


Giovana Serrão Fensterseifer1; Ana Letícia Boff2; Fernando Eibs Cafrune2
Financial support: None
Conflict of interest: None
Submitted on: 15/05/2021
Approved on: 03/09/2021
How to cite this article: Fensterseifer GS, Cafrune FE, Boff AL. Pigmented columns as a dermoscopy feature in a seborrheic keratosis associated with a squamous cell carcinoma. Surg Cosmet Dermatol. 2021;13:e20210049
INTRODUCTION: Seborrheic keratosis (SK) has the typical pigmented dermoscopy features such as fissures and ridges, fat fingers, and cerebriform patterns. Here we describe a case where pigmented columns (PC) were visualized on SK’s dermoscopy associated with a squamous cell carcinoma (SCC). Case presentation: We report a case of a lesion whose dermoscopy showed PC. Histopathological report showed well-differentiated SCC and associated SK. Discussion: The PC was visualized in an area of dendritic melanocytes in the epidermis, correlating with the pigmented SK component of the lesion. To our knowledge, this is the first time PC is described in SK´s dermoscopy.
Keywords: Carcinoma squamous cell; Dermoscopy; Skin neoplasms.
Seborrheic keratosis (SK) has the typical pigmented dermoscopy features such as fissures and ridges, fat fingers, and cerebriform patterns. Here we describe a case where pigmented columns (PC), not characterized as any of the pigmented structures mentioned before, were visualized at dermoscopy. The histopathological report revealed a squamous cell carcinoma (SCC) with SK associated.
A 66-year-old man presented to the clinic reporting recent growth and bleeding of a lesion he has had for a few years. The patient had no previous history of skin cancer. Physical examination revealed a 1cm-brownish plaque with hemorrhagic crust on the preauricular area. Dermoscopy showed milium cyst-like structures in the posterior portion of the lesion, a hemorrhagic crust inferiorly and, superiorly, a blue-white veil followed by PC at the top of the lesion. (Figure 1).
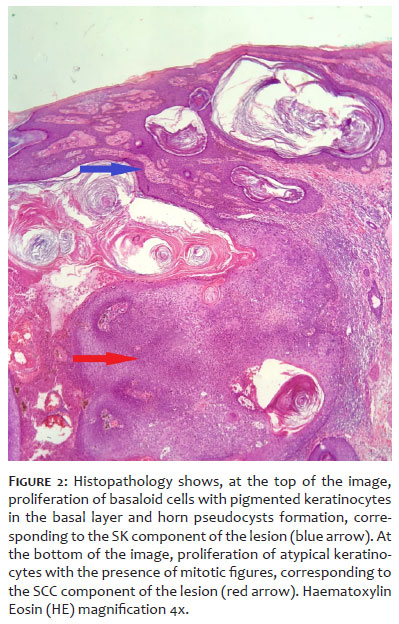
We performed the excisional biopsy. The histopathological report showed well-differentiated SCC with clear surgical margins and associated SK (Figure 2). The patient has been followed for three years with no signs of lesion recurrence to date.
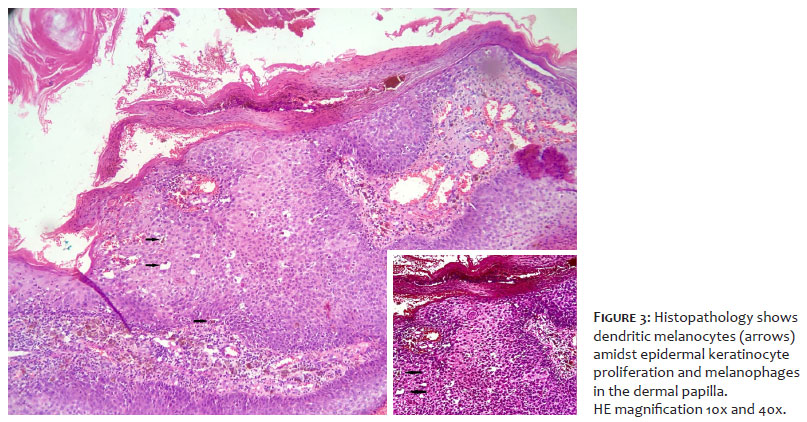
Regarding SCC dermoscopy structures, one can find polymorphous vessels. If ulceration and blood crusts are present, these appear as reddish to brownish or black blotches on the surface of the tumor. Pigmented invasive SCC is rare, and, on dermoscopy, it is characterized by a diffuse, homogeneous blue pigmentation with irregularly distributed blue-gray granular structures.1; In this case, the PC at the lesion’s periphery intrigued us. Fissures and ridges, fat fingers, and cerebriform patterns are the well-known pigmented dermoscopy structures in SK. In histopathology, they correlate to wedge-shaped clefts of the surface of the epidermis often filled with keratin. In our case, we visualized these PC in an area of dendritic melanocytes seen amidst basaloid keratinocytes in the acanthotic epidermis, correlating with the pigmented SK component of the lesion (Figure 3).
Besides this exciting finding in the SK dermoscopy, our case consisted of an SK with malignant transformation into an invasive SCC. It’s a rare event, considering that the transformation into an in situ SCC is much more common than into an invasive SCC. According to Vun et al., in a retrospective study of 813 histological specimens reported as seborrheic keratosis, 43 were associated with non-melanoma skin cancer. Among these, 36 were associated with squamous cell carcinoma in situ, and only two were associated with invasive squamous cell carcinomas.2; To our knowledge, this is the first time these dermoscopy structures (PC) are described in an SK. Further studies are necessary to determine its prevalence and to analyze its exact histopathology correlation.
Giovana Serrão Fensterseifer 0000-0002-1093-1250
Preparation and writing of the manuscript; critical literature review.
Fernando Eibs Cafrune 0000-0002-6645-0122
Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Ana Letícia Boff 0000-0002-5207-0567
Author's Contribution: Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Zalaudek I, Argenziano G. Dermoscopy of actinic keratosis, intraepidermal carcinoma and squamous cell carcinoma. Curr Probl Dermatol. 2015;46:70-6.
2. Vun Y, De'Ambrosis B, Spelman L, Muir JB, Yong-Gee S, Wagner G, et al. Seborrhoeic keratosis and malignancy: collision tumour or malignant transformation? Australas J Dermatol. 2006;47(2):106-8.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}