


Lara Xavier Bazotti; Leticia Maoletti Teixeira; Ana Paula Naspolini
Financial support: None
Conflict of interest: None
Submitted on: 05/05/2021
Approved on: 05/08/2021
How to cite this article: Bazotti LX, Teixeira LM, Naspolini AP. Risk factors correlated with frontal fibrosing alopecia in Criciuma, Santa Catarina: a case-control study. Surg Cosmet Dermatol. 2022;14:e20220042
INTRODUCTION: Fibrosing Frontal Alopecia (FFA) is a form of scarring alopecia, in which patients have an irreversible loss of hair follicles, especially in the frontal and temporoparietal regions. The etiopathogenesis is not fully understood, although hypotheses about genetic, hormonal, and behavioral factors, such as the use of sunscreen and facial moisturizers, have already been described.
METHODS: A case-control study was conducted using an objective questionnaire with 33 questions. Sixty women were evaluated, 30 diagnosed with FFA, and 30 not affected by the disease.
RESULTS: The mean age of the sample was 64 years old. 76.7% of patients with FFA and 23.3% of controls used facial sunscreen and the difference was statistically significant (p<0.001). Also, the use of facial moisturizer was significantly higher in patients with alopecia (63.3%) when compared to controls (33.3%; p=0.038). The frequency of use of regular soap on the face was significantly lower in patients with FFA (46.7%) when compared to the control group (83.3%; p=0.006).
CONCLUSION: Results suggest a possible association between FFA and the use of facial products, such as sunscreen and moisturizer, in this population. All patients were menopausal, reinforcing the hormonal relationship with the disease.
Keywords: Alopecia; Contraceptives oral combined; Finasteride; Menopause; Tamoxifen
The term cicatricial alopecia represents a group of diseases characterized by replacing the follicular structure with fibrous tissue.1,2 Frontal Fibrosing Alopecia (FFA) is a scarring, marginal, and symmetrical alopecia along the frontal hair implantation line. First described by Axel Munthe in 1929,3 FFA may have been sporadic and ignored for more than six decades, until 1994, when Kossard published a series of cases with six women affected by the disease.4 In this report, the patients were Caucasian and menopausal, with a recess in frontal hair implantation line, associated with perifollicular erythema and complete reduction or loss of eyebrows. Since its discovery, there has been an increase in its incidence worldwide. There is even evidence suggesting that FFA is an evolving epidemic.5 However, it’s not known for sure whether this increase in the number of cases is due to better recognition of the disease by dermatologists or if there has been an increase in its incidence, since FFA has also been diagnosed in women in the pre-menopause and, more rarely, in men.6
The etiopathogenesis of FFA is not fully understood, although several hypotheses have been proposed. Among them, the genetic factor is relevant since there are cases in siblings and members of the same family,7 suggesting an autosomal dominant inheritance with incomplete dominance.8 The recent identification of genomic loci strongly associated with lichenoid inflammation and FFA reinforces this idea. The locus of most significant susceptibility appears to be 6p21, located in the HLA region. According to the literature, the risk of developing FFA seems to increase five times with the HLA-B class 07: 029 allele implantation.9 Still, a possible hormonal mechanism has already been raised due to its predominance in postmenopausal women or those using antiandrogenic therapy.10,11 The gamma peroxisome proliferator-activated receptor (PPAR-γ) has intense antifibrotic activity, and its decline may correlate with the FFA fibrogenic inflammatory process. The triggering factors that lead to PPAR-γ deficiency and consequent inflammation are still unknown.9 The environmental component can participate as an etiopathogenic factor in the disease, mainly due to the late appearance of symptoms in most cases.12 Environmental exposure through cosmetic habits using facial moisturizers, face foundation, sunscreens, and hair dyes contains components such as nanoparticles of titanium dioxide, which has also been suggested to favor the development of FFA.13
The diagnosis of FFA can be clinical, guided by trichoscopy findings, such as perifollicular erythema and follicular hyperkeratosis, even before the final and permanent phase of evolution, with scarring alopecia.14 Histopathological evaluation is necessary in the early stages or cases of diagnostic doubt.15
FFA is a chronic condition that requires long-term treatment. Currently, there is no consensus on effective treatments.16 It is constantly associated with decreased quality of life mainly due to symptoms such as itching and scalp sensitivity, unsightly discomfort, and frustration about the inability to control the course of the disease.17
Given the importance of this clinical condition, a well-designed study that evaluates risk factors in patients diagnosed with FFA may help to clarify the characteristics predominantly involved in this pathology in our population. Therefore, this study aims to assess the factors correlated with FFA in patients assisted in private dermatological clinics in the municipality of Criciúma – SC, from July 2019 to April 2020.
The Research and Human Ethics Committee (3,938,659) of the Universidade do Extremo Sul Catarinense (UNESC) approved this study. After studying the agreement and signing the Free and Informed Consent Term, the patients agreed to participate, with their privacy and identification respected.
