


Cleide Garbelini-Lima; Gabriela Evangelista de Almeida; Talita Fernandes Picanço e Souza; Alcidarta dos Reis Gadelha; Ilner de Souza e Souza
Received on: 04/10/2020
Approved on: 09/02/2021
Financial support: None
Conflict of interest: None
Study conducted at the Tropical Medicine Foundation Dr. Heitor Vieira Dourado, Manaus (AM), Brazil
Case study of exceptional response to treatment of recurrent xanthelasma palpebrarum with an ablative laser. The patient underwent a single session of laser Erbium: Yttrium-aluminum-garnet (Fotona®) 2940 nm, and we performed photographic records with Vectra® H2 2019 before and after the procedure. Satisfactory clinical results were reported, with good pain tolerability and early recovery compared to surgical procedures and, consequently, less time away from work activities.
Keywords: Lasers; Laser therapy; Laser coagulation; Xanthelasma palpebraum
Xanthelasma palpebrarum (XP) is a benign disease of the eyelid and periorbital region.1 Yellowish and thin polygonal papules and plaques characterize the condition, occurring most commonly in the area near the medial corner of the upper eyelid. Lesions can be single or multiple and, in the latter case, tend to be symmetrical.2,3
The condition belongs to the group of xanthomas, and it is the most common cutaneous presentation. It may also involve the neck, trunk, shoulders, and armpits.3 The disease most commonly affects the elderly, with a preference for women.4
The exact pathogenic mechanism is not fully understood. Still, it is known that cutaneous xanthelasma represents the deposition of fibroproliferative connective tissue associated with lipid histiocytes, also known as foam cells.
Histologically, foam cells are typically found in the middle, superficial, and perianexial dermis, and they are associated with fibrosis and inflammation. There is no association between xanthelasmas and levels of high-density lipoprotein or triglycerides. 3
XP is typically asymptomatic, with no reports of skin complications. However, due to aesthetic dissatisfaction and psychological damage, it must be treated effectively.
Literature frequently cites as treatments the application of topical trichloroacetic acid (TAC) 50% and 70%, surgical excision, and laser ablation. Scientific evidence is limited regarding the most effective treatment.3 Adverse events, such as ectropion, post-inflammatory hypo or hyperpigmentation, infection, and healing defects, are possible, depending on the technique chosen, in addition to a high recurrence rate.
The ablative laser is a therapy targeted for XP. The proposed mechanism of action is perivascular foam cells destruction by thermal damage and dermal vessel coagulation. It blocks the lipids leakage into the tissue, thus preventing recurrence. The literature describes different types of lasers, including carbon dioxide (CO2), argon, Erbium (Er), and pulsed dye.3
The Erbium:yttrium-aluminum-garnet laser (Er: YAG) is purely ablative,3 with a wavelength of 2940nm. It has a high affinity with tissue water and can remove thin skin layers guaranteeing minimal thermal damage. Also, it allows precise ablation of the tissue in delicate places, with excellent depth control. Because it is not very invasive, it minimizes the adverse events of the treatment.
In this study, we report a case of XP recurrent after surgical excision that presented a satisfactory result with just one session of Er:YAG laser, with minimal peri and postoperative discomfort, rapid healing, less time away from daily activities, and better aesthetic outcomes than those presented in the previous treatment.
