


Thessaly Puel de Oliveira; Hillani da Silva Andrade; José Roberto Pegas; Cristina Santos Ribeiro Bechara
Financial support: None
Conflict of interest: None
How to cite this article: Oliveira TP, Andrade HS, Pegas JR, Bechara CSR. Prevalence of pathological diagnoses and epidemiological profile of patients with non-melanoma skin cancer suspicious lesions. Surg Cosmet Dermatol. 2021;13:e20210031.
INTRODUCTION: Cutaneous cancer has a high incidence, can be screened with dermatological clinical examination and confirmed by cutaneous biopsy.
OBJECTIVE: To verify the prevalence of pathological diagnoses for suspected non-melanoma skin cancer (NMSC) lesions in a Reference Service.
METHODS: Observational and cross-sectional study. Patients with indication of skin biopsy for suspected NMSC were included. Variables analyzed: age, gender, personal history of skin cancer, number of biopsies, biopsy site, and pathological outcome, divided into Group 1 (neoplastic lesions); Group 2 (premalignant lesions), and Group 3 (benign lesions).
RESULTS: A total of 287 patients, with an average of 1.33 biopsies per patient. The median age in the sample was 71 years, and 56.1% were women. Personal history of skin cancer: 44.95%. General sample: group 1: 62%; group 2: 21% and group 3: 17%. Neoplasms found: 68% were BCC, 30% were SCC, and other neoplasms: 2%. In the group of premalignant lesions: mainly actinic keratosis; in the group of benign lesions: diagnostic variety. The cephalic segment was the most frequently biopsied topography (58%).
CONCLUSIONS: In this study, we showed a higher incidence of skin cancer in women, with the majority of elderly patients being the most frequent diagnosis of BCC.
Keywords: Basal Cell; Biopsy; Carcinoma; Neoplasms; Skin neoplasms; Squamous cell.
Skin cancer has gained special significance in recent decades due to its increasing incidence. It is considered a public health problem in geographic areas of intense exposure to ultraviolet radiation.1,2,3 Non-melanoma skin cancer (NMSC), represented by basal cell carcinoma (BCC) and squamous cell carcinoma (SCC), corresponds to 30% of all malignant tumors registered in the country. BCC accounts for 70% of skin cancer diagnoses, followed by SCC, diagnosed in 25% of cases.1
It is believed that 90% of NMSC can be attributed to sun exposure,4 and BCC is associated with cumulative exposure. This fact reinforces the importance of photoprotection, which should be introduced from childhood and is considered the measure of choice worldwide to prevent NMSC.5 Other causes related to the development of skin cancer are family history, exposure to chemicals, radiotherapies, phenotypic factors, immunosuppression, and some hereditary genetic syndromes.6
Diagnosis of skin cancer mainly involves clinical examination, conducted through visual inspection of the patient’s skin, and histopathological analysis after the lesion’s biopsy, which is indicated when a clinical study shows suspicion of NMSC or melanoma.7 A specialized professional must perform a thorough physical examination, identifying suspected malignant lesions through their clinical characteristics. Advances in dermoscopic studies of these lesions allowed higher precision in indicating skin biopsies for diagnostic confirmation.8,9,10
When detected early, BCC presents high cure rates.2,6 According to the National Comprehensive Cancer Network (NCCN), NMSC treatment should prioritize the complete cure of the tumor. The NCCN recommends the biopsy of all NMSCs before any procedure, allowing the most appropriate treatment choice.11 Despite the low mortality rate, this type of tumor has high morbidity because it causes disfigurement, resulting in physical and psychological disability.12 However, in some cases, there is tumor recurrence after excision. Among the reasons for occurrence, some studies highlight the relationship with the location, lesion extension, compromised surgical margins, and others. Considering this, it is of paramount importance to screen patients who have already had skin tumors to monitor the recurrence or persistence of tumors and detect new lesions.14
Assuming that there is considerable underreporting due to underdiagnosis, and also because it is a neoplasm with good prognosis if treated in an appropriate and timely manner, this study aims to verify the prevalence of anatomopathological results and epidemiological/clinical profile of patients who underwent biopsy for NMSC suspicious lesions in the Dermatology Service of Complexo Hospitalar Padre Bento de Guarulhos-SP (CHPBG), between June and December 2019, promoting further discussion and analysis on this subject.
