


Anelise Darabas dos Santos1; Douglas Haddad Filho2; Flávia Fenólio Nigro Marcelino3; Luiza Vieites4
Submitted on: 24/07/2021
Approved on: 13/09/2021
Financial support: None
Conflict of interest: None
How to cite this article: Santos AD, Haddad Filho D, Marcelino FFN, Vieites L. Applicability of the Limberg Flap: a case series. Surg Cosmet Dermatol. 2022;14:e20220079
Local flaps are an excellent option for repairing the excision of skin tumors, where the primary closure of the defect would cause aesthetic and functional impairment. The rhomboid (Limberg) flap is a simple and versatile transposition flap that can be applied widely with good cosmetic and vascularization results. The retrospective analysis of a case series using the Limberg flap to reconstruct defects resulting from tumor resections proved to be easy to perform, with excellent evolution and vascular viability.
Keywords: Carcinoma basal cell; Skin neoplasms; Surgical flaps; Surgical oncology
Skin cancer is the most incident worldwide, with basal cell carcinoma (BCC) being the most common malignant neoplasm. Its incidence has increased over the last few years, influenced by population aging and accumulated sun exposure. BCC has low mortality but can cause significant morbidity, mainly due to local tissue destruction.1
The clinical and histological presentation of BCC is quite variable and includes the nodular, superficial, infundibulocystic, fibroepithelial, and desmoplastic subtypes, with different characteristics.1,11 Due to its low metastatic power, BCC treatment aims mainly at local control. Anatomical location is a known risk factor for BCC recurrence, and areas in the H-zone of the face, which encompasses the nose, temples, ears, periocular, periauricular, and upper lips, are considered high-risk regions, regardless of tumor size. Surgical resection with adequate safety margins of the lesion is the mainstay of treatment for this neoplasm. However, it causes aesthetic and/or functional damage, requiring the use of local reconstruction techniques to close the resulting cutaneous defects.1 A thorough evaluation of each lesion and each patient chooses surgical method to have a better result regarding surgical recovery and the aesthetic outcome.
Skin flaps are classified according to the movement of the skin towards the receptor area. They can be advancement, rotation, transposition, or interpolation flaps.3,4 The Limberg flap is a straightforward and versatile type of transposition flap since its geometric design can be constructed from any of the four corners of the rhomboid design.5,6
It is called “transpositional” because it is elevated and mobilized towards an adjacent defect and transposed by an incomplete bridge of skin.3 Alexander A. Limberg first described its use in 1946, based on the Euclidean definition of the geometric figure of the rhomboid design, a parallelogram with four equal sides, equal opposite acute angles, and equal opposite obtuse angles.4,7 The traditional rhombic flap using the Limberg design is performed with 60 and 120 degrees angles of equal length sides.3
Subsequently, Dufourmentel and Webster performed modifications to the original technique.3 Dufourmentel proposed its alteration using a 90 degree angle, allowing a smaller rotation arc and less tension at the flap tip.4,6,8 Webster projected the construction of a 30 degrees angle, increasing the pedicle base, combined with M-plasty, decreasing the rotational deformity of the edges and reducing tension at the donor site.4,9
We conducted a retrospective analysis of a series of cases involving 20 outpatient surgeries, in which local anesthesia with 1% lidocaine and epinephrine solution 1:200,000 was used. The flaps were made considering the size and location of the original defect, as well as lines of force, and elasticity of the adjacent tissues. They were performed with 0.5 cm safety margins on the sides and across the entire thickness of the skin.
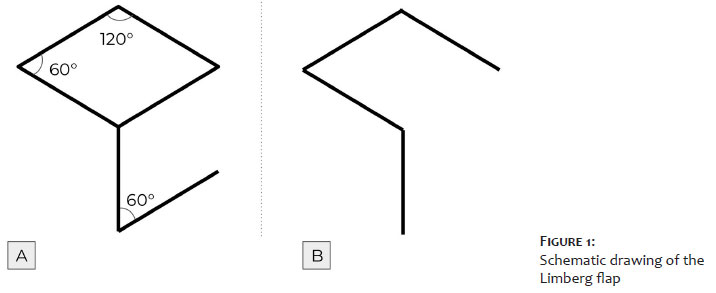
From the defect resulting from the resection, a diamond was drawn with internal 60 degrees and 120 degrees angles (Figure 1A). The marking must be idealized with two equilateral triangles with 60 degree angles aligned base to base, so that all sides of the defect have the same length, which, in practice, is equal to the smallest diagonal. The first side of the flap is an extension out of the defect of the smallest diagonal along its own length; the second side is marked with a line the same size as the first one, adjacent to the diamond defect, creating a 60 degree angle at the apex of the flap.
The final configuration of the flap scar, in all cases, is predictable, as Figure 1B shows.10 In dermatological surgery, the rhomboidal flap is very useful in the forehead, periocular regions, nasal tip, malar region, chin, and neck, and can be applied to other regions of the body.4
For each defect, four rhomboid flaps can potentially be made. Then, according to the lines of tension and expression of the skin, orientation, and location, the flap that best adapts to the defect is chosen. The undermining of all lesion edges, the flap edges, and the flap base is performed, providing an adequate approximation of the tissues, without tension in the closure.10
We assessed a series of patients diagnosed with BCC in which the Limberg flap was used for post-excision reconstruction of the lesions. All patients were Fitzpatrick skin phototype II. We highlight that, from the selected series, in four cases the flap was performed on the face and, in another patient, on the left thoracic region (Figure 6), which demonstrates the versatility of using this flap. All cases progressed well, with excellent tissue perfusion. Figures 2, 3, 4, and 5 illustrate other cases in the present series.
