


Francisco Milton da Silva Junior1; Marcelo Tavares Oliveira1; Luiz Carlos Angelini1; Wu Tu Chung2
Financial support: None
Conflict of interest: None
Submitted on: 29/04/2021
Approved on: 04/06/2021
How to cite this article: Silva Junior FM, Oliveira MT, Angelini LC, Chung WT. Treatment of hook nails using the Bakhach’s technique: a retrospective study. Surg Cosmet Dermatol. 2021;13:20210039
INTRODUCTION: The cause of the hook nail is the trauma of the hyponychium. The nail plate presents longitudinal hypercurvature of volar concavity, causing functional loss, aesthetics concerns, and pain.
OBJECTIVE: To evaluate the research results of 20 medical records of patients submitted to hook nail correction surgeries of traumatic etiologies.
METHODS: Epidemiological, cross-sectional, retrospective study of patients’ medical records who were submitted to Bakhach’s surgical technique, from 2010 to 2018, in the Hand Surgery Outpatient Clinic of the Hospital do Servidor Público Municipal de São Paulo.
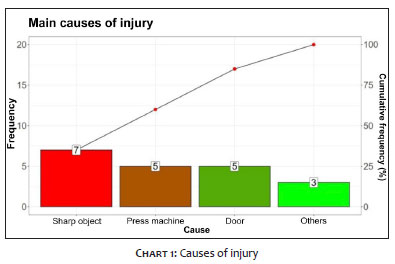
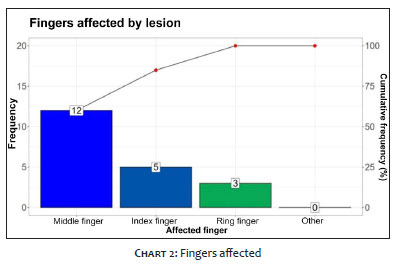
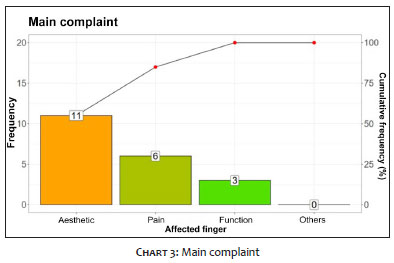
RESULTS: We analyzed 20 affected fingers: 7 were victims of accidents with sharp objects, 5 with press machines, 5 with doors, 1 with window, 1 with motorcycle, and 1 due to a dog bite. The finger with the highest incidence was the middle finger (n=12), followed by the index finger (n=5), and ring finger (n=3). The main complaint was aesthetics (n=11); pain (n=6), and functional (n=3). All cases had type II distal digital transverse amputations and underwent surgical treatment. The reconstruction surgery occurred between 4 and 25 months after the trauma.
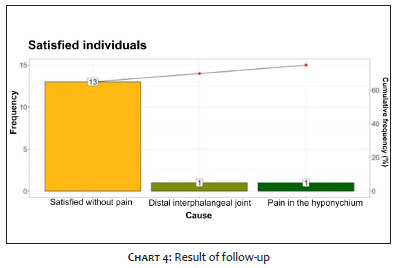
CONCLUSION: 15 patients were satisfied and two felt pain: one in the distal interphalangeal joint and the other in the hyponychium. The follow-up ranged from 6 months to 2 years.
Keywords: Finger injuries; Hand injuries; Nail diseases; Nails malformed
Amputations of the end of the distal phalanx can result in bone and tissue loss, making it difficult to close the wound. The hook nail is a deformity caused by traumatic injury to the hyponychium, and the nail plate presents a longitudinal hypercurvature with volar concavity. The patient complains of functional incapacity, aesthetic impairment, and pain.1-5
This study aims to demonstrate the necessity of Bakhach’s surgical technique for the functional rehabilitation of the affected finger of the hook nail with the esthetic satisfaction of the patient.
We assessed 20 medical records of patients treated at the Hand Surgery Outpatient Clinic of the Hospital do Servidor Público Municipal of São Paulo between 2010 and 2018. All patients presented hook nails with traumatic etiology. The Informed Consent Form (ICF) was not applied, considering the current coronavirus pandemic and the fact pointed out by the researchers that some surgeries were performed many years ago. Once the researchers explicitly committed to the secrecy and care with the confidentiality of the data, the research ethics committee considered the waiver of the informed consent pertinent.
According to the medical records, surgeries were performed under anesthesia, with an injection of 3 ml 2% lidocaine without epinephrine in the flexor tendon sheath. The tourniquet was performed using the finger of a glove. The nail plate was removed, and two lateral incisions were made on each side of the paronychia. Between these incisions, a rectangular skin graft was taken from the region proximal to the eponychium.4 The nail matrix was carefully separated from the phalanx, preserving the irrigation of the proximal portion. The nail matrix was reinserted proximally, with the distal interphalangeal joint as a limit. We used the “V-Y” flap, popularized by Atasoy,3 to reconstruct the hyponychium. Weekly dressings were performed, and the stitches were removed within 14 days (Figures 1 to 5).
Of the 20 fingers affected, 15 belonged to male patients and five to female patients. Seven patients were victims of accidents with sharp objects, five with press machines, five with doors, one with a window, one with a motorcycle, and one due to a dog bite (Chart 1).