The present study was a case-control study conducted in 17 private dermatological clinics in the city of Criciúma, Santa Catarina, Brazil.
Sixty women living in the city of Criciuma (SC) were evaluated from July 2019 to April 2020. Thirty patients with clinical or histopathological diagnosis of FFA and thirty not affected by the disease were included in the control group after assessment by experienced dermatologists and pathologists. The inclusion criteria considered age over 18 years, follow-up by a dermatologist, FFA diagnosis in the case group, and not having alopecia in the control group. Patients undergoing chemotherapy, with questionnaires incorrectly filled out, and with pathologies that could present similar clinical symptoms (tinea capitis, seborrheic dermatitis, telogen effluvium, alopecia areata, other cicatricial alopecia, rosacea) were excluded from the study.
The research data were collected based on the application of an objective questionnaire composed of 33 questions, developed by the researchers and applied by the attending dermatologist.
The questionnaire was divided into two parts: the first part, directed to the specialist doctor, comprised questions on autoimmune diseases and skin allergies; and the second part, aimed at the patients, included queries to assess sociodemographic and behavioral parameters. The common questions for both groups addressed the frequency of the current use of sunscreen, face foundation, facial moisturizer, anti-residue shampoo, common soap on the face, as well as previous chemotherapy treatment, smoking, vegetarian or high-sugar diet, hair straightening or hair dye.
The hormonal history was evaluated by the presence of menopause, previous hysterectomy, use of tamoxifen, intrauterine device (IUD), or combined oral contraceptive pill (COCP). Regarding FFA, previous symptoms (burning, sensitivity, pruritus), treatments in use and perception of response to them, time between the onset of symptoms and diagnosis and quality of life (whether the patient considers or not to have been affected by the disease).
The data collected were analyzed using the software IBM Statistical Package for the Social Sciences (SPSS) version 21.0. Quantitative variables were expressed using the mean and standard deviation. Qualitative variables were expressed through frequency and percentage.
Statistical tests were performed with a significance level of α = 0.05 and 95% confidence. The distribution of data regarding normality was assessed using the Shapiro-Wilk test.
The comparison of the mean of the quantitative variables between the categories of the dichotomous qualitative variables was performed using the Mann-Whitney U test. The investigation of the existence of an association between qualitative variables was conducted by applying Fisher’s exact test and Pearson’s-chi-square test, followed by residue analysis when statistical significance was observed. The measure of the association strength used was the Odds Ratio (OR), obtained through binary logistic regression.
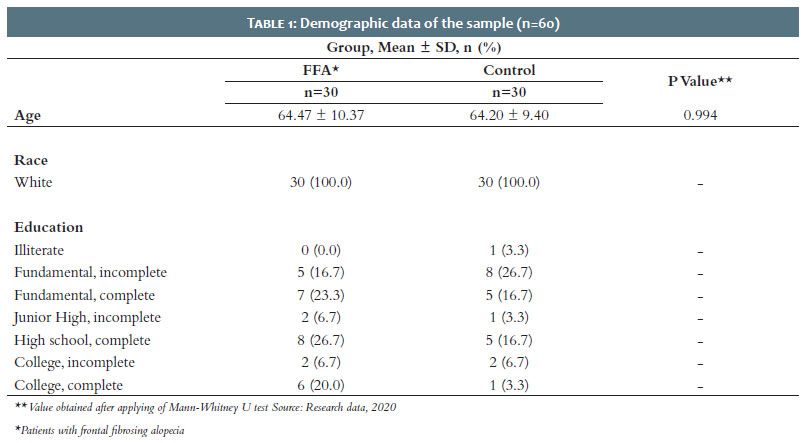
The total sample comprised 60 women, distributed in 30 cases and 30 controls. Table 1 shows the demographic data.
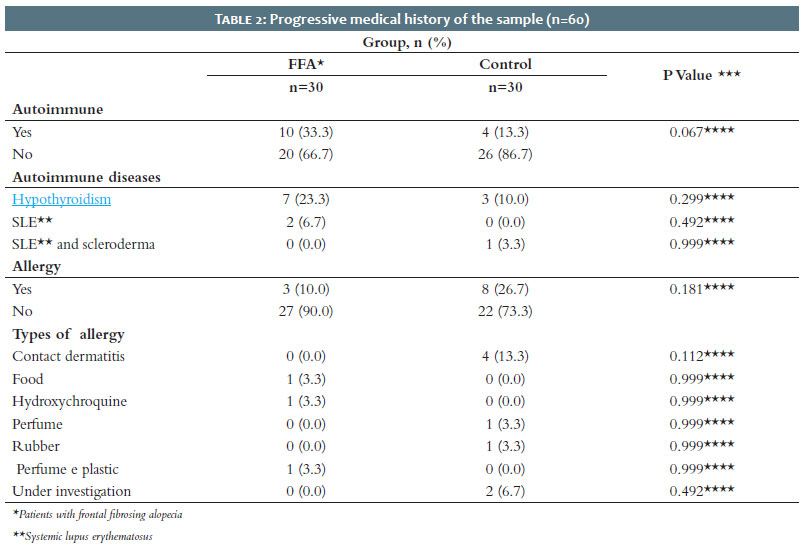
There was no statistical difference in the assessment of autoimmune diseases, such as hypothyroidism, systemic lupus erythematosus, and scleroderma (p = 0.299; p = 0.492, and p = 0.999 respectively – Table 2). No statistically significant difference was found regarding the presence of allergies, such as contact dermatitis or drug allergies (p = 0.112 and p = 0.999, respectively – Table 2).