Local flaps are an excellent option for the excision repair of tumor skin lesions, where primary closure of the defect would cause aesthetic and/or functional damage, with the possibility of distortion of the structures. They are preferred to grafts as they present better color and texture correspondence with the recipient skin area since they are in the same region. Also, they don’t need a homogeneous receptor bed for good integration since they have their vascular pedicle.2 A well-planned and executed local flap allows the acquisition of excellent results and minimal distortion of facial lines.3
The safety of the rhomboid flap has made its use increasingly widespread, and it can be applied on a large part of the body surface.12,13 Local facial flaps, especially on the forehead, malar region, temple, and lower part of the chin and lip, are ideal locations for vector transposition using the rhomboid flap according to Langer’s lines.4 The literature also reports the use of the Limberg flap to reconstruct defects after resection of large lesions in the trunk,13 as in the present series, and also in the pilonidal cyst,14 lumbosacral meningomyelocele correction,15,16 burns sequelae, such as bands and synechiae, antecubital region,17 and even in breast reconstructions.18,19 The choice of using this flap in patients with trunk injuries considers the limitation of edge-to-edge closure, extensive scarring, excess tension, and increased possibility of complications.
The Limberg flap is versatile, and up to four flaps can be elevated from the rhomboid design if necessary, which cannot be seen in advancement or bilobed flap, for example. It can be applied in single or multiple formats, with vascular viability and good cosmetic results.5
We can conclude that the Limberg flap presented good aesthetic and functional results in the cases described, illustrating its great versatility both in facial lesions and in extensive injuries in the trunk, proving to be a safe flap with good vascularization and easy to perform.
Anelise Darabas dos Santos 0000-0002-4957-9688
Preparation and writing of the manuscript; critical literature review.
Douglas Haddad Filho 0000-0001-9304-4739
Approval of the final version of the manuscript; study design and planning; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Flávia Fenólio Nigro Marcelino 0000-0003-4057-5143
Preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review.
Luiza Vieites 0000-0003-0647-8104
Preparation and writing of the manuscript.
1. Kim DP, Kus KJB, Ruiz E. Basal cell carcinoma review. Hematol Oncol Clin North Am. 2019;33(1):13-24.
2. Schmid MH, Meuli-Simmen C, Hafner J. Repair of cutaneous defects after skin cancer surgery. Recent Results Cancer Res. 2002;160:225-33.
3. Starkman SJ, Williams CT, Sherris DA. Flap basics I: rotation and transposition flaps. Facial Plast Surg Clin North Am. 2017;25(3):313-21.
4. Hon HH, Chandra SR. Rhomboid flap. Atlas Oral Maxillofac Surg Clin North Am. 2020;28(1):17-22.
5. Chasmar LR. The versatile rhomboid (Limberg) flap. Can J Plast Surg. 2007;15(2):67-71.
6. Lister GD, Gibson T. Closure of rhomboid skin defects: the flaps of Limberg and Dufourmentel. Br J Plast Surg. 1972;25(3):300-14.
7. Limberg AA. Mathematical principles of local plastic procedures the surface of the body. Leningrad (Russia): Medgis; 1946
8. Dufourmentel C. Le lambeau en L pour losange (LLL). Interview de Claude Dufourmentel par E. Achard [The L-shaped flap for lozenge-shaped defects. Interview with Claude Dufourmentel by E. Achard]. Ann Chir Plast. 1979;24(4):397-9.
9. Webster RC, Davidson TM, Smith RC. The thirty degree transposition flap. Laryngoscope. 1978;88(1 Pt 1):85-94.
10. Alvarez GS, Laitano FF, Siqueira EJ, Oliveira MP, Martins PDE. Aplicações do retalho romboide em reparações cutâneas. Rev Bras Cir Plást. 2012;27(1):102-7.
11. Cameron MC, Lee E, Hibler BP, Barker CA, Mori S, Cordova M, et al. Basal cell carcinoma: epidemiology; pathophysiology; clinical and histological subtypes; and disease associations. J Am Acad Dermatol. 2019;80(2):303-17.
12. Aydin OE, Tan O, Algan S, Kuduban SD, Cinal H, Barin EZ. Versatile use of rhomboid flaps for closure of skin defects. Eurasian J Med. 2011;43(1):1-8.
13. Kang AS, Kang KS. Rhomboid flap for large cutaneous trunk defect. Plast Reconstr Surg Glob Open. 2020;8(6):e2932.
14. Akin M, Leventoglu S, Mentes BB, Bostanci H, Gokbayir H, Kilic K, et al. Comparison of the classic Limberg flap and modified Limberg flap in the treatment of pilonidal sinus disease: a retrospective analysis of 416 patients. Surg Today. 2010;40(8):757-62.
15. Ohtsuka H, Shioya N, Yada K. Modified Limberg flap for lumbosacral meningomyelocele defects. Ann Plast Surg. 1979;3(2):114-7.
16. Muneuchi G, Matsumoto Y, Tamai M, Kogure T, Igawa HH, Nagao S. Rhomboid perforator flap for a large skin defect due to lumbosacral meningocele: a simple and reliable modification. Ann Plast Surg. 2005;54(6):670-2.
17. Gümüş N. A new approach to the antecubital scar contracture: rhomboid rotation flap. J Plast Reconstr Aesthet Surg. 2010;63(8):1392-3.
18. Gwynn BR, Williams CR. Use of the Limberg flap to close breast wounds after partial mastectomy. Ann R Coll Surg Engl. 1985;67(4):245-6.
19. Silva Neto MP, Adão O, Scandiuzzi D, Chaem LHT. Retalho rombóide na reparação mamária imediata pós-quadrantectomia e dissecção axilar. Rev Bras Cir Plást. 2001;16(1):29-34.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}