


Alexandra Brugnera Nunes de Mattos1; Gabriela Martins Fim1; Gabriela Quadri Bortoli1; Caroline Erthal1; Márcio Guedes Brandão2
Submitted on: 6/09/2021
Approved on: 22/11/2021
Financial support: None
Conflict of interest: None
How to cite this article: Mattos ABN, Fim GM, Bortoli GQ, Erthal C, Brandão MG. External vascular compression by hyaluronic acid injection via pneumatic microjet device. Surg Cosmet Dermatol. 2022;14:e20220090
Filling with hyaluronic acid using a pen that injects with vacuum pressure in the lips region became popular due to not using needles, but it presents risks like any minimally invasive procedure. We present a case of injection of hyaluronic acid with this device in the labial region, which resulted in a subocclusion of the inferior labial artery. It is known that the use of pressure can offer a lower precision than the methods already used classically. Therefore, it is important to warn about the risks of this device, which despite not using needles, presents the same risks of complications.
Keywords: Dermal fillers; Hyaluronic acid; Lip
With the popularization of hyaluronic acid fillers, there was an increase in cases of vascular complications, such as compression, vascular obstruction, and tissue necrosis, which intrigues patients and physicians.1 The hyaluronic acid pen uses pneumatic pressure to administer hyaluronic acid into the skin. Thus, it is presented as a needle-free device that, theoretically, would make the procedure safer. However, like any minimally invasive aesthetic technique, it presents vascular risks. This study aims to report a case of vascular compression by a vacuum device and discuss the risk of this method.
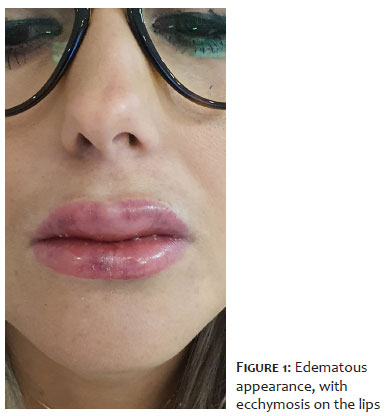
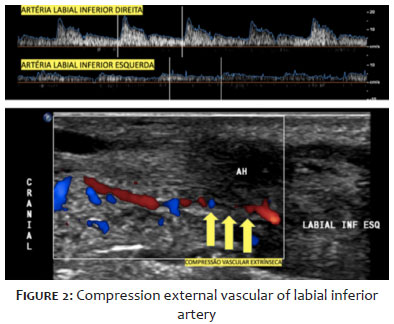
A 31-year-old woman sought dermatological care reporting significant lip edema three hours after undergoing lip filling with two syringes of hyaluronic acid using a needle-free pneumatic injection device. Before the procedure, the patient had already ingested 80 mg of prednisone and 180 mg of fexofenadine on her own, as she had already presented an episode of lip edema four months ago, after the application of 1 ml of hyaluronic acid with a needle. At the time, she underwent an allergic test to lidocaine and mepivacaine anesthetics, both negative. On physical examination, she presented significant diffuse edema, with a hardened appearance of the lips and ecchymosis, but no pallor (Figure 1). We referred the patient for urgent ultrasound examination, which showed changes in flow amplitude and vascular resistance between the right and left inferior labial arteries, with reduced systolic velocity peaks and decreased vascular resistance distally, suggesting extrinsic compression of the artery horizontal labrum, but without signs of occlusion (Figure 2). Also, multiple hypoechoic areas were observed in between, affecting the upper and lower lips throughout their extension, compatible with an important focal inflammatory process after using the filler. The patient was followed up and prescribed prednisone 40 mg and ciprofloxacin 500 mg daily. It was it was not necessary to apply hyaluronidase. Within 24 hours, there was a reduction in edema, with no signs of arterial occlusion.
The hyaluronic acid injection via a pneumatic microjet device is a system for administering substances into the skin through pneumatic pressure exerted by the equipment. As it is a needle-free device, it is believed to be safe.2 However, as with any minimally invasive procedure, there are risks of complications, such as edema, ecchymosis, site infection, and arterial occlusion. Using a needle-free pneumatic injection pen, the application plan can be erratic, and the hyaluronic acid can penetrate the most diverse layers of the skin and lead to vascular compression, as in the case presented here. Furthermore, there are anatomical variations in the labial artery, which is a challenge for physicians 3 because both labial arteries are branches of the facial artery (FA). In the upper lip, the main one is the superior labial artery (SLA), and the septal (SA) and subalar (SAA) arteries are usually optional. It is important to emphasize that the superior labial artery is bilateral; nevertheless, it can present significant variations.4 The lower lip, in its turn, is supplied by the inferior labial artery (ILA) and labiomental artery (LMA) – the last one has both horizontal and vertical branches.
Complications are classified as early (related to infiltration, such as edema, pain, ecchymosis, bleeding, inflammatory, and allergic reactions) or late (regarding infections, nodules, granuloma, and scars).5 Vascular complications can arise due to the anatomical location, the injected volume, the use of narrow gauge needles, previous scars, and the material composition.6 The applied technique, the high volume of hyaluronic acid, and the previous reaction to hyaluronic acid may have exacerbated the reaction of the patient in this study. Based on current scientific evidence, if any complications occur in the procedure, it is recommended to stop it immediately, massage the area, use high doses of hyaluronidase as a way to undo it, and wait around an hour to reassess the need for a new infiltration.5 In the case the patient evolves with greater edema and arterial occlusion, there would be a need for local injection of hyaluronidase to dissolve the product. Therefore, a good anamnesis, anatomical knowledge, in addition to a professional trained to recognize complications and treat them, are essential to avoid a worse evolution of the case.
The application of hyaluronic acid using a pneumatic microjet device has risks. As the application is made via pressure, the product can penetrate the tissues erratically and lead to vascular occlusion and other complications. Thus, the search for a trained professional with well-studied filling techniques should always be recommended.
Alexandra Brugnera Nunes de Mattos 0000-0002-7284-7193
Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Gabriela Martins Fim 0000-0003-2919-1253
Preparation and writing of the manuscript; critical revision of the manuscript.
Gabriela Quadri Bortoli 0000-0002-1691-518X
Preparation and writing of the manuscript.
Caroline Erthal 0000-0002-3189-855X
Critical revision of the manuscript.
Márcio Guedes Brandão 0000-0002-3114-693X
Intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
1. DeLorenzi C. Complications of injectable fillers, part 2: vascular complications. Aesthet Surg J. 2014;34(4):584-600.
2. Lima VGF, Regattieri NAT, Pompeu MF, Costa IMC. External vascular compression by hyaluronic acid filler documented with high-frequency ultrasound. J Cosmet Dermatol. 2019;18(6):1629-31.
3. Vent J, Lefarth F, Massing T, Angerstein W. Do you know where your fillers go? An ultrastructural investigation of the lips. Clin Cosmet Investig Dermatol. 2014;7:191-9.
4. Paixão MP. Conheço a anatomia labial? Implicações para o bom preenchimento. Surg Cosmet Dermatol. 2015;7(1):10-6.
5. Daher JC, Da-Silva SV, Campos AC, Dias RCS, Damasio AA, Costa RSC. Vascular complications from facial fillers with hyaluronic acid: preparation of a prevention and treatment protocol. Rev Bras Cir Plást. 2020;35(1):2-7.
6. Manual Smart Press. SMART PRESS XS, 2021. Accessed: 27 fev 2021. Available from: https://cdn.awsli.com.br/297/297389/arquivos/Manual%20-%20Smart%20Press%20XS%20(H)%20V1.pdf.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}