We conducted a cross-sectional and retrospective observational study by analyzing medical records of patients who underwent skin biopsies for NMSC suspicion lesions in the Dermatology Service of CHPBG, from June to December 2019. This study was submitted to the CHPBG Research Ethics Committee (CEP 245/2025) through Plataforma Brasil and it was approved under the number 3,929,819.
The variables analyzed in the study were: age, gender, personal history of skin cancer, number of biopsies, biopsy site, and anatomopathological results. After completing data collection, the general epidemiological profile of the sample was designed (total number of patients in the study) by observing the mean, maximum, and minimum age and gender, in addition to following the frequency of the personal history of skin cancer.
Then, the patients were grouped according to the anatomopathological result, forming three distinct groups: Group 1, comprising patients with confirmed neoplastic lesions in the anatomopathological analysis; Group 2, including individuals with premalignant lesions in the anatomopathological analysis; and Group 3, with patients with benign lesions in the anatomopathological examination. The epidemiological profile of each group was analyzed later. We subdivided Group 1 into BCC, SCC, and other neoplasms to enable the individual assessment of each histological type of neoplasm found, allowing the analysis of the topographic location in each of these subgroups.
The study included the medical records of patients with skin lesions suggestive of NMSC, whose biopsies already had a histopathological result. The biopsies were performed at the CHPBG Dermatology Service from June to December 2019. We excluded the medical records of patients with requests for biopsy of cutaneous lesions not suggestive of malignancy, in addition to patients with cutaneous lesions suggestive of malignancy that had already been surgically addressed, even those with an indication for a new biopsy. Likewise, patients who did not attend or did not have the anatomopathological report during the research period and individuals with a previous diagnosis of NMSC known as Gorlin Syndrome, xeroderma pigmentosum, or mycosis fungoid, or those treated outside the established period, were excluded.
This study included all skin biopsy samples indicated by clinical suspicion of NMSC, totaling 382 points of skin biopsies in a total of 287 patients, corresponding to a mean of 1.33 biopsies per patient, with a maximum number of seven biopsies in the same patient.
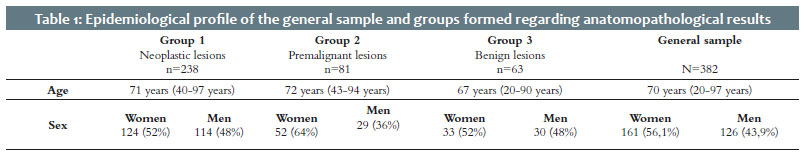
The overall sample (287 patients) comprised 126 (43.9%) men and 161 (56.1%) women, and the patients’ age ranged between 20 and 97 years, with a median of 71 years. Among the assessed patients, 129 (44.95%) had a personal history of skin cancer and 158 (55.05%) did not.
We formed three large groups according to the anatomopathological results obtained from the samples to know the diagnoses of suspicious lesions in the general sample:
- Group 1: comprising samples with anatomopathological results that confirmed neoplastic lesions;
- Group 2: including samples with anatomopathological results of premalignant lesions;
- Group 3: encompassing samples with anatomopathological results of benign lesions.
Group 1 comprised 62% (238 cases) of the general sample, most of them (52%) women. This group had a median age of 71 years, with a minimum age of 40 years and a maximum of 97 years. Group 2 corresponded to 21% (81 cases, 64% women and 36% men) and Group 3 to 17% (63 cases, 52% women and 48% men) of the total sample. The median age was 72 years, with a minimum age of 43 years and a maximum of 94 years, and 67 years, with a minimum age of 20 years and a maximum of 90 years, for Groups 2 and 3, respectively (Table 1).
Regarding the personal history of skin cancer, we found it in 45% (n=107) of positive biopsies for skin cancer (238 samples). For the group of positive biopsies for premalignant lesions (81 samples), 54% (n=44) already had a previous skin cancer diagnosis. In the group of positive biopsies for benign lesions (63 samples), 37% (n=23) had a previous history of skin cancer (Table 2).