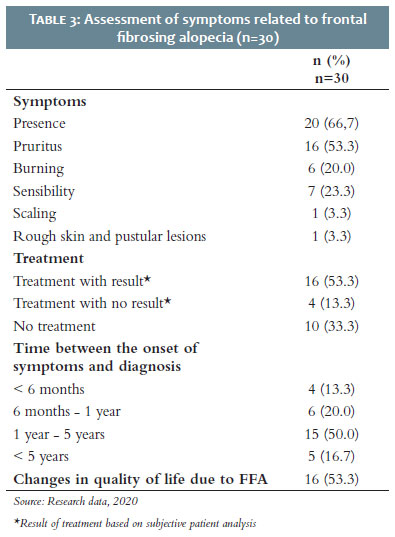
According to the evolution of symptoms related to FFA, 66.7% of cases reported their presence, with the most common symptom being pruritus (53.3%), followed by sensitivity (23.3%), and burning (20%). When asked about treatment, 53.3% reported improvement with treatment, 13.3% without improvement, and 33.3% without treatment at the time of assessment. The onset of clinical manifestations until diagnosis occurred between 1 to 5 years in 50% of cases, 6 months to 1 year in 20%, more than 5 years in 16.7%, and less than 6 months in 13.3 %. Still, 53.3% reported changes in quality of life due to FFA (Table 3).
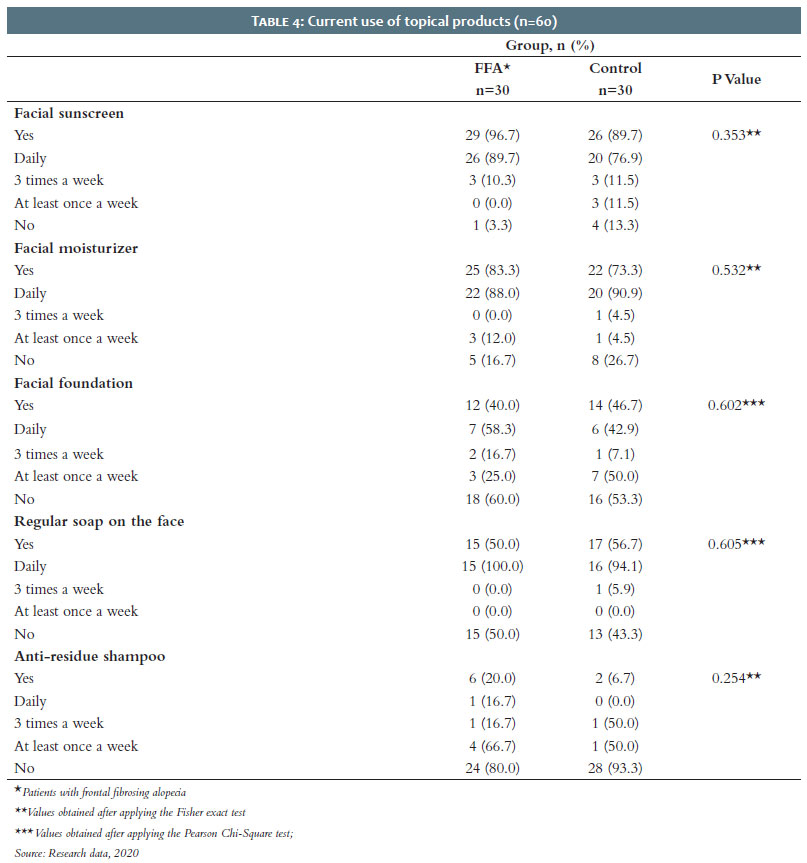
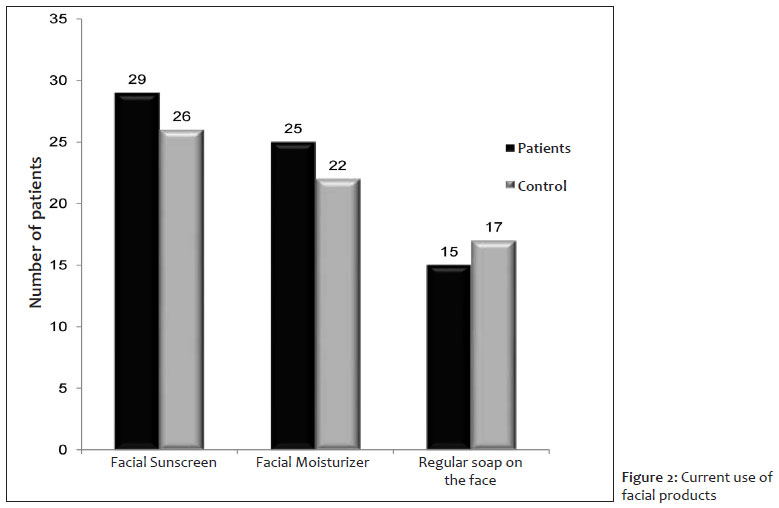
Regarding the use of topical facial products, there was no significant difference between the groups when assessing the current use of facial cosmetics, including the use of sunscreen, facial moisturizer, face foundation (makeup), regular soap on the face or anti-residue shampoo (p = 0.353; p = 0.532; p = 0.602; p = 0.605, and p = 0.254, respectively – Table 4).
