


Isabella Zurita Dehó1; Jayme de Oliveira Filho2; Irina Andrea Pires Afonso2; Anna Rita Ferrante Mitidieri de Oliveira1
Submitted on: 27/05/2021
Approved on: 04/06/2021
Financial support: None
Conflict of interest: None
How to cite this article: Dehó IZ, Oliveira Filho J, Afonso IAP, Oliveira ARFM. Unexpected riziform bodies. Surg Cosmet Dermatol. 2022;14:e20220057
Riziform bodies are structures in the synovial fluid or attached to the synovium, which macroscopically resemble rice grains. They are common in patients with rheumatoid arthritis and result from a chronic inflammation. They are found in 25% of aspiration procedures or joint surgery. However, there are still no publications reporting its presence in the subcutaneous tissue. We report for the first time the occurrence of riziform bodies in the subcutaneous plane of the palmar region in a patient with rheumatoid arthritis, confirmed by sonographic and anatomopathological examination, successfully treated with surgical drainage, without recurrences after two years of follow-up.
Keywords: Abscess; Rheumatoid arthritis; Dermatopathies; Hand dermatoses; Outpatient Surgical Procedures; Surgical Diagnostic Techniques
Riziform bodies are structures found in the synovial fluid or adhered to the synovia. They receive this name because they macroscopically resemble rice grains.1 These agents occur due to a chronic and nonspecific synovial inflammatory response.2 They are composed of an acidophilic center of collagen types I, II, and IV, encapsulated in the periphery by fibrin.3, 4
These structures were described for the first time in 1895 in a patient with tuberculous arthritis.1 They were later described in association with other diseases, such as rheumatoid arthritis (RA), juvenile idiopathic arthritis (JIA), osteoarthritis, tenosynovitis associated with brucellosis, joint infection by mycobacteria and fungi, or even idiopathically, in patients without comorbidities.1, 3
They are currently more frequently associated with rheumatoid arthritis than seronegative arthritis. Its removal ensures clinical improvement for patients, reduction of synovitis, and the possibility of investigating infectious causes.5
Riziform bodies are found in 25% of aspiration procedures or joint surgeries.3,4 However, there are still no publications reporting their presence in the subcutaneous plane, even in patients with rheumatoid arthritis. In this article, we report, for the first time, the occurrence of riziform bodies in the subcutaneous tissue of the palmar region in a patient with rheumatoid arthritis, confirmed by ultrasound and pathological examinations. They were successfully surgically drained, with no recurrences after a two-year follow-up.
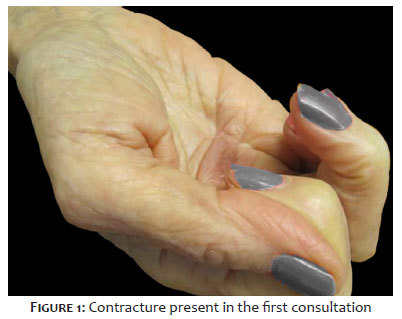
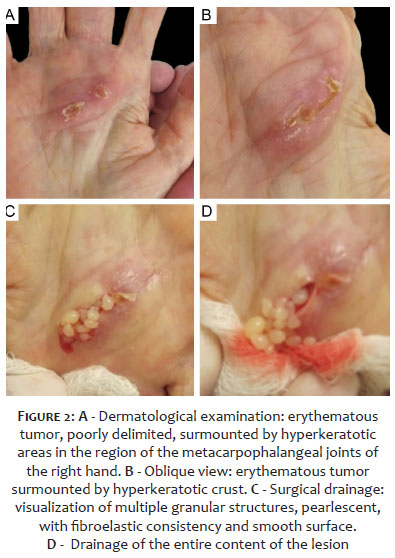
A 67-year-old woman, skin phototype II, born and resident in São Paulo, sought medical care for three weeks complaining of pain and difficulty opening her right hand (Figure 1). Dermatological examination revealed an erythematous tumor, poorly delimited, measuring 2.7 cm in its longest axis, surmounted by hyperkeratotic areas in the right palmar region, at the level of the metacarpophalangeal joints, between the second and fourth fingers (Figures 2A and 2B).
She had a personal history of hepatitis C, diabetes mellitus, sickle cell anemia, rheumatoid arthritis, and kidney transplantation 26 years ago. The patient was in use of ribavirin, NPH human insulin, azathioprine, folic acid, B complex, alpha epoetin, and prednisone 5 mg/d.
The differential diagnoses included cutaneous abscess, tenosynovitis, epidermal inclusion cyst, adnexal tumor, and Dupuytren’s contracture.
Given that the clinical characteristics suggested the diagnosis of abscess, we chose treatment with oral ciprofloxacin 500 mg 12/12h for ten days and requested exams, including imaging. After a week, the patient returned with the results of the exams, and the lesion still looked the same.
