


Isabella Parente Almeida1; Maria Isabel Ramos Saraiva1,2; Maria Cristina de Lorenzo Messina2,3; João Pereira Duprat4; Luiz Guilherme Martins Castro1,2
Financial support: None
Conflict of interest: None
How to cite this article: Saraiva MIR, Almeida IP, Messina MCL, Duprat JP, Castro LGM. Sentinel Lymph Node Biopsy for Cutaneous Melanoma in a real life setting: analysis of 47 cases treated at a private clinic in Brazil. Surg Cosm Dermatol. 2021;13:e20210021
BACKGROUND: Sentinel Lymph Node (SLN) status has been shown to be the strongest independent prognostic factor of cutaneous melanoma (CM) stage I-II patients. Few papers on CM at private clinics (PC) are available.
OBJECTIVE: To present clinical and histologic data, complications and frequency of SLN involvement in CM patients diagnosed and followed at a dermatology/cutaneous oncology PC in São Paulo/Brazil, who were submitted to SLNB.
METHODS: Retrospective, single-center cohort of patients who attended PC from June 1998 to Jan 2020. Electronic files were selected and analyzed. Minimum period for considering the patient eligible was 1 year.
RESULTS: 215 CM lesions were identified in 184 patients(1.2 melanoma/patient). Forty-seven patients (25.5%) were submitted to SLNB and 59 SLN for histologic examination (1.2 SLN/patient). 10,9% tested positive. SLN identification happened in 95.7%. In 38/47 (80,8%) patients single LBD was found, while multiple-LBD was found in 9/47(19.1%). Eighteen(72,0%) out of 25 trunk lesions drained to single basin, while in 7 patients multiple LBD was found. Complication rate was 6,0%.
CONCLUSION: Percentage of CM patients that undergo SLNB, node positivity for metastasis, draining basins and complications in this study were similar to studies in northern hemisphere patients. Clinical and epidemiologic characteristics of CM patients differ markedly between PC and PHS patients.
Keywords: Biopsy; Melanoma; Sentinel lymph node
Sentinel Lymph Node (SLN) status is the most decisive independent prognostic factor of cutaneous melanoma (CM) stage I-II patients.1 Accurate assessment of the regional LN status by SLN biopsy (SLNB) is becoming even more critical in the era of novel effective adjuvant therapies for the microscopic nodal disease.2 Some points on SLNB’s role and benefit in this setting are still controversial.3
Most published papers on SLNB for CM analyze patients from the northern hemisphere and Australia, large hospitals, or public health system (PHS). Very few articles on CM patients diagnosed and followed at private clinics (PC) are available in the literature. 4-8 We have not been able to find papers specifically addressing CM patients from PC who underwent SLNB, which leaves information gaps about what happens in this context.
This study aims to present clinical and histologic data, describing complications and frequency of SLN involvement in CM patients diagnosed and followed at a dermatology/cutaneous oncology PC in São Paulo/Brazil. They were submitted to SLNB, and their data were compared with data from the literature.
A retrospective, single-center study selected and analyzed the electronic files of a cohort of patients diagnosed with CM attending a PC from June 1998 to January 2020. Data collected consisted of gender, primary tumor’s anatomic location, melanoma clinical type, Breslow thickness, and history of SLNB. Among those submitted to SLNB, we also assessed SLN status, lymph node basins drainage, number of excised SLN, surgical complications associated with SLNB, and eventual local or distant relapses.
The same surgical team, consisting of dermatologic and oncologic surgeons, operated on all but seven patients at different hospitals in São Paulo. Pathologists from the different hospitals where surgeries were performed determined SLN histologic status. After removal, SLN were submitted to serial sectioning and permanent preparations for histological and immunohistochemical examination, according to current recommendations at the time. SLN was identified using Tc-labeled radiopharmaceutical preoperative lymphoscintigraphy and subsequent intraoperative detection with gamma probe associated or not with blue-dye.
Follow-up was also based on information contained in the electronic charts. The minimum period for considering the patient eligible was one year.
