


Mariana M. Morita; Thomas S. P. Marcondes; Vidal Haddad-Jr; Hélio Amante Miot
Financial support: None
Conflict of interest: None
Submitted on: 05/05/2021
Approved on: 04/06/2021
How to cite this article: Morita MM, Marcondes TSP, Haddad-Jr V, Miot HA. Cryosurgery with liquid nitrogen versus trichloroacetic acid in the treatment of human papillomavirus (HPV) penile wart: a randomized controlled trial. Surg Cosmet Dermatol. 2021;13:20210041.
BACKGROUND: Anogenital warts are the most prevalent sexually transmitted infection (0.5%) among dermatological consultations. Cryotherapy with liquid nitrogen (LN) and therapy with trichloroacetic acid (TCA) are remarkable among the treatment strategies.
OBJECTIVE: To evaluate the effectiveness of LN versus TCA in to treat penile warts in patients from a Brazilian public institution.
METHODS: Open, parallel, randomized clinical trial. Following randomization, the warts were counted and submitted to cryotherapy (10s) or case therapy (TCA 80%) in each visit. The primary dependent variable was the lesion count before and after four weeks of treatment. We assessed the following variables: complete clearance, age, immunosuppression, smoking, topography, and education.
RESULTS: 142 treatments were evaluated in 52 participants. There was a predominance of young adults, and the main topography affected was the penis shaft. The mean reduction rate per session was 48% for LN and 26% for TCA (p=0.11). 42 (81%) participants achieved complete clearance, with 39 (75%; 95% CI: 64-85%) reaching clearance in up to three sessions. Age was associated with a worse therapeutic response rate (ß =-0.09; p<0.01).
CONCLUSIONS: LN and TCA proved to be effective to treat penile warts, without difference between treatments. Age was associated with a worse therapeutic response.
Keywords: Trichloroacetic acid; Cryosurgery; Sexually transmitted diseases; Papillomavirus infections; Warts
Despite the vaccination campaign, anogenital warts (AGWs) remain a prevalent sexually transmitted infection (0.5%) among dermatological care.1 The human alpha papillomavirus (HPV) causes AGWs, usually genotypes 6 and 11. It has a low-oncogenic risk but may present co-infection with high-risk genotypes. In addition to the critical link between contagion and impact on quality of life, HPV can induce epithelial neoplasms, especially in immunocompromised individuals.2,3
Among the therapeutic strategies used in AGW treatment, clinical therapy (e.g., imiquimod, podophyllotoxin) and surgical options, especially electrocoagulation, cryotherapy with liquid nitrogen (LN), and treatment with trichloroacetic acid (TCA) 80-90% stand out due to their accessibility and no need for anesthesia. There is no hierarchy of treatments, and few randomized studies compare the effectiveness of different strategies in AGW treatment. LN is associated with a 44-87% cure rate and TCA with 56-94%.4
This study aims to assess the effectiveness of LN versus TCA to treat penile warts in patients from a Brazilian public institution.
It is an open, parallel, randomized clinical trial involving patients with penile AGW. At each clinical visit, the AGW were counted and submitted to treatment with LN (10s) or TCA 80%, according to computerized randomization. Patients were re-assessed after four weeks, AGWs were recounted, and patients were re-enrolled in the study under further randomization if new treatments were needed. The primary dependent variable was AGW lesion count, assessed after acetoscopy (with acetic acid 5%), before treatment, and after four weeks. We also analyzed complete clearance, age, immunosuppression, smoking, topography (penis glans, shaft, foreskin), and education. The numerical variation of the lesions was evaluated using a generalized linear mixed-effect model (negative binomial). Outcomes were assessed by intention to treat (ITT). Participants who did not attend the re-evaluation visit were considered a therapeutic failure, and the mixed model imputed their results. Significance was defined as p values <0.05. The project was approved by the Research Ethics Committee (n. 4418.2012).
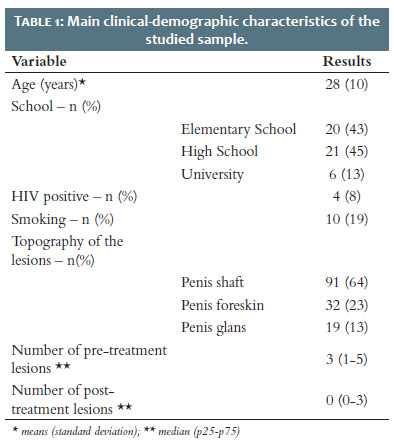
We assessed 142 treatments in 52 participants: 13 (9%) of the cases did not return for re-evaluation (drop out). Table 1 shows the primary clinical and demographic data of the sample. There was a predominance of young adults, low education, and the main affected topography was the penis shaft. Cauterization with TCA was indicated in 63 (44%) of the treatments, and 59 was completed; NL was indicated in 79 (56%) of the treatments, with 70 completed, with no difference between the groups regarding the drop out rate (p=0.82).