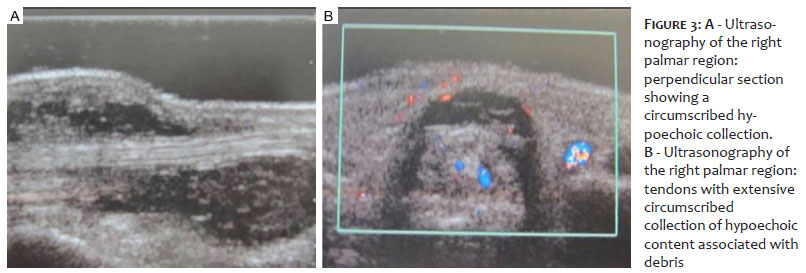
The ultrasound of the right hand showed tendons with an extensive circumscribed collection, walls, and hypoechoic content associated with thick suspension debris surrounding the tendons (Figure 3).
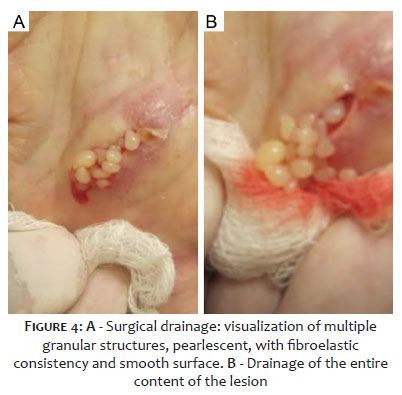
We conducted the surgical drainage of the lesion. During the procedure, we observed the presence of a fibrous nodule adhered to the deep planes, associated with the emergence of multiple granular, cystic structures, with fibroelastic consistency and smooth surface (Figures 4A and 4B).
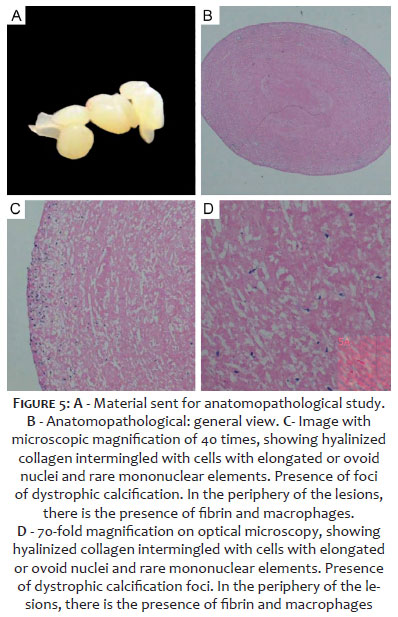
The material was sent to the anatomopathological exam (Figures 5A, 5B, 5C, and 5D), which showed granular material represented by hyalinized collagen, intermingled with cells with elongated or ovoid nuclei and rare mononuclear elements, and presence of foci of dystrophic calcification. In the periphery of the lesions, we observed the presence of fibrin and macrophages, some of them phagocytizing a light brown pigment with the characteristics of hemosiderin. There was an absence of signs of malignancy. These features confirmed the diagnosis of “riziform bodies”.
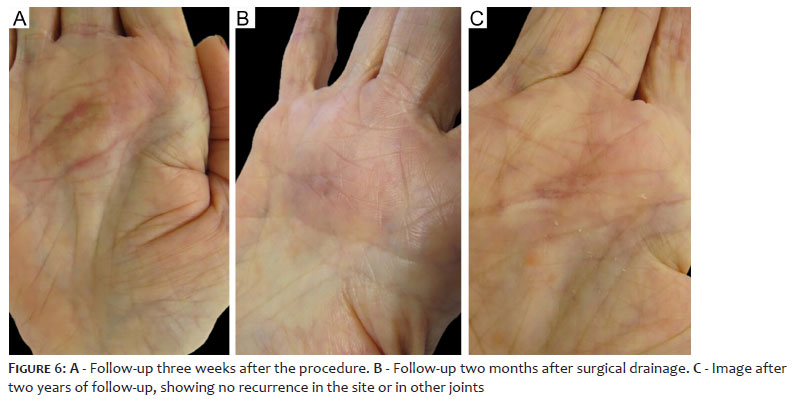
One month after the drainage, the patient returned for consultation, presenting clinical improvement; however, she still had difficulty flexing her fingers (Figure 6A).
Two months after the drainage, the patient returned with significant clinical improvement, including the ability to flex her fingers, which was previously difficult to perform (Figure 6B).
The patient evolved with complete wound healing and no recurrence after a two-year follow-up (Figure 6C).
This article presents the complete clinical picture and the follow-up of the lesions within one month, two months, and two years after the procedure.
Riziform bodies are prevalent in patients with rheumatoid arthritis. Previous studies have already demonstrated its presence in 72% of the joint effusions of these patients.5 On average, they appear in rheumatoid arthritis with six to nine years of evolution. Still, they can occur both at the onset of the condition and in later stages, without association with the disease severity.5
Its pathogenesis remains uncertain. It is believed that these bodies are the end product of an inflammatory and proliferative process in the synovia, associated with ischemia with subsequent degeneration and desquamation of the same, encapsulated by fibrin.6
In this article, the patient had a previous diagnosis of rheumatoid arthritis. On the other hand, other authors reported the presence of riziform bodies before the diagnosis of inflammatory arthritis, highlighting the importance of following up on these patients for at least one to two years for etiological investigation.2
Riziform bodies have already been isolated in chronic infectious arthritis of the hands, mainly caused by Mycobacterium marinum and M. avium.7 However, it is the first article to report their occurrence in this location, associated with rheumatoid arthritis.
