


Bruna de Souza Felix Bravo1; Julien Totti de Bastos2; Kedima Caldeira Nassif3
Received on: 20/01/2020
Approved on: 24/02/2021
Financial support: None
Conflict of interest: None
Study conducted at the Hospital Federal da Lagoa, Rio de Janeiro (RJ), Brazil
INTRODUCTION: One of the most feared complications when using facial fillers is the potential risk of intravascular injection. Therefore, all applicators must be aware of the treatment algorithm in the case of ischemia.
OBJECTIVE: This article reports a case of lip ischemia after filling with hyaluronic acid, completely reversed only after the use of warm compresses.
METHODS: Use of warm compresses in case of lip ischemia.
RESULTS: Complete reversibility of ischemia.
CONCLUSIONS: Despite not being the only measure to be adopted in an ischemia condition after hyaluronic acid filling, this case demonstrates the value of using warm compresses, which in the present report was sufficient to revert the condition.
Keywords: Cosmetic techniques; Hyaluronic acid; Lip
The human face has a rich vascular network Its numerous collateral arteries and the presence of anastomoses between vascular territories make it a potentially dangerous environment for the use of facial fillers due to the risk of ischemia.1
Ischemia induced by injection of fillers is a rare but feared consequence and usually occurs due to injecting the product directly into an artery. However, it can also result from compression or vascular injury.
The immediate diagnosis and early treatment are essential for the satisfactory resolution of the problem.2,3
This article reports a case of late ischemia after lip filling, resolved only with the use of local heat applied by the patient at home and complete reversal of the condition, verified on the patient's return to the office for the continuity of the treatment algorithm.
A 29-year-old woman performed lip filling for aesthetic purposes in a dermatologic office. She was healthy, with no known comorbidities or allergies.
Topical anesthesia was performed with lidocaine 30 minutes before the procedure, followed by cleaning with alcoholic chlorhexidine. The product was applied with a 30G needle, with 1.5 ml of hyaluronic acid (Juvederm vollift - Allergan) in the lip contour and vermilion. Before the injection, an aspiration test was performed for seven seconds, negative on all points. The patient reported no pain during the application. At the end of the procedure, no pain and no evident clinical signs of ischemia were observed. She was instructed to take prednisone 40 mg daily for three days, maintaining the follow-up.
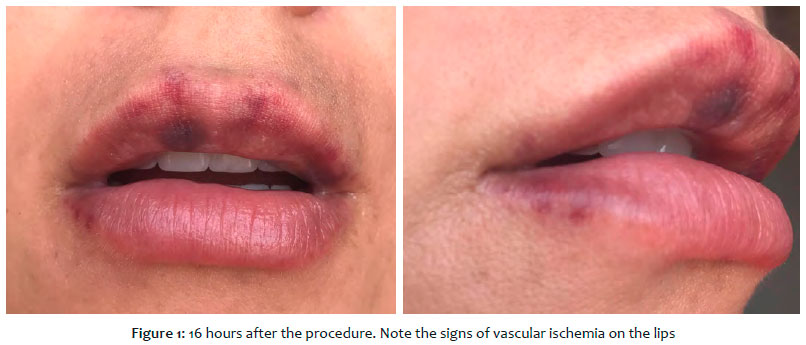
The next day, 16 hours after the procedure, the patient informed that she was feeling well, with no pain, and forwarded photos for evaluation showing the presence of signs suggestive of vascular occlusion (Figure 1). The patient’s immediate presence at the clinic was requested, and she was instructed to put warm compresses and massage the area until she arrived at the clinic. After 10 minutes of warm compresses, the patient sent new photos demonstrating a critical reversal of the process (Figure 2).
The image sent by the patient 16 hours after the procedure shows clear signs of vascular ischemia on the lips. Comparatively, after the warm compresses, it’s possible to note the improvement in ischemic signs (Figure 3).
The patient was assessed in person, for three consecutive days, with no clinical changes.
No other treatment was performed, such as the use of hyaluronidase or anticoagulants.
The vascular anatomy of the face is complex, and doctors who apply facial fillers must be familiar with it. The professional should also quickly recognize the signs and symptoms of an ischemic condition and keep in mind the recommended management in these cases.
The initial presentation of embolic vascular events is the presence of momentary whitening, which can last only a few seconds (sometimes it is even absent). It progresses to livedo reticularis (which can last up to a few days), blistering (which usually appears on the third day), crusts, necrosis, sloughing, and, finally, healing by secondary intention – a process that can take six weeks or more.3,4 A slow capillary recharge time (the regular time is from one to two seconds) associated with skin sensitivity to touch can alert the presence of an ischemic condition.1 Symptoms may include pain and discomfort disproportionate to those typically experienced in conventional fillers. However, it is essential to note that newer fillers are composed of local anesthetics, changing the clinical picture in these cases.1,3
Depending on the inserted material’s nature and quantity, the product’s viscosity and cohesion, as well as the pressure applied at the injection time, different scenarios gravities are observed.1 If only a small amount is injected, the material may be deposited in a location where the guarantee of adjacent blood vessels still provides sufficient blood supply in such a way that no ischemic result occurs. The rich vascular network ignores the obstruction so entirely that the accident never manifests clinically.1
Therefore, in general, it is likely that the safest practice is to inject small product amounts (0.1 mL) into several areas.1,5 Other potential factors for intra-arterial injection would be the use of smaller, sharper needles and the presence of scars in the treatment area.1
Facing a case of vascular obstruction, it is necessary to follow the treatment protocol. Its onset time is decisive in the outcome success. After the first recognition of vascular impairment, warm compresses and massage on the site are recommended.