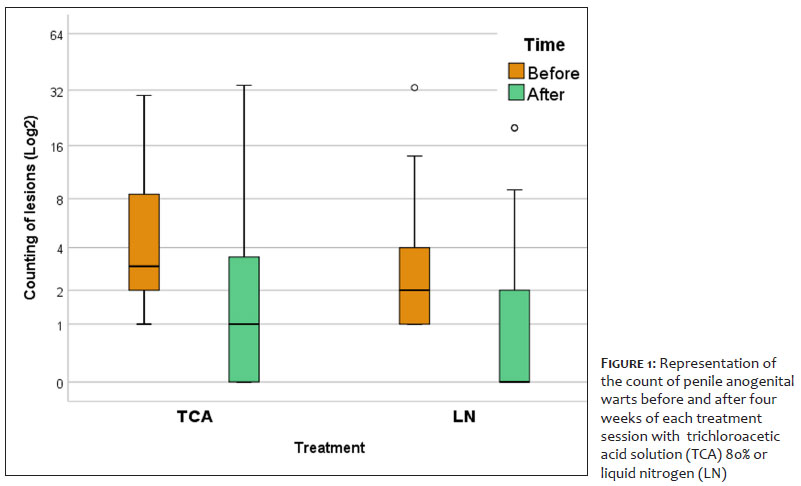
Figure 1 represents the AGW counts for each group and treatment time. There was a significant reduction in the median (p25-p75) of AGWs for both groups: TCA (3 [2-9] to 1 [0-4]; p<0.01) and LN (2 [1-4] to 0 [0-2]; p<0.01), with no differences between treatments (p=0.11). The mean percentage reduction in each session was 48% for LN and 26% for TCA.
Complete clearance (absence of acetowhite areas) was achieved by 42 (81%) study participants during follow-up, with 39 (75%; 95% CI: 64-85%) of all included participants achieving clearance within up to three monthly sessions. As the participants were re-included at each return in different treatment groups, assessing the complete clearance linked to each treatment was impossible.
When we assessed clinical-demographic elements as predictors of a general response to treatments, age (β= -0.09; p<0.01) was associated with the worst response rate. However, HIV carriers (p=0.99), education (p=0.51), smoking (p=0.17), and the topography of the lesions (p=0.24) did not interfere in the therapeutic response.
In a randomized clinical trial analyzing TCA 90% versus LN (swab) in lesions in both sexes, complete clearance in up to six sessions of TCA was 64%, and LN was 70%.5
A systematic review of randomized studies identified complete clearance of 72% for TCA therapy (six studies) versus 58% for LN (12 studies). However, the LN application regimen (spray versus swab), TCA concentration (80% versus 90%), and the number of sessions were not weighted.4
The present study has limitations because it is monocentric, depends only on clinical diagnosis, shows loss to follow-up of 9% of subjects included, does not have a quantitative assessment of immunity, and does not protocol follow-up with the same treatment type for each participant. Prospective studies should compare whether the combination of treatments (e.g., TCA+LN, TCA+imiquimod) or different regimens of LN or TCA 90% can lead to more robust results, reducing the number of sessions needed to clear genital HPV.
LN and TCA proved to be effective in treating AGW, with no difference between treatments. Age was a factor associated with a worse therapeutic response.
Mariana M. Morita 0000-0002-6396-7388
Approval of the final version of the manuscript; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Thomas S. P. Marcondes 0000-0002-4448-9595
Approval of the final version of the manuscript; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Vidal Haddad-Jr 0000-0001-7214-0422
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Hélio Amante Miot 0000-0002-2596-9294
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Miot HA, Penna GO, Ramos AMC, Penna MLF, Schmidt SM, Luz FB, et al. Profile of dermatological consultations in Brazil. An Bras Dermatol. 2018;93(6):916-28.
2. Leto Md, Santos Júnior GF, Porro AM, Tomimori J. Human papillomavirus infection: etiopathogenesis, molecular biology and clinical manifestations. An Bras Dermatol. 2011;86(2):306-17.
3. Camargo CC, D'Elia MPB, Miot HA. Quality of life in men diagnosed with anogenital warts. An Bras Dermatol. 2017;92(3):427-9.
4. Bertolotti A, Milpied B, Fouéré S, Cabié A, Dupin N, Derancourt C. Local management of anogenital warts in immunocompetent adults: systematic review and pooled analysis of randomized-controlled trial data. J Am Acad Dermatol. 2019;81(5):1203-4.
5. 5 Abdullah AN, Walzman M, Wade A. Treatment of external genital warts comparing cryotherapy (liquid nitrogen) and trichloroacetic acid. Sex Transm Dis. 1993;20(6):344-5.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}