


Bruna Margatho Elias; Giovanna Curi Campos; Hudson Dutra Rezende; José Roberto Paes Almeida; Karla Calaça Kabbach Prigenzi; Sandra Lopes Mattos Dinato
Submitted on: 27/07/2021
Approved on: 18/08/2021
Financial support: None
Conflict of interest: None
How to cite this article: Elias BM, Campos GC, Rezende HD, Almeida JRP, Prigenzi KCK, Dinato SLM. Merkel cell carcinoma: multiple primary skin lesions in the lower limb. Surg Cosmet Dermatol. 2022;14:e20210082
Merkel cell carcinoma is a rare and aggressive neuroendocrine skin tumor usually presenting as a single lesion in the head or neck region. We report a case of atypical topography and presentation, with multiple and simultaneous tumors on the left leg of rapid progression associated with palpable inguinal lymphadenopathy and diagnostic confirmation by histopathology and immunohistochemistry. Exeresis of the left inguinal lymph node and skin lesions with a safety margin was performed.
Keywords: Carcinoma Merkel cell; Merkel cells; Merkel cell polyomavirus
Merkel cell carcinoma (MCC) is a rare form of non-melanoma skin cancer of neuroendocrine origin, more common in elderly white men.1 In general, it manifests as an asymptomatic papule or nodule, pink or bluish-red, with a rapid increase in size, in weeks to months.2 The most affected sites are the photoexposed areas of the head and neck.3 The pathogenesis of MCC is still unknown, despite the association with several chromosomal abnormalities, growth signaling, and apoptotic pathways, in addition to the possible involvement of polyomavirus in tumor carcinogenesis. Even today, MCC represents a diagnostic and therapeutic challenge in clinical practice.
A Caucasian 70-year-old man, born and residing in Santos, retired, came to the Dermatology Sector complaining of multiple fast-growing lesions on the left leg, four months ago. The lesions were painful, with colorless exudation. The patient reported swelling, color change in the region, and difficulty walking. He denied any systemic symptoms, despite using atenolol and sinvastatin. Dermatological examination revealed multiple papules, nodules, tumors (diameters ranged from 1 cm to 6 cm) with exudate. The lesions had a slightly soft consistency on palpation (Figure 1). Painless, nonadherent bilateral inguinal lymph nodes were palpable, and edema was present in the compromised limb. Dermoscopy showed multiple irregular, polymorphic vessels, bright white areas without structures, and milky-red areas. Also, we observed a lesion clinically compatible with basal cell carcinoma (BCC) in the presternal region.
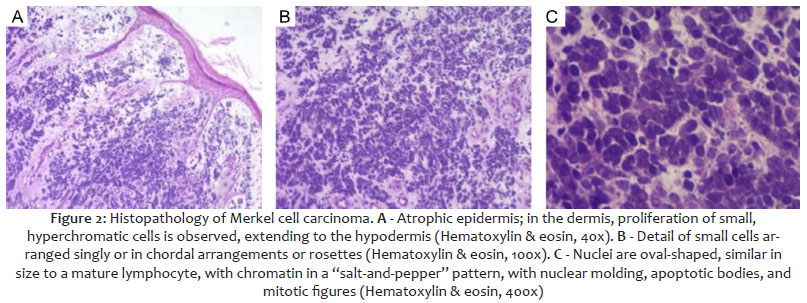
Biopsy of a solitary papular lesion near the left medial malleolus revealed proliferation of atypical small cells in the dermis, with a high nucleus/cytoplasm ratio, a high mitotic index (>30 mitoses/10CGA), and numerous apoptotic bodies, arranged in chordal pattern or solid blocks, which sometimes outlined rosettes. It indicated a high-grade malignant neoplasm, suggesting a small cell neuroendocrine carcinoma (Figure 2). Immunohistochemistry revealed immunoexpression of cytokeratin 5/6, chromogranin, synaptophysin, and CK20 in a “dotted” pattern, confirming epithelial histogenesis and neuroendocrine differentiation of neoplastic cells, compatible with the diagnosis of MCC (small cell neuroendocrine carcinoma). Markers indicative of squamous differentiation, melanocytic histogenesis, and pulmonary and gastrointestinal primary site were also performed and were negative.
Given the rarity of the case and its atypical topography and presentation, we searched immunosuppression, which was negative. Thus, the differential diagnosis with neuroendocrine carcinoma of another primary site was questioned. Additional evaluation with computed tomography (CT) scans of the chest, abdomen, and pelvis did not reveal disease in other sites nor lymph node enlargement. CT of the left leg showed exophytic skin lesions that maintained continuity with the subcutaneous tissue, without presenting a clear cleavage plane with the underlying muscle fasciae and without infiltrating deeper muscles or planes. Plasma investigation by qualitative PCR for polyomavirus was negative.
The patient was referred to oncological surgery and underwent excision of the left inguinal lymph node, which was sent for intraoperative and subsequent histopathological frozen section, with a negative result. Then, excision of the skin lesions was performed with a safety margin (Figure 3).
Due to the extensive exposed area, with the impossibility of primary closure and difficulty to conduct flaps due to the skin condition, a dressing was made with silver sulfadiazine and Rayon bandage, opting for healing by secondary intention (Figure 4).
