


Shishira R Jartarkar1; Swayamsidda Mishra2; Manjunath KG1; Spoorthy B1
Financial support: None
Conflict of interest: None
Submitted on: 17/05/2021
Approved on: 04/06/2021
How to cite this article: Jartarkar SR, Manjunath KG, Mishra S, Spoorthy B. Intralesional vitamin D in multiple recurrent plantar warts - A single blind, prospective, placebo controlled study. Surg Cosmet Dermatol. 2021;13:e20210050
INTRODUCTION: Warts or verrucae, caused by the human papillomavirus (HPV), are a benign epidermal proliferation of the skin. Most patients seek medical advice as warts are cosmetically unacceptable and can be painful. Plantar warts, in particular, are typically refractory to treatment requiring multiple treatment sessions. High recurrence rates, pain, and scarring limit the available therapeutic modalities. In contrast, immunotherapeutic approaches stimulate the host immune system by enhancing cellular immunity to eliminate the virus.
OBJECTIVE: To assess the safety and efficacy of intralesional vitamin D3 injection to treat multiple recurrent plantar warts.
METHODS: 60 patients with multiple recurrent warts were divided into two groups of 30 each. Group 1 received 0.5 ml intralesional vitamin D in the base of the largest wart, and Group 2 received 0.5 ml of normal saline. The sessions were repeated every two weeks for a maximum of four sessions, and patients were followed up for 12 months to detect any recurrences.
RESULTS: The study group showed complete clearance in 73.3% (22) individuals, while most controls (70%) showed no response.
CONCLUSION: Intralesional vitamin D3 is a safe and effective treatment option for multiple recurrent plantar warts.
Keywords: Cellular immunity; Injections, intralesional; Warts
Warts or verrucae are a benign epidermal proliferation of the skin caused by the human papillomavirus (HPV). As it is highly infectious, some people experience HPV infection at some point in their life.1,2 Based on their form and site, warts are classified into verruca vulgaris, verruca plana, verruca plantaris, filiform/digitate warts, myrmecia, subungal/periungal warts, anogenital warts, and mosaic warts.3
Although 60-65% of warts resolve spontaneously by two years, most patients seek medical advice as warts are cosmetically unacceptable and can be painful at specific sites, such as plantar warts.1 Plantar warts, in particular, are typically refractory to treatment requiring multiple treatment sessions.4 Several therapeutic modalities are available such as medical agents (5-fluorouracil, podophyllotoxin, salicylic acid, oral zinc and ranitidine, cytodestructive methods (electrocautery, cryotherapy, photodynamic therapy), and surgical excision. High recurrence rates, pain, and scarring limit these modalities. Also, they are not suitable for multiple refractory warts.5,6 In contrast, immunotherapeutic approaches stimulate the host immune system by enhancing cell-mediated immunity to eliminate the virus rather than only clearing the lesions.6,7 Immunotherapy leads to warts clearance without scarring or physical changes and augments the host response against the causative agent.8 Various antigens have been tried, such as measles, mumps, and rubella vaccine (MMR), also purified protein derivative (PPD) and candida antigen. Few studies used topical vitamin D.9-12
The effect of vitamin D derivatives on warts is speculated to be derived from its potential to regulate epidermal cell proliferation and differentiation and modulate cytokine production. Upregulation of vitamin D receptors (VDR) in the skin leads to the induction of antimicrobial peptides.9-12
Our study aims to evaluate the safety and efficacy of intralesional vitamin D3 injection in multiple recurrent plantar warts.
It is a hospital-based, single-blind, comparative, interventional study conducted in the Department of Dermatology outpatient clinic of the Medical Sciences and Research Centre, Bengaluru - Karnataka - India from June 2018 to January 2020, after obtaining approval from our institutional ethics committee.
A total of 60 patients with multiple recurrent plantar warts were included in the study. Informed written consent was taken from each participant in the study.
Patients with multiple recurrent plantar warts of different sizes and duration with/out distant warts willing to provide informed written consent were included in the study.
Children <12 years, pregnant and lactating women, and patients with keloidal tendency, any evidence of immunosuppression, systemic or dermatological disorder, or prior hypersensitivity to vitamin D3 or any drug, were excluded from the study.
We randomly assigned patients into two groups of 30 each using the “chit box” method.
All the patients were subjected to a standard protocol that included complete history and systemic and cutaneous examination.
Complete history included demographic data (name, age, gender, address, occupation), and present history (disease duration, presence or absence of distant warts, drug intake, or systemic illness).