The most affected finger was the middle (12), followed by the index (5) and the ring (3) (Chart 2).
The main complaint of patients was aesthetic (11), followed by pain (6), and function (3). Shows these results (Chart 3).
All patients had undergone type II transverse digital amputations and underwent urgent surgical treatment at different hospitals. Reconstructive surgery took place between four and 25 months post-trauma. We obtained a proximal repositioning of the nail bed ranging from 3 mm to 5 mm (10 patients with 5 mm, five with 4 mm, and five with 3 mm). No flap showed necrosis. The surgical time ranged between 30 and 55 minutes. Fifteen patients were satisfied with the result, although two remained in pain, one in the distal interphalangeal joint and the other in the hyponychium. Follow-up time ranged from six months to two years, and all patients returned to their normal activities (Chart 4).
Acute nail bed injuries must be cared for urgently and adequately, as established deformities are challenging to treat.1,6 The attempt to obtain coverage of the shortened bone of the distal phalanx by traction of the nail bed towards the digital pulp generates the deformity known as a hook nail. Some authors have described techniques with variable aesthetic results6,7,8 and/or that require sophistication for microsurgical reconstruction with tissue donated from the first or second toe.9,10 The method described by Bakhach1,2 proved to be efficient precisely for its practicality, low complication rate, and good clinical and aesthetic improvement in acute cases or its long evolution, as demonstrated in our series.
Numerous arterial branches originating from the distal dorsal digital arch irrigate the eponychium flap,1,2 allowing the safe elevation of the dermal-hypodermal flap. We obtained the replacement of the nail in a more proximal position (3 mm to 5 mm) similar to that obtained by Bakhach et al.2 This repositioning increases the area supported by the phalanx, favoring the growth of a nail plate with greater length and without longitudinal curvature. The V-Y advancement flap3 favored the reconstruction of the hyponychium and a better quality digital pulp.3, 10-13
The hook nails surgical treatment using the Bakhach technique is a safe surgical option, with good aesthetic and functional results.
Francisco Milton da Silva Junior 0000-0001-7914-2914
Study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Marcelo Tavares Oliveira 0000-0002-7090-861
Approval of the final version of the manuscript; study design and planning; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Luiz Carlos Angelini 0000-0001-6762-4270
Active participation in research orientation; critical revision of the manuscript.
Wu Tu Chung 0000-0002-9709-1177
Statistical analysis; critical literature review; critical revision of the manuscript.
1. Bakhach J. Le lambeau d'éponychium [Eponychial flap]. Ann Chir Plast Esthet. 1998;43(3):259-63.
2. Bakhach J, Demiri E, Guimberteau JC. Use of the eponychial flap to restore the length of a short nail: a review of 30 cases. Plast Reconstr Surg. 2005;116(2):478-83.
3. Atasoy E, Ioakimidis E, Kasdan ML, Kutz JE, Kleinert HE. Reconstruction of the amputated finger tip with a triangular volar flap. A new surgical procedure. J Bone Joint Surg Am. 1970;52(5):921-6.
4. Chiu DT. Transthecal digital block: flexor tendon sheath used for anesthetic infusion. J Hand Surg Am. 1990;15(3):471-7.
5. Foucher G, Merle M, Michon J. Les amputations digitales distales: de la cicatrisation dirigée au transfert microchirurgical de pulpe d'orteil. Indications et résultats [Distal digital amputations: from delayed healing to microsurgical transfer of the toe pulp. Indications and results]. Chirurgie. 1986;112(10):727-35.
6. Atasoy E, Godfrey A, Kalisman M. The "antenna" procedure for the "hook-nail" deformity. J Hand Surg Am. 1983;8(1):55-8.
7. Dufourmentel C. Problèmes esthétiques dans la reconstruction des moignons digitaux [Esthetic problems in the reconstruction of digital stumps]. Ann Chir. 1971;25(19):995-9.
8. Foucher G, Lenoble E, Goffin D, Sammut D. Le lambeau "escalator" dans le traitement de l'ongle en griffe [Escalator flap in the treatment of claw nail]. Ann Chir Plast Esthet. 1991;36(1):51-3.
9. Foucher G, Merle M, Maneaud M, Michon J. Microsurgical free partial toe transfer in hand reconstruction: a report of 12 cases. Plast Reconstr Surg. 1980;65(5):616-27.
10. Koshima I, Moriguchi T, Umeda N, Yamada A. Trimmed second toetip transfer for reconstruction of claw nail deformity of the fingers. Br J Plast Surg. 1992;45(8):591-4.
11. Foucher G, Merle M, Maneaud M, Michon J. Microsurgical free partial toe transfer in hand reconstruction: a report of 12 cases. Plast Reconstr Surg. 1980;65(5):616-27.
12. Cunha AL, Tania LT, Oliveira LO, Craviotto M. Retalho do eponíquio para alongamento ungueal: série de casos. Rev Bras Cir Plást. 2019;34 (Suppl. 1):67-9.
13. Cambon-Binder A, Le Hanneur M, Doursounian L, Masquelet AC, Sautet A. Eponychial flap refinement for the treatment of "hook-nail" deformity. J Plast Reconstr Aesthet Surg. 2017;70(7):979-81.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}