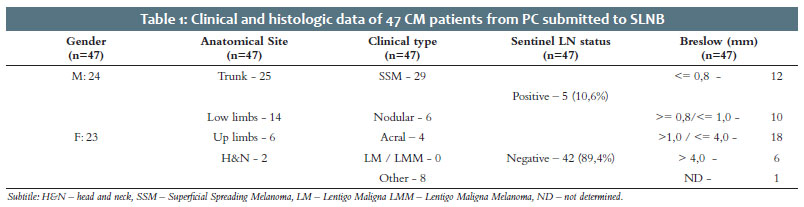
A total of 215 CM lesions were identified in 184 patients (1,2 melanoma/patient). Forty-seven patients (25,5%) were submitted to SLNB, which harvested 59 SLN for histologic examination (1,2 SLN/patient). In 2/47 (4,2%) patients no SLN was identified. Five/47 patients (10,6%) tested positive.
Primary lesions that led to the indication of SLNB were located on the trunk (26), lower limbs (14), upper limbs (6), and head & neck (2) (Table 1). Pre-operatory lymphoscintigraphy allowed identification of lymph node basins drainage (LBD) in all but one patient. In 38/47 (80,8%) patients single LBD was found while multiple-LBD was observed in 9/47 (19,1%).
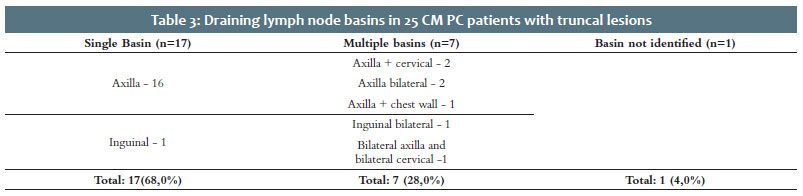
Eighteen (72,0%) out of 25 lesions drained to single basins, while in 7 patients these lesions drained to multiple basins. Among them, there was a case where CM was located in the interscapular (midline) region and drained to 4 distinct basins (bilateral axilla and bilateral cervical) (Table 3).
Regarding surgical details, SLN identification happened in 95,7% (45/47) of cases. We observed complications four times (3 cases): one patient developed lower limb lymphorrhea and deep venous thrombosis, while two developed lymphorrhea. The complication rate was 6,0% (Table 2).
Thirty-nine patients were eligible for follow-up (at least 12 months). The follow-up period varied from 13 to 177 months. Total follow-up period for the 39 patients was 2410 months, with an average of 61,8 months. False-negatives were identified in 2 cases: 4,0% (per-protocol – PP: 2/47) or 5,1% (intention to treat – ITT: 2/39).
Eggermont1 stated almost two decades ago that SLNB had utterly changed the management of primary CM. Accurate assessment of the regional LN status by SLNB has become even more critical in the present era of novel effective adjuvant immuno and targeted therapies for the microscopic nodal disease.2
The present study performed the histologic processing of the SLNs harvested at different hospitals, by different pathologists, for over 20 years. In each case, samples were processed according to current international recommendations at the time. Technical details varied over the period. This lack of standardization in the SLN assessment could be understood as a negative point - which might be so if the objective was to conduct a controlled study. This non-standardized methodology used in the study for 22 years by different pathologists in various hospitals reflects the “real-life” situation, which was the paper’s objective.
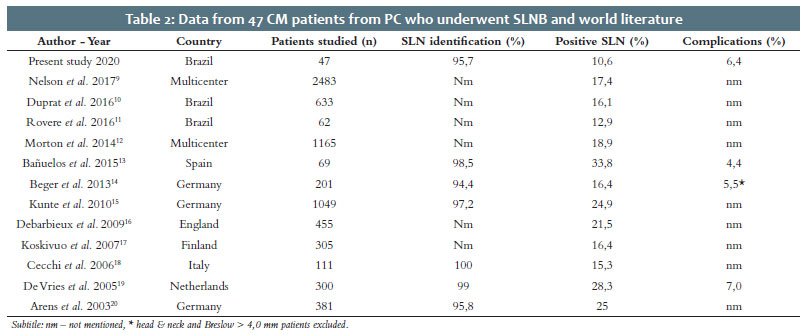
The percentage of identified and excised SLN among the 47 patients reached 95,7% with an averaged of 1,2 SLN/patient, a number in concordance with international literature (Table 2).