MCC is a rare and aggressive condition that affects white men in the 7th and 8th decades of life, coinciding with the profile of the presented patient.1 Classically, it involves photoexposed skin of the cervicofacial region in 29-53% of cases, according to current literature. Approximately 1/3 of cases (35-38%) affect the extremities, 21% upper limbs, and only 14-24% lower limbs.4
The case reported here was observed in a region of rare involvement. Regarding the clinical presentation, it varies widely; however, it’s typically characterized by a single, persistent, and asymptomatic erythematous-violaceous nodular lesion, often smaller than 2 cm, with rapid growth, reaching 20 cm in months.1,5,6 In almost 1/3 of the cases, there are other simultaneous skin neoplasms, such as basal cell carcinoma (BCC), which agrees with our patient.3 The pathogenesis is uncertain, but the polyomavirus seems to have some role, as it is detected in most cases (80%) and frequently among patients with acquired immunodeficiency syndrome and transplanted immunosuppressed individuals. Also, it is integrated into the genome before the clonal expansion of tumor cells, suggesting that it is a factor that contributes to the development of the tumor.4,5 The patient in question did not have immunosuppression or positive serology for the virus.
Due to the usually nonspecific clinical picture, imaging investigation is necessary, helping to diagnose and differentiate MCC from metastases from other neuroendocrine carcinomas, such as small cell lung cancer. The diagnosis is based on a thorough examination of the skin and lymph nodes, biopsy, and histological evaluation by an experienced dermatopathologist.6 Histologically, it presents as small, uniform basophilic cells that fill the dermis with scant cytoplasm, “dusty” chromatin, and nuclear molding. The cells are organized in nests, spreading to the reticular and subcutaneous dermis, with eventual epidermal involvement. The MMC has neuroendocrine and epithelial characteristics, expressing some markers, and CK204 is a very specific and sensitive marker when found in the paranuclear “dotted” pattern, which can be confirmed in the case presented.
It is a highly aggressive and metastatic tumor, with a disease-specific 5-year survival rate of 64% and a 3-year mortality rate of 33% after diagnosis.1,4 It is known that 2/3 of patients with MCC present only local disease but nodal or metastatic condition at the time of diagnosis is not uncommon and local recurrence is around 25-33%.5 A sentinel lymph node biopsy, performed in this case, should be considered for all patients, as 1/3 of individuals with clinically localized disease at the time of presentation has occult lymph node involvement,6 and hematogenous and/or distant lymphatic metastases may occur involving mainly the liver, bones, brain, and skin.1
As for MCC treatment, there is no consensus. Surgical excision is the standard therapy for primary lesions smaller than 3 cm and adjuvant radiation therapy for lesions larger than 2 cm. Some studies recommend 2 cm margins for tumors larger than 2 cm and 1cm margins for tumors smaller than 2 cm. However, there are no controlled studies comparing different excision margins, considering the rarity of the disease.1,4 Also, there is evidence for the use of radiotherapy exclusively for unresectable disease, but not for chemotherapy, reserved for cases of metastatic disease.1,4
Although rare, the incidence of MCC is increasing due to the aging of the population, increased sun exposure, and the high number of immunocompromised individuals.7 As it is an aggressive tumor, atypical presentations must be considered since early recognition makes it possible to improve quality of life and prognostic perspectives.4, 7, 8
Bruna Margatho Elias 0000-0003-2615-5775
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Giovanna Curi Campos 0000-0002-8155-4499
Preparation and writing of the manuscript; critical literature review.
Hudson Dutra Rezende 0000-0002-7039-790X
Approval of the final version of the manuscript; preparation and writing of the manuscript; ; active participation in research orientation; critical literature review; critical revision of the manuscript.
José Roberto Paes Almeida 0000-0002-3869-6715
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Karla Calaça Kabbach Prigenzi 0000-0002-8264-8972
Preparation and writing of the manuscript; critical literature review.
Sandra Lopes Mattos Dinato 0000-0002-4547-0474
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Bassi A, Arunachalam M, Galeone M, Scarfì F, Maio V, Moretti S, et al. Multiple clustered nodules on the leg. Diagnosis: Merkel cell carcinoma. J Clin Oncol. 2014;32(17):e61-2.
2. Almeida MW, Lopes CC, Almeida Junior HL, Costa LE. Carcinoma de células de Merkel em extremidade inferior [Merkel cell carcinoma in lower end]. Rev Col Bras Cir. 2012;39(2):165-7.
3. Fernández-Regueiro R, Suárez-Sánchez FJ, Morís-de la-Tassa J. Merkel cell carcinoma. Report of a case with an atypical location and presentation. Rev Esp Cir Ortop Traumatol (Engl Ed). 2019;63(4):313-5.
4. Blumenthal L, VandenBoom T, Melian E, Peterson A, Hutchens KA. Multiple primary Merkel cell carcinomas presenting as pruritic, painful lower leg tumors. Case Rep Dermatol. 2015;7(3):316-21.
5. Chatzinasiou F, Papadavid E, Korkolopoulou P, Levidou G, Panayiotides I, Theodoropoulos K, et al. An unusual case of diffuse Merkel cell carcinoma successfully treated with low dose radiotherapy. Dermatol Ther. 2015;28(5):282-6.
6. Coggshall K, Tello TL, North JP, Yu SS. Merkel cell carcinoma: an update and review: pathogenesis, diagnosis, and staging. J Am Acad Dermatol. 2018;78(3):433-42.
7. Duprat JP, Landman G, Salvajoli JV, Brechtbühl ER. A review of the epidemiology and treatment of Merkel cell carcinoma. Clinics. 2011;66(10):1817-23.
8. Strobel ES, Feyer P, Steingräber M, Schmitt-Gräff A, Kohl PK. An unusual case of Merkel cell carcinoma. J Cancer Res Clin Oncol. 2008;134(2):119-23.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}