Cutaneous examination comprised assessing number and size of plantar warts, as well as presence or absence of distant warts. Dermoscopy was performed to diagnose plantar warts in doubtful cases.
We conducted a thorough general and systemic examination to exclude any systemic diseases.
Under asepsis, 0.5 ml of vitamin D3 (6lakh IU) was injected intralesionally into the base of the largest wart with an insulin syringe.
Under asepsis, 0.5 ml of normal saline was injected into the base of the largest wart.
The lesions were cleaned with povidone-iodine and spirit. We applied the injections into the base of the largest wart using a 40U insulin syringe. The syringe was held parallel to the skin surface, and the needle was held with the bevel facing upwards while injecting. The injection was repeated into the same wart every session. The session was repeated every two weeks in both groups, similarly, until complete clearance or for a maximum of four sessions. Patients were followed up for 12 months after the last dose to detect recurrences. We assessed patients for warts clearance and adverse events.
After each session, patients were advised to avoid using other lines of treatment during the study and follow-up period.
Assessment of improvement
We assessed the clinical improvement using color photographs at baseline, at each session, and after 12 months of the last session.
The clinical improvement was graded as complete clearance (complete resolution of warts), partial response (reduction in size/ number of warts but not complete clearance), no response (no change in size or number).
Statistical analysis
Data was analyzed using SPSS version 22 and represented as frequency and percentage for categorical variables, mean and standard deviation for quantitative variables. T-test and chi-square tests were used. P<0.05 was considered statistically significant.
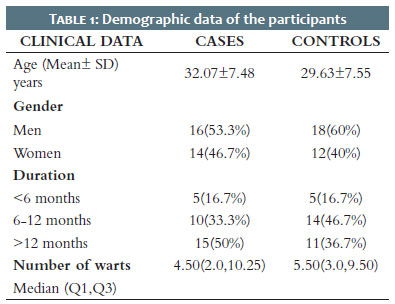
All 60 patients completed the study. Patients were comparable regarding age and sex distribution (p>0.05). The mean age in the study group was 32.1±7.48, and in controls, it was 29.6±7.55. In our study, we noticed a men predominance in both study (53.3%) and control groups (60%). Table 1 presents the demographic data of the study participants.
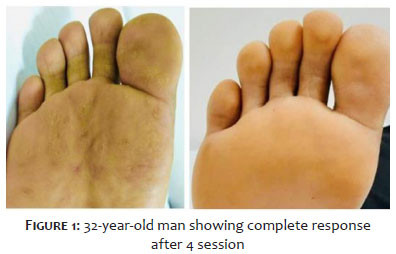
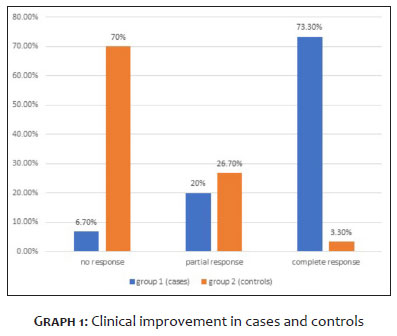
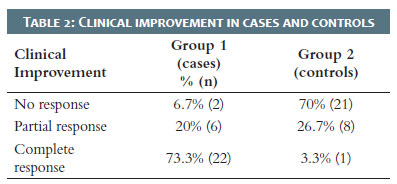
In the study group, we observed complete clearance in 73.3% (22) (Figure 1), partial clearance in 20% (6), and no improvement in 6.7% (2) of patients. In the control group, 70% (21) of patients showed no improvement, 26.7% (8) showed partial response, and 3.3% (1) showed complete response (Chart 1). The difference in improvement was statistically significant (p<0.01). We observed complete resolution of distant warts in all the patients who showed complete response (Table 2).
We noted pain during injection in all the patients in the study group and in 40% in the control group.
Persistent erythema and edema were observed in 3.3% of patients in the study group, which decreased spontaneously within 7-10 days. We followed patients for 12 months, and we observed recurrence in 6.7% (2) subjects in Group 1 during this period.