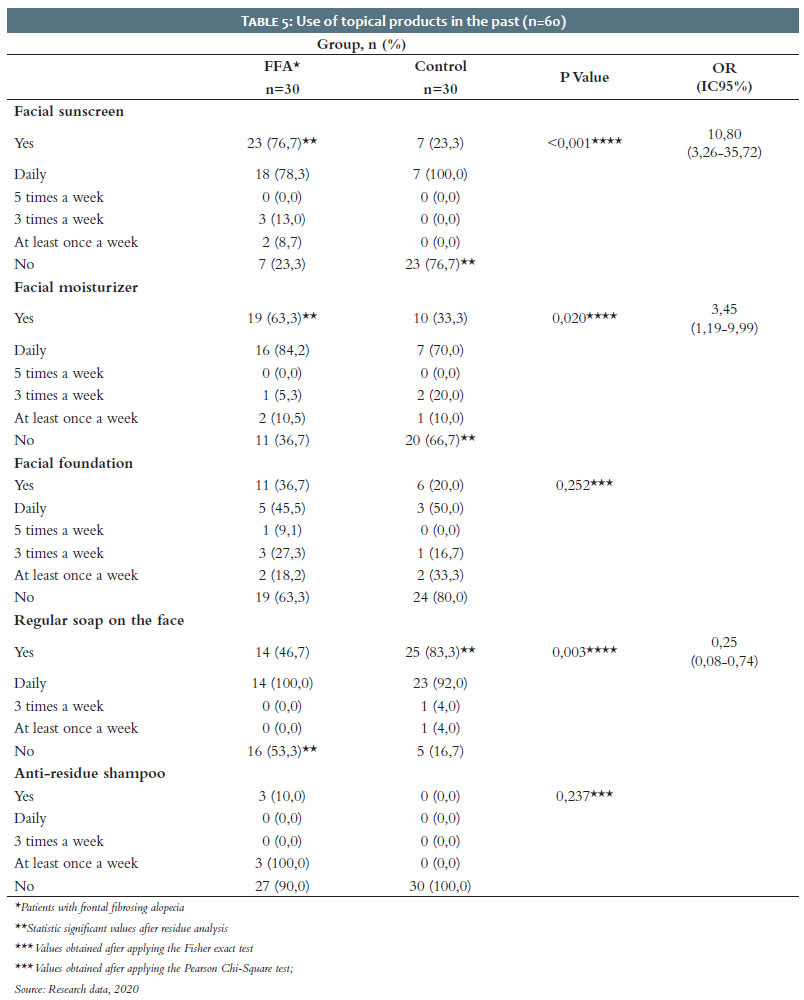
When asked about the previous use of the same substances, patients with FFA showed greater use of sunscreen (76.7%) when compared to the control group (23.3%). This difference is statistically significant (p <0.001 - Table 5). Also, 78.3% of patients with FFA used the product daily. Besides, the use of facial moisturizer also proved to be more present in patients with alopecia (63.3%) when compared to the control group (33.3%), with a statistically significant difference (p = 0.020- Table 5). Also, daily use was more frequent (84.2%) among patients with FFA. On the other hand, when analyzing the use of common soap on the face, a significantly lower use was observed in patients with FFA (46.7%) when compared to the control group (83.3%; p = 0.003) – it was again the daily use of the most frequent product (92%). Finally, using an anti-residue shampoo and face foundation in the past has not shown a statistically significant difference between groups (Table 5).