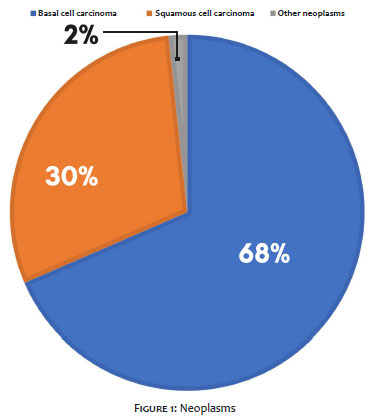
After this initial classification into three large groups, we subdivided the samples from Group 1 according to the histological type of skin cancer. We found 163 cases of BCC (68%), 71 cases of SCC (30%), and 4 cases of other neoplasms (2%). In the latter, the neoplasms found were melanoma (1), undifferentiated carcinoma (1), epithelioid neoplasm (1), and adenocarcinoma (1) (Figure 1).
The anatomopathological results compatible with the diagnosis of actinic keratoses (81 samples) justified the formation of Group 2 since they comprise the spectrum of premalignant skin lesions not classified as neoplastic or benign.
Regarding Group 3, most benign lesions found were nonspecific inflammatory process (15), followed by seborrheic keratosis (11), and intradermal and compound melanocytic nevus (9), in addition to the viral wart (7), among others with lower frequency.
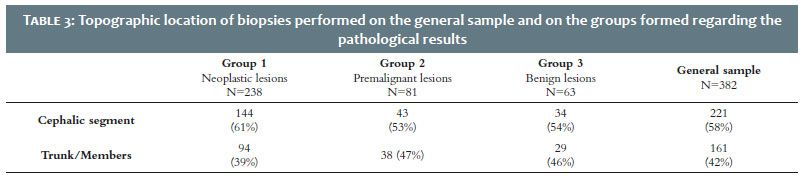
We also assessed the frequencies of the topographic locations of the biopsies performed. The cephalic segment was prevalent with 221 samples (58%), followed by 161 samples (42%) in the trunk and limbs. Regarding the topographic location of biopsied lesions, in the individual analysis of each group, we noticed that Group 1 presented 61% of the samples in the cephalic segment, as well as Group 2 (53%) and Group 3 (54%) (Table 3).
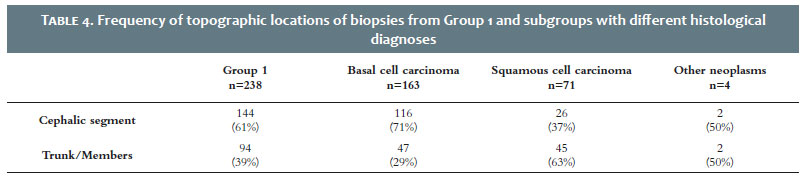
Concerning the topographic locations of the neoplastic lesions (Group 1), in the different histological types, we observed that most of the biopsies for BCC (71%) were in the cephalic segment. On the other hand, SCC was more biopsied in the trunk and limbs (63%) (Table 4).
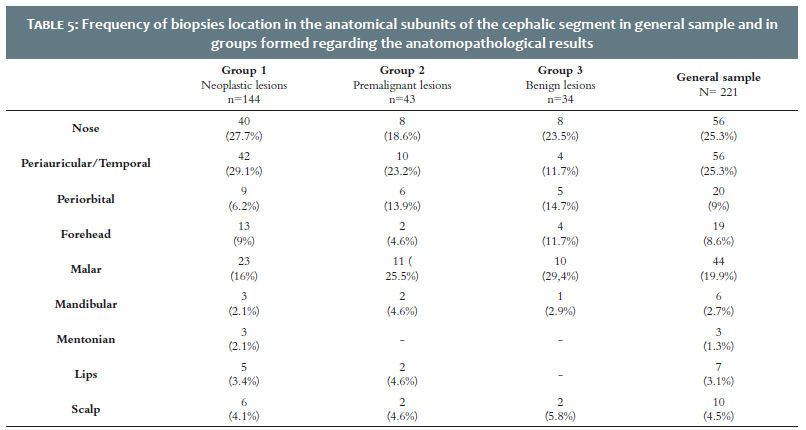
Finally, due to the prognostic importance that the cephalic segment’s risk zones (zone H and zone M) can pose, this region was subdivided into nose, periauricular/temporal, periorbital, forehead, cheeks, jaw, chin, lips, and scalp. Thus, it was possible to identify the frequencies of biopsies in each of these anatomical subunits.