Recurrent multiple plantar warts constitute a frustrating disorder to patients and a challenge to practitioners, as no single therapy is completely effective in all patients, especially when it presents multiple lesions. Immunotherapy has been used as a preferred treatment as it is known to cause resolution of both treated and distant warts by inducing HPV targeted immunity.13 The exact mechanism of vitamin D activity against warts remains to be elucidated.14 However, it is known to control cell proliferation and differentiation and as is known to have immunoregulatory activities. Its effects are mediated via vitamin D receptor (VDR), which is present in the keratinocytes, fibroblasts, melanocytes and other skin’s immune cells.15 Upregulation of VDR leads to activation of Toll-like receptors of human macrophages and induction of antimicrobial peptide expressions as thymic stromal, lymphopoietin, and cathelicidin. It also acts as an anti-inflammatory by reducing the synthesis of IL1alpha and IL6.16
Our study revealed that intralesional vitamin D3 is an effective therapy for multiple recurrent plantar warts with a success rate of 73.3%, as 22 out of 30 patients had complete clearance of plantar warts. This was in concordance with a study by Aktas et al.,4 who reported total clearance in 80% (16 out of 20) of plantar warts patients. Another study, by Raghukumar et al.,13 evaluated the effect of intralesional injection of vitamin D3 in 60 patients with various extragenital warts, showing complete response in 90% of cases.
During the follow-up period of 12 months, we observed recurrence in 6.7% of our study group. It agreed with Raghukumar et al.,13 who reported a recurrence rate of 3.33% during the six-month follow-up.
A randomized controlled trial by El-Sayed et al.17 compared the effectiveness of 0.2 ml intralesional vitamin D3 and 0.2 ml intralesional zinc sulfate every two weeks for a maximum of four sessions. It showed complete response of 62.9% with vitamin D and 71.4% with zinc sulfate.
A placebo-controlled study by Abdel Azim et al.14 showed total clearance of warts in 56.25% (18 out of 32) of patients with intralesional vitamin D3 in cutaneous warts. But our study showed a better response in plantar warts.
Another placebo-controlled study by Kareem et al.16 used 0.2 ml intralesional vitamin D once monthly for two sessions for common warts. It showed complete clearance in 45% of the patients. Our study presented better results, probably due to the increased number of sessions (four sessions) and the use of a higher dose (0.5 ml) of vitamin D3.
There were no significant adverse events observed in our study. The limitation of our study is the relatively small sample size.
Our study shows a beneficial role of intralesional vitamin D3 in multiple recurrent plantar warts. It is a simple, safe, cost-effective treatment modality with a low recurrence rate. However, larger case-control studies as well as in-vitro/in-vivo studies are needed to elucidate the exact mechanism of action of vitamin D3 in warts.
Shishira R Jartarkar 0000-0002-7016-6087
Approval of the final veårsion of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Manjunath KG 0000-0002-4956-0880
Statistical analysis, Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Swayamsidda Mishra 0000-0002-3645-523X
Statistical analysis; study design and planning; data collection, analysis, and interpretation; active participation in research orientation.
Spoorthy B 0000-0003-2283-8050
Statistical analysis; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation.
1. Sterling JC, Handfield-Jones S, Hudson PM; British Association of Dermatologists. Guidelines for the management of cutaneous warts. Br J Dermatol. 2001;144(1):4-11.
2. Tyring SK. Human papillomavirus infections: epidemiology, pathogenesis, and host immune response. J Am Acad Dermatol. 2000;43(1 Pt 2):S18-26.
3. Salman S, Ahmed MS, Ibrahim AM, Mattar OM, El-Shirbiny H, Sarsik S, et al. Intralesional immunotherapy for the treatment of warts: a network meta-analysis. J Am Acad Dermatol. 2019;80(4):922-30.
4. Aktaş H, Ergin C, Demir B, Ekiz Ö. Intralesional vitamin D injection may be an effective treatment option for warts. J Cutan Med Surg. 2016;20(2):118-22.
5. Bacelieri R, Johnson SM. Cutaneous warts: an evidence-based approach to therapy. Am Fam Physician. 2005 15;72(4):647-52.
6. Rivera A, Tyring SK. Therapy of cutaneous human papillomavirus infections. Dermatol Ther. 2004;17(6):441-8.
7. Thappa DM, Chiramel MJ. Evolving role of immunotherapy in the treatment of refractory warts. Indian Dermatol Online J. 2016;7(5):364-70.
8. Sinha S, Relhan V, Garg VK. Immunomodulators in warts: Unexplored or ineffective? Indian J Dermatol. 2015;60(2):118-29.
9. Moscarelli L, Annunziata F, Mjeshtri A, Paudice N, Tsalouchos A, Zanazzi M, et al. Successful treatment of refractory wart with a topical activated vitamin d in a renal transplant recipient. Case Rep Transplant. 2011;2011:368623.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}