The number of papers reporting on CM patients followed at PC is extremely small.5-8,19 As early as 1997, Castro et al.8 demonstrated that in Brazil, the proportion of Caucasians in dermatology PC and Public Health System (PHS) patients differs markedly. Other Brazilian authors corroborated this finding. It it is probably justified by historical aspects and the immense racial diversity in the country, where miscegenation makes its population unique, including Caucasians, Africans, Asians, and indigenous Brazilians. 21,22 Thin CM (Breslow ≤1,0 mm) is diagnosed in a much higher proportion among PC population.8,19,21 CM patients studied in the present study tend to have characteristics that resemble northern hemisphere CM patients. In contrast, there is a higher proportion of non-Caucasian patients with acrally located, thick and ulcerated lesions among PHS population. Similar findings are also observed in Chile and Mexico. 5,23
Murali et al.24 found 6.7% positivity for metastatic melanoma cells in SLN when analyzing 432 patients with thin (≤1 mm) CM. Although there is a low but significant rate of SLN positivity in patients with primary CM of 0.51 to 1.0 mm in thickness, no SLN positivity was detected in the present study´s patients with primary tumor thickness of ≤0,48 mm.
The high number of Breslow <0,8 mm patients submitted to SLNB (12/47 – 25,5%) deserves comment: criteria indicative of SLNB varied during the study period. The presence of mitosis and regression would be decisive to indicate SLNB at some point in time and nowadays is no longer so.25 In the present study, different reasons justified SLNB for Breslow <0,8mm patients: regression was identified in 5 cases, 1 acral lesion, 1 lesion with satelitosis, 2 of mitotic rate >1, one incomplete shave biopsy, where Breslow thickness was determined as “at least”, 2 cases where patients demanded to have the surgery for their own will.
Skip metastases are one of the most significant drawbacks of the method and can be found at different rates. The present study identified two cases. The first was a truncal CM with Breslow thickness 4,5mm and Clark level IV draining to the left axilla. The SLN tested negative for metastases. Ten years later pulmonary and intestinal metastases were identified and quickly led the patient to death. The second was also a truncal CM with Breslow thickness 5,85 mm and vascular invasion draining to both inguinal basins. The three SLN tested negative for metastases. Two years later, cerebral metastases were identified.
Preoperative lymphoscintigraphy has proved to be a vital planning instrument to guide complete removal of all SLNs, mainly when the primary lesion is located on the trunk, as found in the present paper, where 7 out of 25 (28,0%) patients had more than one drainage basin identified (Table 3). Truncal CM presents multiple-LBD from 17% to 34,6% of cases, especially when the lesion is mid-line. The present study associated double axillary/cervical and bilateral axillary drainage with upper back lesions.
The significance of multiple-LBD in truncal melanoma patients undergoing SLNB has long been debated. Currently, it it is widely accepted that multiple-LBD is not an independent risk factor for SLN metastasis and has no independent prognostic significance. Among matched pairs, multiple-LBD did not affect rates of LN metastasis overall survival, overall recurrence, locoregional recurrence, or distant recurrence.26-28
SLNB is an invasive procedure and is not free of risks. Complications and sequelae are far less common when compared to complete LN dissection. Wrightson et al. reported on a total of 2120 patients submitted to SLNB. Overall, 96 (4.6%) of them developed major or minor complications. In contrast, 103 (23.2%) of 444 patients experienced complications when SLNB was followed by complete LN dissection, a number five times higher. 29
CM complication rates reported after SLNB are highly variable in the literature, ranging between 1.8% and 29.9%.30-32 In a systematic literature review, Moody et al.25 found an overall complication rate of 11.3% among SLNB patients, most temporary. Incidence of infection was 2.9%; seroma, 5.1%; hematoma, 0.5%; lymphedema, 1.3%; and nerve injury, 0.3%.
The frequency of complications observed in the present study (6,0%) fits the interval described in Moody et al. review paper.25 One patient developed lower limb lymphorrhea and deep venous thrombosis, while two developed lymphorrhea.
Despite the relatively small number of patients studied, we could observe that data obtained from CM patients at PC submitted to SLNB closely resembled those described in northern hemisphere patients regarding the percentage of individuals that undergo SLNB, node positivity for metastasis, age, draining basins, and complications.
Clinical and epidemiologic characteristics of CM patients in Brazil differ markedly between PC and PHS population. The present study’s findings are restricted to CM Brazilian patients from PC and should not be extrapolated to Brazilian patients from the PHS.
Isabella Parente Almeida 0000-0002-6283-4065
Statistical analysis; study conception and planning; preparation and writing of the manuscript; data collection, analysis and interpretation; intellectual participation in propaedeutic and/or therapeutic management of studied cases; critical literature review.
Maria Isabel Ramos Saraiva 0000-0002-5043-489X
Statistical analysis; study conception and planning; preparation and writing of the manuscript; data collection; analysis and interpretation; intellectual participation in propaedeutic and/or therapeutic management of studied cases; critical literature review.