This study showed that the prevalent anatomical subunits of the cephalic segment in Group 1 were the periauricular/temporal (42% - 29.1%) and nose (40% - 27.7%). Regarding Group 2, the most frequent anatomical subunits of the cephalic segment were cheek (25.5%), periauricular/temporal (23.2%), nose (18.6%), and periorbital (13, 9%). There were no biopsies in the chin region resulting in pre-malignant lesions. In Group 3, the cheek (29.4%), nose (23.5%), and periorbital (14.7%) areas were the most biopsied anatomical subunits. It is noteworthy that there were no biopsies in the chin and lips regions representing benign lesions (Table 5).
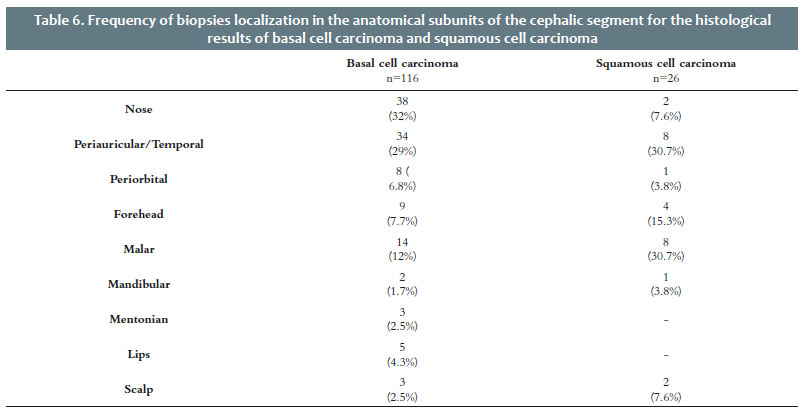
When we assessed only the frequency of biopsies location in the anatomical subunits of the cephalic segment that obtained BCC results, we observed that the most frequent were the nose (32%) and periauricular/temporal regions (29%). Likewise, regarding SCC in the cephalic segment, when we analyzed this frequency, we noticed that the most frequent locations were the periauricular/temporal and cheek areas, both with the same incidence (30.7%) followed by the frontal region (4%-15.3%). It should be noted that, in the entire sample, the jaw and lips regions did not present reports compatible with SCC (Table 6).
This study evaluated the anatomopathological results of all skin lesions indicated for biopsy due to suspicious malignancy over seven months (June to December 2019) in the Dermatology Service of the CHPBG. We obtained 382 biopsies from a total of 271 patients, of which 62% had a diagnosis of skin cancer, 21% indicated premalignant lesions, and only 17% excluded neoplasia. A study conducted in a Reference Service in Southern Brazil found a similarity in the order of frequency of diagnoses. It evaluated 531 anatomopathological results of skin cancer and actinic keratoses, in which 39.74% were BCC, 18.27% were SCC, 4.89% were melanoma, and 31.1% were actinic keratosis.15
According to the data from this study, the mean age of the general sample of patients with suspected skin cancer was 70 years and, for the group with confirmed skin cancer, it was 71 years – similar to those found in other studies. It indicates a higher prevalence of skin cancer in patients over 40 years of age due to greater sun exposure throughout life, the most important risk factor.1,8,9,16,17
In Brazil, approximately 176,930 new cases of skin cancer were estimated in 2020. The state of São Paulo estimated an incidence rate of non-melanoma skin cancer in 2020 higher for women (101.84 per 100,000 women) and lower for men (72.31 per 100,000 men).1 According to this study’s findings, the prevalence was also increased for women, as they had more indication for biopsy (56.1%). The increased prevalence among women was also verified when we evaluated only patients with confirmed skin cancer (52% were women).
The patient with skin cancer becomes a matter of concern due to the risk of developing other skin cancers such as BCC, SCC, and melanoma. Evidence from cohort studies and case registries shows that the patient with skin cancer has a relative risk of 1.12-1.49 times higher for developing a new skin tumor.18 Thus, it is worth noting that, in our study, 45% of patients with skin cancer confirmed by the anatomopathological examination (Group 1) had a second diagnosis of skin cancer in their lifetime.