The local heat promotes vascular dilation, and the massage can help distribute the material as the pressure moves the plunger. The compress can be applied for five to ten minutes every 30-60 minutes, taking care not to cause skin burns.2,5
Hyaluronidase is a particular part of managing ischemic conditions since it is responsible for degrading injected hyaluronic acid (HA). Although a hypersensitivity reaction can rarely occur with the use of hyaluronidase (incidence of 1 in 1,000 patients), most articles do not recommend skin testing in cases of imminent necrosis. However, the attending physician must be prepared for the rare possibility of allergy and even the extreme possibility of anaphylaxis.2,6,7 According to consensus recommendations, in the case of imminent local necrosis, high doses of the enzyme (400 units or more per area) and an injection every 3 cm to 4 cm in the ischemic area (bleached, violet, or reticulated discoloration region) should be applied, followed by a massage. If no improvement is observed in 60 minutes, an additional three to four injection cycles should be performed.2,6,7,8
Aspirin administration (two 325 mg tablets a day for seven days) can be useful as an antiplatelet agent. Nitroglycerin paste at the site may promote vasodilation, but its use is controversial.2 Low molecular weight heparin and systemic prostaglandins have also been a clinical treatment to promote vasodilation.1,7 Although there are no studies with a significant number of patients yet, hyperbaric oxygen therapy seems to provide a better benefit when associated with treatment, especially in cases of severe necrosis or when the tissue has slowed healing. Hyperbaric oxygen can deliver oxygen deep within the skin and help keep oxygen-dependent tissues viable.1,2,7,9
When starting the measures early, the clinical outcomes are positive in most cases, with a complete reversal of ischemia and no sequelae.
In our case, as it is late ischemia, we opted to immediately guide the patient to apply local heat and massage and, as soon as possible, to attend the medical office to continue the therapeutic algorithm and hyaluronidase application.
The patient presented a complete resolution of the ischemic signs a few minutes after applying the compresses, to the authors’ surprise, and it was not necessary to follow the treatment protocol.
Knowledge of the location and distribution of the main vessels of the face is essential for clinicians involved in this type of work. The risk of ischemia is higher when large bolus injections of the product are sent more deeply into tissues for volume increase and when using needles.
The treatment starts with the event’s early diagnosis and must continue with the administration of warm compresses and gentle massage, together with the application of hyaluronidase and oral aspirin. In the authors’ experience, hyaluronidase is the most effective treatment and, therefore, should be the first measure applied in cases of suspected ischemia. After the recommended initial management, if ischemia is still present, the evidence suggests that hyperbaric oxygen therapy may benefit some patients.
All applicators must be aware of the vascular impairment therapeutic algorithm to avoid severe and potentially irreversible sequelae after ischemia.
Bruna de Souza Felix Bravo | 0000-0001-9692-7967
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Julien Totti de Bastos | 0000-0002-1885-8908
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Kedima Caldeira Nassif | 0000-0002-1016-5525
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. DeLorenzi C. Complications of injectable fillers, part 2: vascular complications. Aesthet Surg J. 2014;34(4):584-600. Epub 2014 Apr.
2. Cohen JL, Biesman BS, Dayan SH, DeLorenzi C, Lambros VS, Nestor MS, et al. Treatment of hyaluronic acid filler-induced impending necrosis with hyaluronidase: consensus recommendations. Aesthet Surg J. 2015;35(7):844-9. Epub 2015 May 10.
3. Loh KTD, Phoon YS, Phua V, Kapoor KM. Successfully managing impending skin necrosis following hyaluronic acid filler injection, using high-dose pulsed hyaluronidase. Plast Reconstr Surg Glob Open. 2018;6(2):e1639. eCollection 2018 Feb.
4. DeLorenzi C. New high dose pulsed hyaluronidase protocol for hyaluronic acid filler vascular adverse events. Aesthet Surg J. 2017;37(7):814-25.
5. Cohen JL. Understanding, avoiding, and managing dermal filler complications. Dermatol Surg. 2008;34 (Suppl 1):S92-9.
6. Balassiano LKA, Bravo BSF. Hyaluronidase: a necessity for any dermatologist applying injectable hyaluronic acid. Surg Cosmet Dermatol. 2014;6(4):338¬43.
7. Bravo BSF, Balassiano LKA, Rocha CRM, Padilha CBS, Torrado CM, Silva RT, et al. Necrosis after soft-tissue augmentation with hyaluronic acid. J Clin Aesthet Dermatol. 2015;8(12):42-7.
8. Landau M. Hyaluronidase caveats in treating filler complications. Dermatol Surg. 2015;41 (Suppl 1):S347-53.
9. Kim DW, Yoon ES, Ji YH, Park SH, Lee BI, Dhong ES. Vascular complications of hyaluronic acid fillers and the role of hyaluronidase in management. J Plast Reconstr Aesthet Surg. 2011;64(12):1590-5. Epub 2011 Jul 31.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}