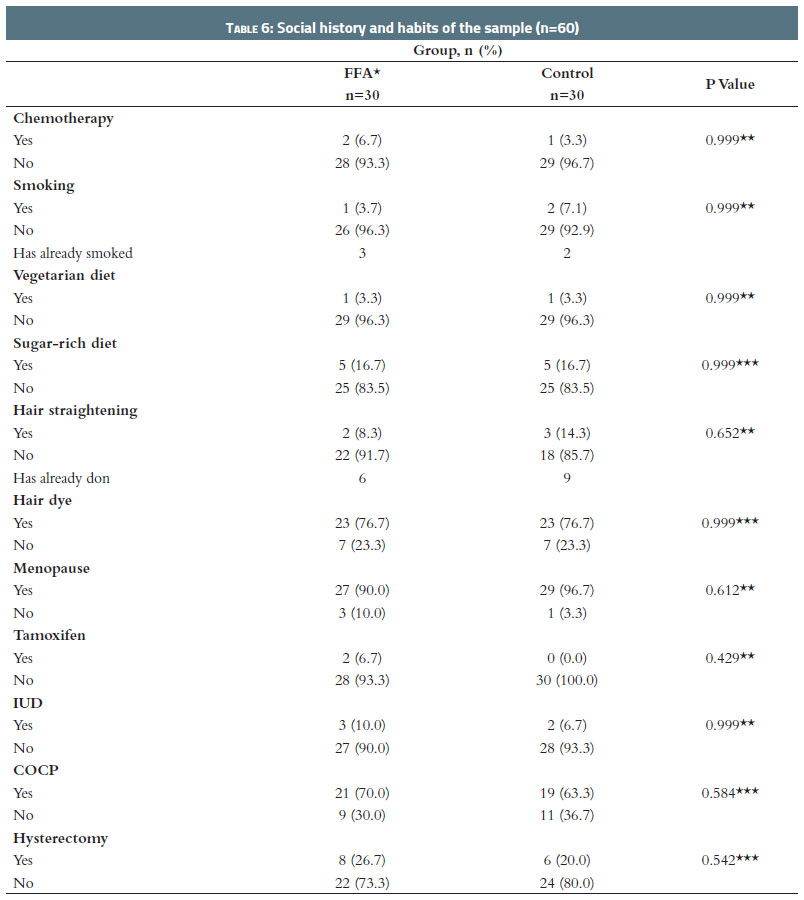
Table 6 shows the assessment of chemotherapy or tamoxifen use, vegetarian or high-sugar diet, straightening or dyeing the hair, as well as IUD or COCP use, smoking, menopause, and hysterectomy. None of the factors analyzed showed any difference in statistics when comparing the two groups.
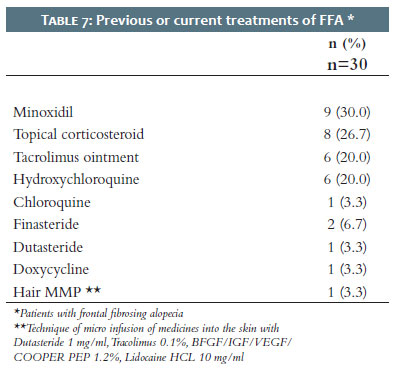
About the topical treatments used, 30% of patients with FFA used minoxidil, 26.7% used corticosteroids, and 20% used tacrolimus. Finally, as systemic therapy, 20% of patients received hydroxychloroquine and 6.7%, finasteride (Table 7).
The sample with FFA in the present study obtained, in its entirety, caucasian patients, probably because the southern region of the country has a higher prevalence of this population. According to IBGE,18 in 2010, about 84% of Santa Catarina’s citizens declared themselves white – the largest number in the country. However, it is known that FFA is found in all populations. A clinical review of 20 black patients in South Africa reinforced the scarcity of information on the epidemiology of FFA in this population and the difficulty in establishing a correct differential diagnosis between FFA and traction alopecia.19
Regarding age and gender, all study participants are women, with a mean age of 64 years (± 10.37 for cases and ± 9.40 for controls), 90% of them menopausal. In a cross-sectional study of 60 cases, the average age of participants at the presentation of FFA was 64 years.20 It is suggested that estrogens play an essential role in regulating the capillary cycle, producing a decrease in the growth of the hair strand, thus leading to the induction of the catagen phase prematurely and maintenance of the telogen phase.21 Thus, the estrogen decrease in menopause can alter the control of the capillary cycle and, in a way, predispose to the development of FFA. The post-menopausal women predominance in FFA, together with the reported efficacy of 5-alpha-reductase inhibitors in disease management, led to several theories about the role of sex hormones in the disease pathogenesis.16
In the analysis of the previous hysterectomy, we observed that a considerable number of women underwent the procedure, a finding also described by other authors,22 where 55 of the 139 patients analyzed reported the previous hysterectomy. Still, there was a sudden decrease in serum estrogen levels in patients undergoing surgical menopause on the hormonal relationship.22 Although more research is needed on hormonal pathogenesis, it is believed that its imbalance may be the trigger for the FFA inflammatory scar reaction in predisposed patients.13
In the present study, we found hypothyroidism in 23.3% and autoimmune diseases in 30% of patients with FFA, similar to the frequency observed in other studies.20 A systematic review of the literature showed that about 34.4% of the cohort of 1083 patients shared the polyautoimmunity phenomenon.23 This can be explained by the fact that genetic and environmental factors are similar among autoimmune diseases, which could lead to the development of concomitant autoimmune disorders.23,24
Regarding the quality of life, although questionnaires applied and validated are not used to evaluate the same, 53.3% of patients reported changes in quality of life by FFA. As mentioned by other authors,25,26 alopecia negatively affects the quality of life. It has been shown that older patients with FFA may be more likely to experience anxiety or depression, and patients with severe alopecia may feel powerless over the disease control.17
In the analysis between the clinic onset and diagnosis, 50% of patients reported that it occurred between 1 year and 5 years. Previous studies have found an average presentation time of 3.4 to 5.3 years.10,20 Eyebrow and eyelash loss may be the first sign of presentation of FFA.20,27,28 Although the frontal hair implantation line is more commonly affected, body hair may also be involved.2 The loss of body hair is usually confused or related to age and hardly reported by the patients themselves28,29,30, resulting in a delay in seeking medical care and, consequently, in treatment.
