


Elcilane Gomes Silva1; Juliana Joyce Chaves de Lima2; Natalia Pantoja Costa1
Submitted on: 13/10/2020
Approved on: 04/03/2021
Financial support: None
Conflict of interest: None
How to cite this article: Silva EG, Lima JJC, Costa NP. Use of botulinum toxin in hidradenitis suppurativa. Surg Cosmet Dermatol. 2021;13:e20210013.
INTRODUCTION: Hidradenitis suppurativa (HS) is an inflamatory, chronic, recurrent, and debilitating condition. There is a lack of consensus about its treatment.
OBJECTIVE: We conducted a review of the national and international literature, searching for articles that addressed the use of botulinum toxin in HS, in addition to describing the doses and techniques used.
METHODS: A bibliographic search was performed in LILACS, Medline, and SciELO.
RESULTS: Botulinum toxin can be an effective therapy in patients with HS, especially in cases of concomitant hyperhidrosis and traditional therapies fail. It offers the possibility of conducting treatment with minimal adverse events, reproducible over time without loss of effectiveness, in addition to reducing pain.
CONCLUSIONS: Patients will likely need more than one treatment over time, as the lesions tend to recur after 6 to 10 months. The technique used has been the standard for hyperhidrosis. Further research is needed to understand its role in the management of HS, including the ideal dosage and frequency of administration.
Keywords: Hidradenitis suppurativa; Hidradenitis; Botulinum toxins; Botulinum toxins, type A
Hidradenitis suppurativa (HS) is also known as acne inversa or Verneuil’s disease. It is an inflammatory condition of a chronicle character, recurrent and debilitant. Its pathogenesis results from chronic obstruction of the follicular portions of the pilosebaceous units.1,2 Its prevalence ranges from 1% to 4% of the world’s population, but it is believed to be underestimated.²
The proposed pathogenic HS sequence starts with a follicular occlusion, causing dilation of the pilosebaceous unit, rupture, and exit of the follicular content (keratin, corneocytes, bacteria, sebaceous matter) in the dermis. The secondary inflammatory process involves deregulation in both innate and adaptive immunity.3,4 Extensive fibrosis is often seen as a late result of this inflammation. We still don’t know whether this mechanism comes from environmental and/or genetic factors.5 Among the risk factors, we can identify family history, obesity, smoking, and drug use (oral and injectable contraceptives containing medroxyprogesterone acetate or levonorgestrel).6
HS may occur sporadically, but genetic studies have identified susceptibility genes involved in the gamma-secretase expression. However, mutations were found only in a minority of HS patients.7 Currently, 23 pathogenic sequences are identified in HS. Still, these findings are probably significant only in the familial HS.8 Hessam et al. showed that the expression of IL36α, β, γ, and IL36Ra was significantly higher in HS lesional skin compared to healthy controls.9
The most common sites of HS involvement are intertriginous skin areas, including armpits, groins, perianal, perineal, and inframammary regions.10 The symptoms begin after puberty and at age 40, being more common in women, with a proportion of 3,6:1 reported in a retrospective French observational study.6,11 Lesions start as inflamed nodules and may evolve into fistulized and interconnected abscesses, forming scars, with pain as their main characteristic.12
It is noteworthy that the pain, associated with foul odor due to the secretion and scar formation, significantly impacts the patients’ quality of life. Even though it is a prevalent disease with limited therapeutic options, it is necessary to correctly treat HS patients due to the higher presence of depression and sexual dysfunction among them.13 Thus, due to its chronic character and its impact on the patients’ quality of life, its correct management, although complex, is essential.14
The initial approach of these patients depends on their classification using Hurley’s clinical staging:15 stage I - abscess(es) formation, no fistulization, and no scarring; stage II - recurrent abscesses, with sinus tracts formation and scarring; stage III - diffuse abscesses or interconnected sinus tracts and multiple abscesses.