Among the neoplasms confirmed by the anatomopathological examination, BCC presented the highest prevalence, with 68% of the total diagnosed neoplasms. This percentage agrees with the literature data that shows that this histological type is the most frequent, with rates reaching up to 70% of all skin neoplasms.8,16,17 According to the order of prevalence of neoplasms, we also emphasize that SCC ranked second, representing 30% of diagnoses. These values are very close to those of the 2015 European Consensus, where SCC represents approximately 20% of skin neoplasms.18
The anatomopathological results compatible with the diagnosis of actinic keratoses represented 21% of the total cases in our study. These lesions comprise a classic spectrum of premalignant cutaneous lesions not categorized as malignant or benign. However, some authors classify them as “in situ” neoplasms since they derive from clonal modifications of keratinocyte DNA.9 Although the diagnosis of actinic keratosis is clinical, some criteria may justify the need for biopsy due to the possibility of neoplastic transformation, such as lesions larger than 1 cm, bleeding, ulceration, induration, rapid growth, and intense erythema.9
NMSC is typically found in the cephalic and cervical segment, upper trunk, and arms.8,9,18,19 In our study, more than half (58%) of the biopsies were performed in the cephalic segment, in accordance with what was found in another Reference Hospital, where the authors showed that most biopsies were performed in the cephalic segment (50.47% of cases).20
A study that epidemiologically assessed patients who obtained skin biopsies compatible with BCC observed that 67% of them were identified in the cephalic segment. The three prevalent anatomical subunits were the nose (47.4%), ear (16.3%), and forehead (14.9%).18 Our study showed that, for patients diagnosed with BCC, the three anatomical subunits most frequently biopsied were the nose (32%), periauricular/temporal region (29%), as reported in the study mentioned above, and the cheek(12%), differing from the previous research.
Most conclusive SCC biopsies occurred in the trunk and limbs (63%), and face (37%). It differs from the literature, which indicates a higher frequency of these tumors also in the cephalic segment. According to the European Consensus (2015), 90% of SCCs are in photoexposed areas, such as the head, neck, back of the hands, and forearms.19 An epidemiological assessment conducted in 2012 identified that 25.9% of SCC biopsies were performed in trunk and limbs and 32.6% on the face, but 41.5% of the reports did not disclose this information.12
According to a literature review about actinic keratoses, these lesions are predominantly located in sun-exposed areas, such as the face, scalp (mainly of bald heads), cervical region, shoulders, forearms, and back of the hands.9 Although the diagnosis of actinic keratosis is clinical, some criteria may justify the need for biopsy due to the possibility of neoplastic transformation, such as lesions larger than 1 cm, bleeding, ulceration, induration, rapid growth, and intense erythema.9 In our study, the biopsied lesions were mainly distributed in the cephalic segment, representing 53% of the sample, and the malar subunit was the most biopsied. Also, 47% of the biopsies were performed in the trunk and limbs. Another relevant factor concerns the potential for malignant actinic keratosis. Though it presents a relatively low percentage (about 10% in immunocompetent patients and 20% in immunocompromised patients, considering only one lesion in 10 years), patients with this type of lesion have a history of intense and prolonged sun exposure. Thus, they almost always have a diagnosis of more than one lesion – which increases the chance of having some malignant transformation.9
When we face a possible clinical diagnosis, together, a range of possible differential diagnoses opens up. With non-melanoma skin cancer it is no different. Thus, other neoplastic diseases of varying cell lineages, such as melanocytes, spindle cells, muscle fibers, gland cells, and non-neoplastic lesions of different inflammatory and even infectious origins, are part of these diagnostic options.21 It justifies the finding of other neoplasms (melanoma, undifferentiated carcinoma, epithelioid neoplasm, and adenocarcinoma) and the different benign lesions as anatomopathological results of some patients in our study.
Due to the epidemiological importance of NMSC and its growing incidence in the world population, its consideration as a public health problem is imperative. In this study, we evidenced a higher incidence of skin cancer among women and elderly patients, and the most frequent diagnosis was basal cell carcinoma. Therefore, better understanding the epidemiological profile of skin cancer in patients treated at a Reference Hospital and knowledge of the accuracy of the biopsies performed allowed a better assessment of the prevalence and possible risk factors associated with this type of neoplasm in this sample of the population. Thus, we emphasize the need for conducting more studies to establish better prevention strategies, with emphasis on early diagnosis and treatment.
Thessaly Puel de Oliveira 0000-0002-8269-4266
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Hillani da Silva Andrade 0000-0001-7466-1731
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
José Roberto Pegas 0000-0002-2541-6008
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Cristina Santos Ribeiro Bechara 0000-0002-7723-2980
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Instituto Nacional do Câncer (INCA). [Cited 2019 Jun 13]. Available from: http://www.inca.gov.br
2. Graffunder CM, Wyatt SW, Bewerse B, Hall I, Reilley B, Lee-Pethel R. Skin cancer prevention: the problem, responses, and lessons learned. Health Educ Behav. 1999;26(3):308-16.