About the previous or current treatments for AFF, topical minoxidil, topical corticoid, tacrolimus ointment, hydroxychloroquine, and 5-alpha-reductase inhibitors were the most used by the participants. The literature brings all of these treatments as therapeutic options, but there is no curative treatment, and the lack of randomized clinical trials does not allow definitive conclusions about the most effective treatment.15
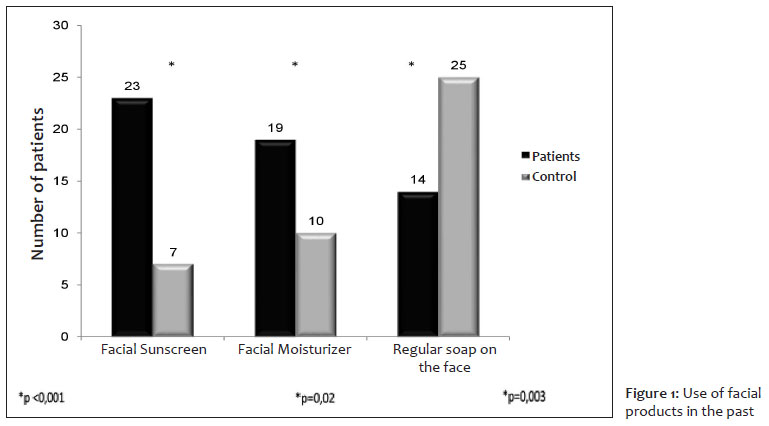
The analysis of the present study showed that women with FFA made more use of facial sunscreen than controls (Figure 1), a result similar to that demonstrated in a case-control study assessing 664 women and 106 British men.12 Regarding the sunscreen component, titanium dioxide nanoparticles have already been detected in the hair strand of a patient with FFA. This result was confirmed by another recent study,28 which also detected titanium dioxide in the hair from 16 of 20 FFA patients. Therefore, it is suspected that this molecule is involved in the pathogenesis of FFA. Because it is present in many of the sunscreens of routine use, it makes them a significant risk factor.31,32 On the other hand, some authors recognize that sunscreens cannot explain some FFA aspects.31,21 The fact that individuals in the general population use products with sunscreen and do not develop FFA, as well as patients with FFA do not use sunscreen regularly, and also the occipital involvement of FFA, where sunscreens would not normally be applied. A Brazilian case-control study with 902 participants found low adherence to the use of facial sunscreen in patients diagnosed with FFA, with no association with long-term use.33 Therefore, a true causal relationship between sunscreens and FFA cannot be concluded at this time.
Although the use of sunscreens by patients with FFA has not come close to universality, it is essential to note that many facial moisturizers are related to chemicals for sun protection.31 In the analysis of the present study, the frequency of isolated use of a facial moisturizer in the past was higher in patients with alopecia when compared to the control group (Figure 1). Similar values have been reported in the previously mentioned literature.10 Data like this corroborate an idea that facial products seem to be related to FFA.
It is worth mentioning that the greater use of these facial cosmetics (sunscreen and facial moisturizer) by patients with alopecia was not demonstrated when asked about the current use, that is, after FFA diagnosis (Figure 2). It is suggested that the decrease in use would be related to a typical response among patients with hair loss, as they relate the use of these products to hair loss, either through lay knowledge, through research, or even speeches by the health professional.31 The same reasoning may explain the lower adherence of FFA patients due to hair procedures and greater use of anti-residue shampoo by this group after the FFA diagnosis. In this case, the use of shampoo would be a typical response to the fact that patients relate the fall to the accumulated capillary waste, a fact also observed in our sample. These results show the importance of knowledge about the fundamental known risk factors for FFA, minimizing stressors, and investing in products with low effectiveness.