In all patients, conservative management with weight loss and smoking cessation is recommended, and psychosocial support and analgesia if necessary. Antibiotics are effective in mild to moderate cases. In women, antiandrogenic therapy reduces the severity of the disease in some cases. Systemic immunosuppression, including cyclosporine and infliximab, led to a significant improvement in moderate to severe disease. In advanced disease, or where medical therapy has failed, surgical treatment may involve radical excision of affected apocrine glands. LASER (light amplification by stimulated emission of radiation) therapy and external beam radiation have also demonstrated efficacy and may be helpful in selected patients.16
Recently, the multiple uses of botulinum toxin (BT) in dermatological conditions have been reviewed, especially those called “Fold (intertriginous) dermatoses”.17 Among these is HS, which involves precisely these areas of the body.5
The exact mechanism by which BT affects the disease process in HS is unclear. The moist environment resulting from the sweat retained in the armpit and groin provides ideal conditions for bacteria to flourish. The presence of apocrine glandular secretions can aggravate it, forming a rich substrate for bacterial growth. The antiperspirant effect of BT reduces the skin flora population, consequently decreasing the inflammatory stimulus for HS. A second possibility is that BT shuts down the function of the whole pilosebaceous unit and apocrine secretion, preventing the rupture and dissemination of follicular material through the dermis, which usually results in more inflammation.18
Currently, there is a lack of consensus on the ideal treatment for HS. Despite the advent of biological drugs, the disease remains a therapeutic challenge. Many therapies are available, but the benefits of these treatments should be weighed against the adverse events. BT represents a new and promising treatment option for this complex disease. However, a shared treatment regimen is necessary to define the potential of this treatment in HS, and mainly, a change in the quality of life of these patients. Given this context, it is relevant to conduct studies seeking to relate such information and subsidize new and more efficient approaches. The present study aimed at reviewing the use of botulinum toxin in hidradenitis suppurativa in the national and international literature, besides describing the doses and techniques used to treat the disease.
This study is a narrative literature review. We conducted a bibliographic search on the electronic databases Latin American & Caribbean Health Sciences Literature (LILACS), Medical Literature Analysis and Retrieval System Online (Medline), and Scientific Electronic Library Online (SciELO), published from 2009 to 2019.
The descriptors used were: Hidradenitis Suppurativa, Hidradenitis, Botulinum Toxins and Botulinum Toxins, Type A. All descriptors are found in the Health Sciences Descriptors (DeCS). We identified nine articles in the databases mentioned above and selected six of them for this study after reading their title and abstract.
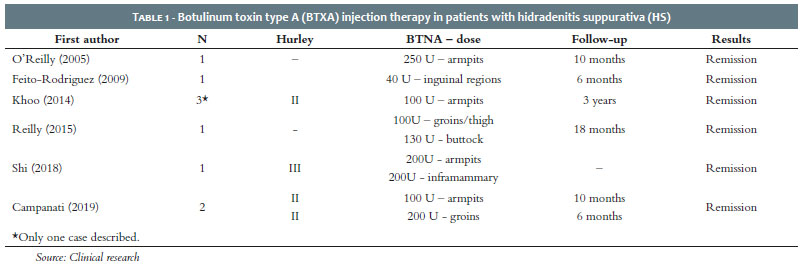
The first case of HS treated with botulinum toxin type A (BTXA) dates back to 2005. The 38-year-old patient (patient A) had the disease for more than ten years and was submitted to therapy with lymecycline and flucloxacillin without clinical improvement. She received then 250 U of Dysport® in both armpits. The toxin was delivered with intradermal papules, the standard technique for hyperhidrosis. After 15 days of the administration, there was no evidence of active inflammation. The patient had complete remission of symptoms until approximately ten months later when the first symptoms of mild inflammation reappeared.19
Feito-Rodriguez et al. described the first case of application of botulinum toxin A in a prepubertal child to treat HS (patient B). At six years of age, the child was diagnosed with HS, presenting erythematous papules and painful nodules only in the groin, symmetrically. Topical and oral antibacterials were prescribed, in addition to isotretinoin, which was discontinued due to adverse events. At the age of 7 years and 5 months, a total dose of 40 U of Botox® was applied under sedation, distributed in 10 to 12 points on an elliptical area on each side of the groin. She had complete remission until six months later when the first lesions reappeared. A new, similar application was made with a good therapeutic response.20
Khoo & Burova reported the third case in the literature, using BTXA to treat HS in three patients. The authors reported the most successful case in a 46-year-old patient (patient C) who had the disease for 11 years (Hurley II). She had already been submitted to systemic antibiotics, without improvement, and surgical drainage of the abscesses. The patient received 50 U of BTXA in each armpit. There was a good clinical response within three months after the first treatment, and after the second treatment, there was clinical remission, which lasted for more than a year. The other two patients presented a disease-free period from 5 to 6 months.18