3. Geller AC, Cantor M, Miller DR, et al. The environmental protection agency's national sun wise school program: sun protection education in US school (1999-2000). J Am Acad Dermatol. 2002;6(5):683-9.
4. Miller SJ. Biology of basal cell carcinoma (Part I). J Am Acad Dermatol. 1991;24(1):1-13.
5. Imanichi D, Gasparello Filho JL, Moraes CF, Soterol RC, Gomes LO. Fatores de risco do câncer de pele não melanoma em idosos no Brasil. Diagn Tratamento. 2017;22(1):3-7.
6. Acosta AE. Carcinoma basocelular. En: Guias de práctica clínica en enfermedades neoplásicas. Instituto Nacional de Cancerologia. 2001;15-31.
7. Costa CS. Epidemiologia do câncer de pele no Brasil e evidências sobre a sua prevenção. Diagn Tratamento. 2012;17(4):206-8.
8. Bichakjian CK, Olencki T, Aasi SZ, Alam M, Andersen JS, Berg D, et al. Basal cell skin cancer, version 1.2016, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2016;14(5):574-97.
9. Reinehr CPH, Bakos RM. Ceratoses actínicas: revisão dos aspectos clínicos, dermatoscópicos e terapêuticos. An Bras Dermatol. 2019;94(6):637-57.
10. Stratigos A, Garbe C, Lebbe C, Malvehy J, del Marmol V, Pehamberger H, et al. Diagnosis and treatment of invasive squamous cell carcinoma of the skin: European consensus-based interdisciplinary guideline. Eur J Cancer. 2015;51(14):1989-2007.
11. Zink BS. Câncer de pele: a importância do seu diagnóstico, tratamento e prevenção. Revista HUPE. 2014;13(supl.1):76-83.
12. Corrêa LHL, Popoaski CP, Custódio G, Gonçalves CO, Trevisol FS. Epidemiologia dos carcinomas espinocelulares na população atendida em Tubarão (SC), entre 1999 e 2009. An Bras Dermatol. 2012;87(4):572-7.
13. Karagas MR. Occurrence of cutaneous basal cell and aquamous cell malignancies among those with a prior history of skin cancer. The Skin Cancer Prevention Study Group. J Invest Dermatol. 1994;102(6):10S13S.
14. Beralla CS, Blanco LFO, Yamane A. Análise dos dados epidemiológicos dos laudos de carcinoma espinocelular. Rev Bras Clin Med São Paulo. 2013;11(1):43-7.
15. Dergham AP, Muraro CC, Ramos EA, Mesquita LAF, Collaço LM. Distribuição dos diagnósticos de lesões pré-neoplásicas e neoplásicas de pele no Hospital Universitário Evangélico de Curitiba. An Bras Dermatol. 2004;79(5):555-9.
16. Custódio G, Locks LH, Coan MF, Gonçalves CO, Trevisol DJ, Trevisol FS. Epidemiologia dos carcinomas basocelulares em Tubarão, Santa Catarina (SC), Brasil, entre 1999 e 2008. An Bras Dermatol. 2010;85(6):815-26.
17. Nasser N. Epidemiologia dos cânceres espinocelulares - Blumenau (SC) - Brasil, de 1980 a 1999. An Bras Dermatol. 2004;79(6):669-677.
18. 18 - Work Group, Invited Reviewers, Kim JYS, Kozlow JH, Mittal B, Moyer J, Olenecki T, Rodgers P. Guidelines of care for the management of cutaneous squamous cell carcinoma. J Am Acad Dermatol. 2018;78(3):560-78.
19. Peris K, Fargnoli MC, Garbe C, Kaufmann R, Bastholt L, Seguin NB, et al. Diagnosis and treatment of basal cell carcinoma: European consensus-based interdisciplinary guidelines. Eur J Cancer. 2019;118:10-34.
20. Simões JC, Campos ECR, Kamei DJ, et al. Análise do perfil epidemiológico, clínico e patológico de pacientes portadores de câncer de pele não melanoma no hospital evangélico de Curitiba. Rev Med Res. 2011;13(4):251-60.
21. Chinem VP, Miot HA. Epidemiologia do carcinoma basocelular. An Bras Dermatol. 2011;86(2):292-305.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}