Maria Cristina de Lorenzo Messina 0000-0002-8401-7349
Data collection, analysis and interpretation; active participation in research orientation; critical literature review; manuscript critical review.
João Pereira Duprat 0000-0001-8968-4506
Data collection, analysis and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Luiz Guilherme Martins Castro 0000-0002-6269-1957
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Eggermont AM. Adjuvant therapy of malignant melanoma and the role of sentinel node mapping. Recent Results Cancer Res. 2000;157:178-89.
2. Ulmer A, Kofler L. Sentinel-node-Biopsie und Lymphknotendissektion im Zeitalter neuer Systemtherapien des malignen Melanoms [Sentinel node biopsy and lymph node dissection in the era of new systemic therapies for malignant melanoma]. Hautarzt. 2019;70(11):864-9.
3. Bigby M, Zagarella S, Sladden M, Popescu CM. Time to reconsider the role of sentinel lymph node biopsy in melanoma. J Am Acad Dermatol. 2019;80(4):1168-71.
4. Stricklin SM, Stoecker WV, Malters JM, Drugge R, Oliviero M, Rabinovitz HS, et al. Melanoma in situ in a private practice setting 2005 through 2009: location, lesion size, lack of concern. J Am Acad Dermatol. 2012;67(3):e105-9.
5. Zemelman VB, Valenzuela CY, Sazunic I, Araya I. Malignant melanoma in Chile: different site distribution between private and state patients. Biol Res. 2014;47(1):34.
6. Cherian P, Tait CP. Melanoma in private practice: do dermatologists make a difference? Australas J Dermatol. 2009;50(4):257-60.
7. Barton MB, Gabriel GS, Frommer MS, Holt PE, Thompson JF. Surgical procedures for melanoma in public and private New South Wales hospitals, 2001-2002. ANZ J Surg. 2006;76(5):318-24.
8. Castro LGM, Toyama CL, Gomes AP, Freire MA, Brito T. Câncer de pele em clínica particular em São Paulo. An Bras Dermatol. 1996;6:471-6.
9. Nelson DW, Stern S, Elashoff DE, Elashoff R, Thompson JF, Mozzillo N, et al. Impact of time between diagnosis and SLNB on outcomes in cutaneous melanoma. J Am Coll Surg. 2017;225(2):302-11.
10. Duprat JP, Brechtbülh ER, Costa de Sá B, Enokihara M, Fregnani JH, Landman G, et al. Absence of tumor-infiltrating lymphocyte is a reproducible predictive factor for sentinel lymph node metastasis: a multicenter database study by the brazilian melanoma group. PLoS One. 2016;11(2):e0148160.
11. Rovere RK, A Sde L, Demarchi V, Stein CE. Sentinel lymph node in melanoma - a study conducted in the South of Brazil. Klin Onkol. 2016;29(4):274-8.
12. Morton DL, Thompson JF, Cochran AJ, Mozzillo N, Nieweg OE, Roses DF, et al. Final trial report of sentinel-node biopsy versus nodal observation in melanoma. N Engl J Med. 2014;370(7):599-609.
13. Bañuelos-Andrío L, Rodríguez-Caravaca G, López-Estebaranz JL, Rueda-Orgaz JA, Pinedo-Moraleda F. Biopsia selectiva del ganglio centinela en melanoma: experiencia durante 8 años en un hospital universitario [Sentinel lymph node biopsy in melanoma: our experience over 8 years in a universitary hospital]. Cir Cir. 2015t;83(5):378-85.
14. Beger J, Hansel G, Krönert C, Fuchs M, Tanner C, Schönlebe J, et al. A 10-year analysis of primary cutaneous malignant melanoma with sentinel lymph node biopsy and long-term follow-up. Int J Dermatol. 2013;52(2):220-30.
15. Kunte C, Geimer T, Baumert J, Konz B, Volkenandt M, Flaig M, et al. Prognostic factors associated with sentinel lymph node positivity and effect of sentinel status on survival: an analysis of 1049 patients with cutaneous melanoma. Melanoma Res. 2010;20(4):330-7.
16. Debarbieux S, Duru G, Dalle S, Béatrix O, Balme B, Thomas L. Sentinel lymph node biopsy in melanoma: a micromorphometric study relating to prognosis and completion lymph node dissection. Br J Dermatol. 2007;157(1):58-67.