Reilly et al. described another case of success in a 23-year-old woman (patient D), diagnosed with HS for four years. She had performed eight surgical incisions in the groins, buttocks, and inner part of the thighs, with slight improvement. The patient received 100 U of BTXA (Botox®) in the groin and inner thighs and 130 U in the buttocks. There was a complete resolution of the symptoms for three months. In the following 18 months, the patient received five more BTXA applications, each consisting of 200 U (100 U in the anterior region and 100 in the posterior). There was a four-month interval between treatments, and in the last month of this interval, there was an exacerbation of the lesions, requiring surgical intervention.16
Shi et al. also reported a case of successful treatment of HS in stage III with BTXA. The 40-year-old patient (patient E) presented HS in the groin and armpits with chronic pain and had failed therapy with oral and topical antibiotics and surgical treatment. She then received a total of 400 U of BTXA – 100 U for each site (bilateral and inframammary axillary region). The study used intradermal injection in parallel lines with 1 cm of distance between the points, with approximately 20 injections per area. There was an excellent response with a significant reduction in drainage and inflammation, as well as pain relief of 50%. In subsequent administration, the dose was reduced to 50 U per area, in addition to injection at other areas such as groins and perineal regions. However, the symptoms returned earlier with the dose reduction. Thus, the subsequent applications resumed the dose of 100 U for each site. The patient received no other treatment during BTXA therapy.10
In 2019, Campanati et al. described two cases of HS treated with BTXA. Case 1 was a 23-year-old young woman (patient F) who presented HS in the armpits (Hurley II) refractory to topical and oral therapies. The area was treated with BTXA (Vistabex®), with a technique similar to axillary hyperhidrosis’ procedure, using 50 U per armpit diluted in 2.5 ml of 0.9% saline solution. She received an intradermal injection, with the administration of 4 U in each square of 1.5 cm². Case 2 was a 50-year-old man (patient G) with HS in the groin and inner thigh region (Hurley II) who had failed other topical and systemic therapies. He received BTXA (Botox®) in the same dilution and technique described above, but 100 U on each side. Both patients were reassessed after one, three, and six months. They experienced real improvement with the disappearance of inflammatory lesions in case 1 and reduction of fistulas in the groin in case 2. The patient of case 1 decided to undergo therapy again after ten months with an optimal response5 (Table 1).
Botulinum toxin type A can be an effective therapy in patients with HS, especially if there is concomitant hyperhidrosis and when traditional therapies fail.
The BTXA blocks the release of acetylcholine and other pre-synaptic vesicle neurotransmitters by deactivating SNARE proteins. It has been used for hyperhidrosis blocking the cholinergic nerve fibers of the sweat glands. The US Food and Drug Administration (FDA) approved it in 2004 to treat severe primary axillary hyperhidrosis refractory to the use of antiperspirants.10
It is not clear how BTXA can improve HS. The first hypothesis is that local factors such as humidity can create an ideal environment for bacterial growth, a known pro-inflammatory element. In fact, bacteria are not promoters of the disease, but they among the main contributors to a vicious inflammatory circle.21 Thus, reducing sweat production could reduce the skin flora population and its potential pro-inflammatory effect.
The other hypothesis about the BTXA therapeutic effect is that it shuts down the function of the entire pilosebaceous unit and apocrine secretions, preventing the rupture and spread of follicular material through the dermis, which usually results in more inflammation and formation of the sinus tract.17
Patient A, treated with 250 U of Dysport® in both armpits, presented condition improvement attributed to reducing apocrine sweat, thus decreasing the tendency of follicular rupture. The study didn’t report how the dilution was made. The technique used was similar to that of hyperhidrosis, but the remission period was ten months, superior to that of hyperhidrosis – 6 to 8 months.19
Patient B received 40 U of Botox®, distributed in 10 to 12 intradermal points in the groin. No dilution was described. She had complete remission within six months, responding satisfactorily to a second treatment. BTXA therapy can be a safe, well-tolerated, and effective method for young patients who develop mild to moderate HS, refractory to other therapies.
