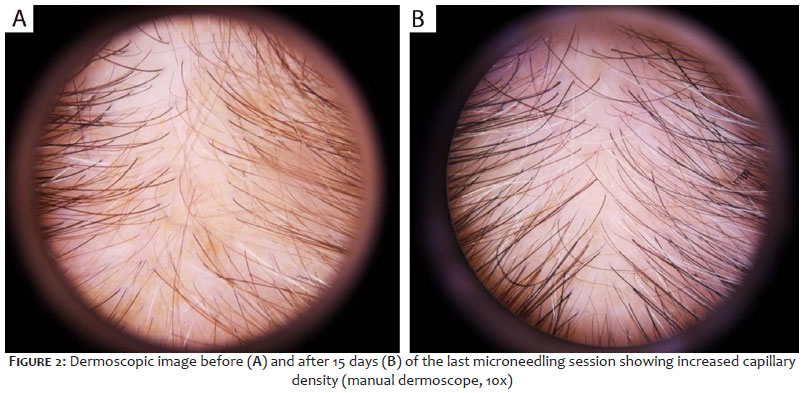
Fifteen days after the 4th session, there was increased capillary density in the frontal and vertex regions, with decreased visualization of the scalp (Figure 1). At dermoscopy, we observed increased capillary density, mainly due to the decreased difference in the hair diameter, the increased general diameter of the hair shafts, and the quantitative reduction of miniaturized hair (Figure 2).
As a chronic condition with high rates of treatment dropout, FPHL presents a challenge to clinical practice.5 The FDA officially authorizes few therapeutic options for FPHL management, such as topical minoxidil and LLLT.3
Despite its proven effectiveness, the unwanted effects of topical minoxidil therapy, such as itching, hypertrichosis, and increased scalp oiliness, lead to poor patient compliance.5 LLLT is an option that has shown satisfactory results but does not replace first-line treatments and cannot yet be considered a widely available and affordable option.6 Thus, microneedling can compose the therapeutic arsenal for cases resistant to standardized therapies or for those patients in which, for some reason, first-line therapies are not applicable.
Our case exemplifies the advantages of microneedling for refractory FPHL. The limitation of this report is the small variation in standardization between the first and second clinical photos, which can distort the global perception of capillary gain. However, dermoscopic photos support the improvement in hair removal and hair diameter after treatment.
Microneedling produces controlled dermal microperforations that stimulate angiogenesis, promote vasodilation, and subsequent release of cytokines and interleukins, also stimulating the expression of genes related to hair growth.7 Part of this action is due to the activation of cellular regeneration mechanisms arising from the follicular the bulge stem cells activation and the Wnt3a/B-catenin pathway activation, which directly signals the maintenance of the anagen phase, hair growth, and stem cell recruitment.7,8,9,10 The minor bleeding induced by the technique also releases growth factors derived from platelets, involved in the activation of the tissue repair process, and vascular endothelium growth factor (VEGF), involved in follicular growth secondary to the increase in the local angiolymphatic network, improving the dermal papilla vascularization.8,10
In the technique, the needle length, varying from 0.25 mm to 2.5 mm, defines the depth of the cutaneous microperforations.10 Although there is no rigid protocol defining the best needle length for the alopecia treatment, many authors opt to use 1.5 mm needles as they provide moderate bleeding and are well tolerated by patients.8,9,11 The number of sessions ranges widely in the literature, but few publications propose less than three sessions in the FPHL.7
The complementary character of microneedling in FPHL treatment is also reinforced by the possible formation of minimal cumulative fibrosis in the scalp in the recovery of tissue damage caused by needles.10 The long-term impact of this phenomenon on the alopecia treatment is still unclear but sufficient to not recommend microneedling as a compulsory and indistinct practice in trichology.
Few studies reveal the real contribution of microneedling alone in FPHL. The demonstration of effectiveness as a short-term monotherapy encourages the rational use of the technique as an auxiliary method in the search for better results, whether in the management of refractory cases or patients with limitations in the standardized prescription.
Pedro Colli Rocha Dias 0000-0002-6987-5177
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Hudson Dutra Rezende 0000-0002-7039-790X
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Rinaldi S, Bussa M, Mascaro A. Update on the treatment of androgenetic alopecia. Eur Rev Med Pharmacol Sci. 2016;20(1):54–8.
2. Ramos PM, Miot HA. Female pattern hair loss: a clinical and pathophysiological review. An Bras Dermatol. 2015;90(4):529–43.
3. Adil A, Godwin M. The effectiveness of treatments for androgenetic alopecia: a systematic review and meta-analysis. J Am Acad Dermatol. 2017;77(1):136-41.e5.
4. Vañó-Galván S, Camacho F. Novedades terapéuticas en tricología. Actas Dermosifiliogr. 2017;108(3):221–8.
5. Siah TW, Muir-Green L, Shapiro J. Female pattern hair loss: a retrospective study in a tertiary referral center. Int J Trichology. 2016;8(2):57–61.
6. Munck A, Dias MFRG, Trüeb RM. Use of low-level laser therapy as monotherapy or concomitant therapy for male and female androgenetic alopecia. Int J Trichology. 2014;6(2):45–9.
7. Dias MFRG, Rezende HD, Mateus A. Dermatologia das alopecias e estudo dos cabelos. São Paulo: Clannad; 2021.
8. Dhurat R, Sukesh M, Avhad G, Dandale A, Pal A, Pund P. A randomized evaluator blinded study of effect of microneedling in androgenetic alopecia: A pilot study. Int J Trichology. 2013;5(1):6–11.
9. Contin LA. Alopecia androgenética masculina tratada com microagulhamento isolado e associado a minoxidil injetável pela técnica de microinfusão de medicamentos pela pele. Surg Cosmet Dermatology. 2016;8(2):158–61.
10. Kim YS, Jeong KH, Kim JE, Woo YJ, Kim BJ, Kang H. Repeated microneedle stimulation induces enhanced hair growth in a murine model. Ann Dermatol. 2016;28(5):586–92.
11. Dhurat R, Mathapati S. Response to microneedling treatment in men with androgenetic alopecia who failed to respond to conventional therapy. Indian J Dermatol. 2015;60(3):260–3.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}