17. Koskivuo I, Talve L, Vihinen P, Mäki M, Vahlberg T, Suominen E. Sentinel lymph node biopsy in cutaneous melanoma: a case-control study. Ann Surg Oncol. 2007;14(12):3566-74.
18. Cecchi R, De Gaudio C, Buralli L, Innocenti S. Lymphatic mapping and sentinel lymph node biopsy in the management of primary cutaneous melanoma: report of a single-centre experience. Tumori. 2006;92(2):113-7.
19. de Vries M, Jager PL, Suurmeijer AJ, Plukker JT, van Ginkel RJ, Hoekstra HJ. Schildwachtklierbiopsie bij het melanoom: prognostische betekenis en nadelen bij 300 patiënten [Sentinel lymph node biopsy for melanoma: prognostic value and disadvantages in 300 patients]. Ned Tijdschr Geneeskd. 2005;149(33):1845-51.
20. Arens A, Osinga J, Schwipper V, Schober O, Tilkorn H, Liebau J. Sentinel-Lymphknoten-Dissektion beim malignen Melanom. Ein diagnostischer und therapeutischer Standard [Sentinel lymph node dissection in patients with malignant melanoma. Diagnostic and therapeutic standards]. Chirurg. 2003;74(7):665-70.
21. Maia M, Russo C, Ferrari N, Ribeiro MCSA, Santos ABO. Reflexões em relação à epidemiologia do melanoma cutâneo no Brasil / Reflections regarding the epidemiology of cutaneous melanoma in Brazil An Bras Dermatol. 202;77(2):163-70.
22. 22 - Pena SD, Di Pietro G, Fuchshuber-Moraes M, Genro JP, Hutz MH, Kehdy Fde S, et al. The genomic ancestry of individuals from different geographical regions of Brazil is more uniform than expected. PLoS One. 2011;6(2):e17063.
23. Saez-de-Ocariz M, Sosa-de-Martínez C, Duran-McKinster C, Orozco-Covarrubias L, Palacios-López C, Ruiz-Maldonado R. Cutaneous melanoma in private vs. public practices of Mexican dermatologists. Int J Dermatol. 2008;47(6):637-9.
24. Murali R, Haydu LE, Quinn MJ, Saw RP, Shannon K, Spillane AJ, et al. Sentinel lymph node biopsy in patients with thin primary cutaneous melanoma. Ann Surg. 2012;255(1):128-33.
25. Castro LG, Bakos RM, Duprat Neto JP, Bittencourt FV, Di Giacomo TH, Serpa SS, et al. Brazilian guidelines for diagnosis, treatment and follow-up of primary cutaneous melanoma - Part II. An Bras Dermatol. 2016;91(1):49-58.
26. Howard JH, Ozao-Choy JJ, Hiles JM, Sim MS, Faries MB. Prognostic value of multiple draining lymph node basins in melanoma: a matched-pair analysis based on the John Wayne Cancer Institute Experience. Front Oncol. 2017;7:172.
27. Ribero S, Osella Abate S, Pasquali S, Rossi CR, Borgognoni L, Piazzalunga D, et al. Multiple lymph node basin drainage in trunk melanoma is not associated with survival of sentinel lymph node-positive patients. Dermatology. 2017;233(2-3):205-11.
28. Castro LGM, Duprat JP, Landman G. Dupla drenagem para cadeias linfonodais distintas, detectada por técnica de biópsia de linfonodo sentinela em pacientes com melanoma cutâneo: relato de dois casos. An Bras Dermatol. 2005;80(5):499-502.
29. Thomas JM. Lymphoedema in the observation and biopsy arms of MSLT-1. Ann Surg Oncol. 2011;18(Suppl 3):S311.
30. Wrightson WR, Wong SL, Edwards MJ, Chao C, Reintgen DS, Ross MI, et al. Complications associated with sentinel lymph node biopsy for melanoma. Ann Surg Oncol. 2003;10(6):676-80.
31. Moody JA, Ali RF, Carbone AC, Singh S, Hardwicke JT. Complications of sentinel lymph node biopsy for melanoma - A systematic review of the literature. Eur J Surg Oncol. 2017;43(2):270-7.
32. Wollina U, Langner D, Schönlebe J, Tanner C, Fuchs M, Nowak A. Sentinel lymph node biopsy in early melanoma-comparison of two techniques for sentinel removal. Wien Med Wochenschr. 2017;167(5-6):100-3.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}