Other environmental factors were also analyzed, such as the diet followed by the patients. Only one of the patients with FFA followed a vegetarian diet. Some studies have already demonstrated the absence of a relationship between FFA and a diet rich in soy and its derivatives.13 However, a recent study32 demonstrated a possible relationship between the emergence of FFA and a diet rich in wheat and corn. Therefore, further studies are needed to confirm the causal relationship between dietary elements and the pathophysiology of FFA.
Regarding the use of tamoxifen, a study with 100 FFA patients raised the hypothesis that tamoxifen use may cause a loss of the estrogenic effect on regulation fibrosis and immunity.10 However, in our sample, only two patients with FFA used the previous one.
On the other hand, some literature suggests three protective factors for developing FFA, such as previous use of IUD,10 COCP,31 and previous or current smoking.33 These studies justified that the use is more commonly reported in patients not affected by the disease and a possible hormonal relationship related to their exposure. Also, a greater use of regular soap by the control group (83.3%) was observed in our study when compared to the case group (46 %) (Figure 1). Thus, it was not yet demonstrated in other studies, which can be understood as a protective factor since it would indicate greater facial hygiene, helping to remove topical products deposited in the follicle over the years.34 Therefore, more studies about the possible protective factors are needed.
The issues raised by the present study bring the need to conduct a well-designed multicenter study with a larger number of patients through long-term follow-up. The substantial result found in the use of facial products highlights the importance of studies that investigate the specific component of each one and its relationship with the disease. Still, the application of validated quality of life questionnaires could quantify the impact of the disease on the patients’ lives.
Lara Xavier Bazotti 0000-0002-1607-9257
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review.
Leticia Maoletti Teixeira 0000-0002-6307-933X
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation.
Ana Paula Naspolini 0000-0002-7201-5709
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Kossard S, Lee M-S, Wilkinson B. Postmenopausal frontal fibrosing alopecia: a frontal variant of lichen planopilaris. J Am Acad Dermatol.1997;36(1):59–66.
2. Ma SA, Imadojemu S, Beer K, Seykora JT. Inflammatory features of frontal fibrosing alopecia. J Cutan Pathol.2017;44(8):672–6.
3. TRUEB, Ralph. A comment on frontal fibrosingalopecia (Axel Munthe's Syndrome). Int J Trichology. 2016;8(4):203–5.
4. Kossard S. Postmenopausal frontal fibrosingalopecia. Arch Dermatol.1994;130(6):770-4.
5. Mirmirani P, Tosti A, Goldberg L, Whiting D, Sotoodian B. Frontal fibrosingalopecia: an emerging epidemic. Skin Appendage Disord. 2019;5(2):90-3.
6. Rácz E, Gho C, Moorman PW, NoordhoekHegt V, Neumann HA. Treatment of frontal fibrosing alopecia and lichen planopilaris: a systematic review. J Eur Acad Dermatol Venereol. 2013;27(12):1461-70.
7. Dlova N, Goh C-L, Tosti A. Familial frontal fibrosing alopecia. Br J Dermatol.2013;168(1):220–2.
8. Tziotzios C, Stefanato CM, Fenton DA, Simpson MA, McGrath JA. Frontal fibrosing alopecia: reflections and hypotheses on aetiology and pathogenesis. Exp Dermatol. 2016;25(11):847-52.
9. Tziotzios C, Petridis C, Dand N, Ainali C, et al. Genome-wide association study in frontal fibrosing alopecia identifies four susceptibility loci including HLA-B* 07:02. Nat Commun. 2019;10(1):1150.
10. Vañó-Galván S, Molina-Ruiz AM, Serrano-Falcón C, Arias-Santiago S, Rodrigues-Barata AR, Garnacho-Saucedo G, et al.Frontal fibrosing alopecia: a multicenter review of 355 patients. J Am Acad Dermatol. 2014;70(4):670-8.
11. Buendía-Castaño D, Saceda-Corralo D, Moreno-Arrones OM, Fonda-Pascual P, Alegre-Sánchez A, Pindado-Ortega C, et al. Hormonal and gynecological risk factors in frontal fibrosingalopecia: acase-control study. Skin Appendage Disord. 2018;4(4):274-6.
12. Katoulis AC, Diamanti K, Sgouros D, Liakou AI, Bozi E, Avgerinou G, et al. Is there a pathogenetic link between frontal fibrosing alopecia, androgenetic alopecia and fibrosing alopecia in a pattern distribution? J Eur Acad Dermatol Venereol. 2018;32(6):e218-e20.
13. Moreno-Arrones OM, Saceda-Corralo D, Rodrigues-Barata AR, Castellanos-González M, Fernández-Pugnaire MA, Grimalt R, et al. Risk factors associated with frontal fibrosing alopecia: a multicentre case-control study. ClinExpDermatol. 2019;44(4):404-10.