Patient C received 50 U of BTXA in each axilla (100 U diluted in 4 ml of 0.9% SS). The study didn’t report the technique used. She presented clinical remission after the second treatment and periodically continued to perform the toxin application.
Patient D underwent application of 100 U of Botox® in the groin and thighs and 130 U in the buttocks. Neither technique nor dilution was reported. She presented a complete resolution of the symptoms for three months but required subsequent treatments (five treatments of 200 U), with intervals of four months. Nevertheless, the patient developed infectious exacerbation demanding surgical treatment.
Patient E received 400 U of BTXA, 100 U in each area: right/left inframammary and right/left axilla. The dilution was 100 U of toxin in 2 ml saline solution, and the technique used intradermal injection in parallel lines with a distance of 1 cm between the points. At each point, 0.1 ml of the dilution was injected. Here, we obtained the first complete description of the doses, dilution, and technique. The patient obtained an excellent response to treatment beyond pain relief. Shi et al. also reported that subsequent applications with lower BTXA dosages (50 U per area) led to a faster return of symptoms, resuming the higher doses. The authors pointed out that BTXA seems to work best in the inflammatory state of the disease and that the toxin can be an economical treatment for HS, even in the Hurley III.10
Patient F underwent application of 50 U of Vistabex® in each axilla, in a technique similar to that of axillary hyperhidrosis (50 U diluted in 2.5 ml 0.9% SS). Each 1.5 cm² square received 4 U. Patient G received 100 U of Botox® in each groin, with the same dilution and technique described above. In both, efficacy was similar to hyperhidrosis treatment (6-12 months) with a slow recovery from the disease.
It is worth mentioning that most of the off-label uses of BTXA are for chronic diseases. However, a question remains: how long can we use this treatment in patients with HS without risks or sequelae? We found that all patients needed subsequent doses to control the disease better. Another topic to be discussed is that the botulinum toxin has an immunogenic potential related to the dose injected and injection frequency. Therefore, it is reasonable to extend the application intervals by balancing the dose with the expected duration of the clinical effect. A well-defined dosage regimen is required, as well as injection and dilution techniques for standardization of these protocols.
BTXA is a new and promising treatment option. Further research is needed to understand its role in HS management, including optimal dosing and administration frequency. Patients are likely to need more than one treatment over time, as lesions tend to recur after an average of six to ten months. The technique used has been the standard one for hyperhidrosis.
It is a safe, well-tolerated, and effective method for young patients who develop mild to moderate HS without improvement after several therapeutic modalities. Also, it offers the possibility to perform a treatment dedicated to some patients providing minimal, reproducible adverse events over time without loss of effectiveness, in addition to reducing pain.
Elcilane Gomes Silva 0000-0001-8841-2285
Preparation and writing of the manuscript; data collection, analysis, and interpretation.
Juliana Joyce Chaves de Lima 0000-0002-9971-5908
Preparation and writing of the manuscript; data collection, analysis, and interpretation.
Natalia Pantoja Costa 0000-0002-3454-6760
Author’s contribution: Preparation and writing of the manuscript; data collection, analysis, and interpretation.
1. Alikhan A, Lynch PJ, Eisen DB. Hidradenitis suppurativa: a comprehensive review. J Am Acad Dermatol. 2009;60(4):539-61.
2. Jemec GBE. Clinical practice. Hidradenitis suppurativa. N Engl J Med. 2012;366(2):158-64.
3. Napolitano M, Megna M, Timoshchuk EA, Patruno C, Balato N, Fabbrocini G, et al. Hidradenitis suppurativa: froma pathogenesis to diagnosis and treatment. Clin Cosmet Investig Dermatol. 2017;10:105-15.