Furthermore, during surgical drainage, we observed that they originated from the subcutaneous tissue of the patient’s palmar region, unlike what is expected in rheumatoid arthritis, in which they predominantly occur within the bursa, with the subacromial being the most affected. This subcutaneous occurrence was previously reported only in tenosynovitis caused by mycobacteria.8
In patients with rheumatoid arthritis, consideration of concomitant infection is essential, especially in patients using immunosuppressants and corticosteroids.7
As shown the particles are characterized, macroscopically, by a smooth, light, yellow surface. However, it has already been demonstrated that riziform bodies can present several morphological variations: color (between white and yellow), consistency (smooth or rough), and size (from less than 2 mm to greater than 7mm).5
In this case, the patient had complete remission of the lesion after surgical drainage without the need for additional treatments. Other authors have reported similar results after treatment but with a shorter follow-up time than described in this article.2 The improvement with drainage seems to be due to the removal of fibrin deposits that make up the riziform bodies since this substance presents the ability to perpetuate the inflammatory stimulus in the joints.5 Thus, in addition to being curative, surgical drainage reduces the recurrence risk, as observed during the two-year follow-up of our patient.9
Another measure associated with surgical treatment is the clinical control of underlying arthritis with specific pharmacological therapy, and, in cases of associated infection, antimicrobial therapy should be introduced.
What most caught our attention in this patient was the rarity we came across similar cases.
The diagnosis was made through physical examination combined with ultrasound examination and confirmed by pathological examination. Along with the unique characteristics of the surgical finding, we concluded this unusual and rare diagnosis.
In this case, we believe that the etiology is rheumatoid arthritis. As the clinical evolution has been satisfactory, we did not conduct other tests, nor the proposal in the literature for the excision of the affected tendon sheath. However, we are closely following the evolution of the clinical picture, which continues without recurrences and with good recovery of joint movements after two years of follow-up.
Isabella Zurita Dehó 0000-0002-2884-7073
Preparation and writing of the manuscript.
Jayme de Oliveira Filho 0000-0003-0239-0981
Approval of the final version of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Irina Andrea Pires Afonso 0-000-0001-6787-8529
Author’s contribution: Approval of the final version of the manuscript; preparation and writing of the manuscript.
Anna Rita Ferrante Mitidieri de Oliveira 0000-0002-5551-7440
Approval of the final version of the manuscript.
1. Campos LR, Sztajnbok FCN, Galvão S, Lessa MA, Aymoré IL, et al. Presence of riziform bodies in a patient with juvenile idiopathic arthritis: case report and literature review. Rev Bras Reumatol Engl Ed. 2017;57(6):610-2.
2. Subramaniam R, Tan JW, Chau CY, Lee KT. Subacromial bursitis with giant rice bodies as initial presentation of rheumatoid arthritis. J Clin Rheumatol. 2012;18(7):352-5.
3. Reda FM, Talal G, Moncef B, Reda-Allah B, Omar LM, Saleh BM. Mass of the thenar eminence hiding idiopathic massive rice bodies formation with a compression of the median nerve: case report and review of the literature. Int J Surg Case Rep. 2018;50:28-31.
4. Cheung HS, Ryan LM, Kozin F, McCarty DJ. Synovial origins of Rice bodies in joint fluid. Arthritis Rheum. 1980;23(1):72-6.
5. Popert AJ, Scott DL, Wainwright AC, Walton KW, Williamson N, Chapman JH. Frequency of occurrence, mode of development, and significance or rice bodies in rheumatoid joints. Ann Rheum Dis. 1982;41(2):109-17.
6. Karaoğlu S, Karaaslan F, Mermerkaya MU. A mechanically locked knee joint due to free-floating flake-shaped rice bodies: a case report. Acta Orthop Traumatol Turc. 2015;49(5):565-7.
7. Matcuk Jr GR, Patel DB, Lefebvre RE. Horseshoe abscess of the hand with rice bodies secondary to mycobacterium avium intracellulare infection. Clin Imaging. 2020;63:24-9.
8. Saraya T, Fukuoka K, Maruno H, Komagata Y, Fujiwara M, Kaname S. Tenosynovitis with rice body formation due to mycobacterium intracellulare infection after initiation of infliximab Therapy. Am J Case Rep. 2018;19:656-62.
9. Cegarra-Escolano M, Jaloux C, Camuzard O. Rice-body formation without rheumatic disease or tuberculosis in a "sausage" ring finger. Hand Surg Rehabil. 2018:S2468-1229(18)30067-7.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}