14. Waśkiel A, Rakowska A, Sikora M, Olszewska M, Rudnicka L. Trichoscopy in lichen planopilaris: an update. Dermatol Rev. 2018;105(1):63-75.
15. Miteva M, Tosti A. Dermoscopy guided scalp biopsy in cicatricial alopecia. J Eur Acad Dermatol Venereol. 2013;27(10):1299-303.
16. Iorizzo M, Tosti A. Frontal fibrosingalopecia: an update on pathogenesis, diagnosis, and treatment. Am J Clin Dermatol. 2019;20(3):379-90.
17. Saceda-Corralo D, Pindado-Ortega C, Moreno-Arrones ÓM, Fernández-González P, Rodrigues-Barata AR, Jaén-Olasolo P, et al. Health-related quality of life in patients with frontal fibrosing alopecia. JAMA Dermatol. 2018;154(4):479-80.
18. Instituto Brasileiro de Geografia e Estatística [homepage na internet]. Pesquisa Nacional por Amostra de Domicílios: síntese de indicadores 2011 [Acessed 04 mai 2020]. Available from: http:www.ibge.gov.br
19. Dlova NC, Jordaan HF, Skenjane A, Khoza N, Tosti A. Frontal fibrosing alopecia: a clinical review of 20 black patients from South Africa. Br J Dermatol. 2013;169(4):939-41.
20. MacDonald A, Clark C, Holmes S. Frontal fibrosing alopecia: a review of 60 cases. J Am Acad Dermatol. 2012;67(5):955-61.
21. Hu HM, Zhang SB, Lei XH, Deng ZL, Guo WX, Qiu ZF, et al. Estrogen leads to reversible hair cycle retardation through inducing premature catagen and maintaining telogen. PLoS One. 2012;7(7):e40124.
22. Imhof RL, Chaudhry HM, Larkin SC, Torgerson RR, Tolkachjov SN. Frontal fibrosingalopecia in women: the mayo clinic experience with 148 patients, 1992-2016. Mayo Clin Proc. 2018;93(11):1581-8.
23. Rojas-Villarraga A, Amaya-Amaya J, Rodriguez-Rodriguez A, Mantilla RD, Anaya JM. Introducing polyautoimmunity: secondary autoimmune diseases no longer exist. Autoimmune Dis. 2012;2012:254319.
24. Chiang YZ, Bundy C, Griffiths CE, Paus R, Harries MJ. The role of beliefs: lessons from a pilot study on illness perception, psychological distress and quality of life in patients with primary cicatricial alopecia. Br J Dermatol. 2015;172(1):130-7.
25. Ladizinski B, Bazakas A, Selim MA, Olsen EA. Frontal fibrosing alopecia: a retrospective review of 19 patients seen at Duke University. J Am Acad Dermatol. 2013;68(5):749-55.
26. Samrao A, Chew AL, Price V. Frontal fibrosing alopecia: a clinical review of 36 patients. Br J Dermatol. 2010;163(6):1296-300.
27. Moreno-Arrones OM, Saceda-Corralo D, Fonda-Pascual P, Rodrigues-Barata AR, Buendía-Castaño D, Alegre-Sánchez A, et al. Frontal fibrosing alopecia: clinical and prognostic classification. J Eur Acad Dermatol Venereol. 2017;31(10):1739-45.
28. Miteva M, Camacho I, Romanelli P, Tosti A. Acute hair loss on the limbs in frontal fibrosing alopecia: a clinic pathological study of two cases. Br J Dermatol. 2010;163(2):426-8.
29. Thompson CT, Chen ZQ, Kolivras A, Tosti A. Identification of titanium dioxide on the hair shaft of patients with and without frontal fibrosing alopecia: a pilot study of 20 patients. Br J Dermatol. 2019;181(1):216-7.
30. Aerts O, Bracke A, Goossens A, Meuleman V, Lambert J. Titanium dioxide nanoparticles and frontal fibrosing alopecia: cause or consequence? J Eur Acad Dermatol Venereol. 2019;33(1):e45-e6.
31. Aldoori N, Dobson K, Holden CR, McDonagh AJ, Harries M, Messenger AG. Frontal fibrosing alopecia: possible association with leave-on facial skin care products and sunscreens; a questionnaire study. Br J Dermatol. 2016;175(4):762-7.
32. Rudnicka L, Rakowska A. The increasing incidence of frontal fibrosing alopecia. In search of triggering factors. J Eur Acad Dermatol Venereol. 2017;31(10):1579-80.
33. Ramos PM, Anzai A, Duque-Estrada B, Farias DC, Melo DF, Mulinari-Brenner F, et al. Risk factors for frontal fibrosing alopecia: A case-control study in a multiracial population. J Am Acad Dermatol. 2021;84(3):712-8.
34. Gamret AC, Potluri VS, Krishnamurthy K, Fertig RM. Frontal fibrosing alopecia: efficacy of treatment modalities. Int J Womens Health. 2019 29;11:273-85.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}