4. Van der Zee HH, Laman JD, Boer J, Prens EP. Hidradenitis suppurativa: viewpoint on clinical phenotyping, pathogenesis and novel treatments. Exp Dermatol. 2012;21(10):735-39.
5. Campanati A, Martina E, Giuliodori K, Bobyr I, Consales V, Offidani A. Two cases of Hidradenitis suppurativa and botulinum toxin type a therapy: A novel approach for a pathology that is still difficult to manage. Dermatol Ther. 2019;32(3):e12841.
6. Vazquez BG, Alikhan A, Weaver AL, Wetter DA, Davis MD. Incidence of hidradenitis suppurativa and associated factors: a population-based study of Olmsted County, Minnesota. J Invest Dermatol. 2013;133(1):97-103.
7. Pink AE, Simpson MA, Desai N, Trembath RC, Barker JNW. Gamma-secretase mutations in hidradenitis suppurativa: new insights into disease pathogenesis. J Invest Dermatol. 2013;133(3):601-7.
8. Frew JW, Vekic DA, Woods J, Cains GD. A systematic review and critical evaluation of reported pathogenic sequence variants in hidradenitis suppurativa. Br J Dermatol. 2017;177(4):987-98.
9. Hessam S, Sand M, Gambichler T, Skrygan M, Ruddel I, Bechara FG. Interleukin-36 in hidradenitis suppurativa: evidence for a distinctive proinflammatory role and a key factor in the development of aninflammatory loop. Br J Dermatol. 2018;178(3):761-7.
10. Shi W, Schultz S, Strouse A, Gater DR. Successful treatment of stage III hidradenitis suppurativawith botulinum toxin A. Br J Dermatol Case Rep. 2019;12(1):e226064.
11. Canoui-Poitrine F, Le Thuaut A, Revuz JE, Viallette C, Gabison G, Poli F, et al. Identification of three hidradenitis suppurativa phenotypes: latent class analysis of a cross- sectional study. J Invest Dermatol. 2013;133(6):1506-11.
12. Kurek A, Peters EM, Chanwangpong A, Sabat R, Sterry W, Schneider- Burrus S. Profound disturbances of sexual health in patients with acne inversa. J Am Acad Dermatol. 2012;67(3):422-8.
13. Onderdijk AJ, van der Zee HH, Esmann S, Lophaven S, Dufour DN, Jemec GB, et al. Depression in patients with hidradenitis suppurativa. J Eur Acad Dermatol Venereol. 2013;27(4):473-8.
14. Muzy G, Crocco EI, Alves RO. Hidradenite supurativa: atualização e revisão de suas modalidades terapêuticas. Surg Cosmet Dermatol. 2014;6(3):206-12.
15. Sartorius K, Emtestam L, Jemec GB, Lapins J. Objective scoring of hidradenitis suppurativareflecting the role of tobacco smoking and obesity. Br J Dermatol. 2009;161(4):831-9.
16. Reilly DJ, Munasinghe CP, Nizzero DE. Botulinum toxin A for the management of hidradenitis suppurativa. Plast Surg Case Studies. 2015;1(1):3-4.
17. Campanati A, Martina E, Giuliodori K, Consales V, Bobyr I, Offidani A. Botulinum toxin Off-Label use in dermatology: a review. Skin Appendage Disord. 2017;3(1):39-56.
18. Khoo ABS, Burova EP. Hidradenitis suppurativa treated with clostridium botulinum toxin A. Clin Exp Dermatol. 2014;39(6):749-50.
19. O'Reilly DJ, Pleat JM, Richards AM. Treatment of hidradenitis suppurativa with botulinum toxin A. Plast Reconstr Surg. 2005;116(5):1575-6.
20. Feito-Rodriguez M, Sendagorta-Cudos E, Herranz-Pinto P, de Lucas-Laguna R. Prepubertal hidradenitis suppurativa successfully treated with botulinum toxin A. Am Soc Dermatol Surg. 2009; 35(8):1300-2.
21. Matusiak L, Bieniek A, Szepietowski JC. Bacteriology of hidradenitis suppurativa - Which antibiotics are the treatment of choice? Acta Derm Venereol. 2014;94(6):699-702.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}