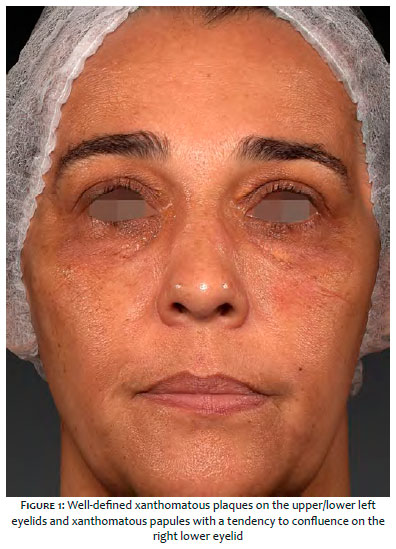
A 51-year-old woman, married, Fitzpatrick skin phototype IV, presented yellowish plaques, with bipolar location, for approximately 14 years. She denied previous comorbidities and illnesses or similar family conditions. The physical examination revealed a xanthomatous plaque of approximately 2 cm in its largest diameter on the upper eyelid and about 1.2 cm in its largest diameter on the lower eyelid, both in the left eye, in addition to xanthomatous papules with a tendency to confluence in the lower eyelid of the right eye (Figure 1). The patient reported having undergone two previous surgical corrections. The laboratory tests presented a slight increase in total cholesterol levels (232 gm/dL). After obtaining the informed consent, the patient received lesion treatment with the Er:YAG 555 laser (Fotona® Dallas, Texas) in benign lesions mode, with a wavelength of 2940nm, energy of 5J, delivery speed of 7 Hz, and 3 mm tip. The patient underwent a single session with excellent pain tolerance based on the use of a topical anesthetic of tetracaine 3.5% associated with lidocaine10%, carried on a transdermal basis with a pre-procedure action time of 30 minutes.
Serial photographs were taken: before the procedure (Figure 2), seven days after the procedure (Figure 3), and two months after the procedure (Figure 4). Records were made with the Vectra® H2 2019 equipment. There was complete regression of the lesions and healing in 20 days, with mild hypochromia, shorter time interval, and better recovery compared to previous surgical procedures, as well as a lower risk of perioperative and postoperative bleeding. There was a significant improvement in quality of life assessed by the DLQI (Dermatology Life Quality Index) questionnaire.
From a cutaneous point of view, XP is, in most cases, a purely aesthetic problem. Thus, the therapies used for its treatment must cause minimal adverse events.
Surgical excision always leaves a scar, although it is often discreet. However, postoperative complications such as infections, bleeding, and unsightly scars can occur. The CO2 laser removes xanthelasmas in a cosmetically acceptable way. However, it creates a comparatively deeper zone of temperature and damage associated with postoperative erythema persisting for months.4
The Er:YAG 2940nm laser has an extremely high absorption by the water contained in the tissue and can ablate thin layers of skin in the range of a few nanometers ensuring minimum thermal damage.4 It allows precise ablation and dermal extrusion of aggregated esterified cholesterol, dermal remodeling, and excellent depth control.5 In addition, it has a smaller thermal coagulation zone compared to the CO2 laser.
Er:YAG laser also has the advantage of faster healing, less erythema, and less post-inflammatory dyschromia.3
In a clinical trial with 15 patients, Borelli and Kaudewitz4 concluded that Er:YAG 2940nm is effective in the xanthelasma treatment, causing minimal adverse events with no recurrences in the follow-up period that ranged from seven to 12 months.
Abdelkader and Alashry5 demonstrated that Er:YAG is more effective than Q-switched neodymium:yttrium aluminum garnet (QSNd:YAG) laser in treating XP lesions, in addition to having less unsightly adverse events.
Er:YAG laser represents an effective method for the XP treatment, causing less pain discomfort and allowing the use of only topical anesthetic. Also, there is no need for suturing and, consequently, better healing with less time away from work activities.
Cleide Garbelini-Lima | 0000-0002-8840-7635
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Gabriela Evangelista de Almeida | 0000-0002-8437-2842
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Talita Fernandes Picanço e Souza | 0000-0001-7423-5820
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Alcidarta dos Reis Gadelha | 0000-0002-1194-7545
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Ilner de Souza e Souza | 0000-0001-6125-2832
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Al Aboud AM, Al Aboud DM. Xanthelasma palpebrarum. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2020.
2. Nguyen AH, Vaudreuil AM, Huerter CJ. Systematic review of laser therapy in xanthelasma palpebrarum. Int J Dermatol. 2017;56(3):e47-e55.
3. Laftah Z, Al-Niaimi F. Xanthelasma: an update on treatment modalities. J Cutan Aesthet Surg 2018;11:1-6.
4. Borelli C, Kaudewitz P. Xanthelasma palpebrarum: treatment with the erbium:YAG laser. Lasers Surg Med. 2001;29(3):260-64.
5. Abdelkader M, Alashry SE. Argon laser versus erbium:YAG laser in the treatment of xanthelasma palpebrarum. Saudi J Ophthalmol. 2015;29(2):116-20.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}